
Korea 2026 pollen allergies are setting records no prior season can match — and climate change is the reason why. Climate change is quietly reshaping one of the most common conditions on earth: allergic rhinitis. Pollen seasons are starting earlier, lasting longer, and producing far higher allergen loads than they did a decade ago — and this shift is now measurable not just in data, but in overflowing ENT waiting rooms across the Northern Hemisphere. As an ENT specialist practicing in Seoul, Korea, I am writing this because 2026 is the year the numbers became impossible to ignore here: between April 1 and 16, Seoul’s cumulative pollen index reached 1,178 — compared to 277 during the same period in 2025, a 4.25-fold increase in a single year. (Dong-a Ilbo, 2026) Korea is one data point in a global pattern. If this season hasn’t arrived at full force in your city yet, the mechanisms described here almost certainly apply to where you live as well.

Why Is Korea’s Spring 2026 the Worst Pollen Season on Record?
1. The Urban Heat Island Effect: Seoul’s Streets Are Now a Pollen Factory
On April 12, Seoul’s daytime high crossed 20°C — and the pollen index spiked almost immediately. That is not a coincidence. Deciduous trees release pollen when temperature thresholds are crossed; the urban heat island effect means city streets cross those thresholds earlier and more sharply than surrounding areas. The dense tree canopy planted across Seoul over the past two decades now acts less like urban greenery and more like a distributed pollen-release network, while reduced wind circulation between buildings keeps airborne particles suspended longer.
2. Climate Change Has Lengthened the Season Itself
April 2026 Lancet Countdown report confirmed that climate change has extended allergenic pollen seasons in Europe by 1-2 weeks compared to the 1990s (The Lancet Countdown Europe, 2026). Rising temperatures accelerate plant growth cycles, increase total pollen output per tree, and shift the peak window earlier in the calendar. Korea’s pollen calendar, maintained by the National Institute of Meteorological Sciences, already documents that birch (Betula) and oak (Quercus) — the two primary spring allergens — now peak across Seoul and surrounding regions in April and May, a window that continues to expand.
3. The Patient Pool Has Grown by 18% in Two Years
Korea’s allergic rhinitis patient population grew from 4.91 million in 2021 to approximately 5.8 million in 2023 — an 18% increase in two years (Health Insurance Review and Assessment Service [HIRA], 2023; National Health Insurance Service [NHIS], 2023). When a larger sensitized population encounters a fourfold spike in pollen load, the clinical impact compounds. Patients who managed well on their usual medication regimen in previous seasons may find that the same dose no longer controls symptoms at 2026’s pollen concentrations.
What Is Happening Inside Your Nose Right Now
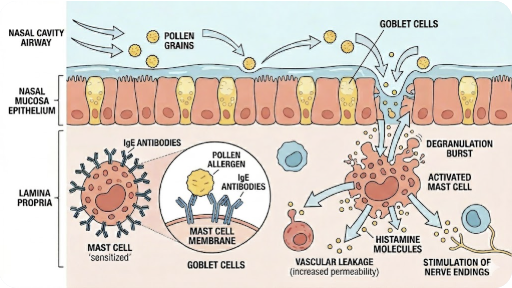
When birch or oak pollen contacts the nasal mucosa, it binds to IgE antibodies on mast cells, triggering degranulation and the release of histamine, leukotrienes, and prostaglandins. The result: sneezing, watery discharge, nasal congestion, and itching — the classic early-phase response. If exposure is sustained, eosinophils accumulate in the mucosa over 4–8 hours, reinforcing the inflammatory cycle (late-phase response).
From an ENT perspective, two downstream complications matter most and are often missed in general health advice.
Sinusitis. Sustained mucosal edema can block the ostiomeatal complex — the narrow drainage pathway connecting the sinuses to the nasal cavity. When the sinuses can’t drain, pressure builds, bacteria or fungi can colonize the retained secretions, and allergic rhinitis transitions into acute or chronic sinusitis. Signs: facial pressure, pain above the eyebrows or under the cheeks, thick discolored discharge.
Otitis media with effusion (OME). The Eustachian tube regulates middle ear pressure by opening briefly during swallowing. Nasal mucosal swelling impairs Eustachian tube function, causing fluid to accumulate in the middle ear. Signs: ear fullness, muffled hearing, or a sensation of water in the ear. These symptoms deserve ENT evaluation — not a wait-and-see approach.
The ENT Specialist’s Response Plan
Part A — Avoidance: Timing Is Everything
Outdoor pollen concentrations peak between 5:00 and 10:00 a.m. — shift exercise and outdoor activities to late afternoon or evening. On high-pollen days
- Wear a KF94 mask outdoors. Pollen grains measure 15–50 µm; a well-fitted KF94 blocks them effectively.
- Keep windows closed, especially in the morning. Use HEPA-filtered air purifiers indoors.
- After returning home: change clothes, shower, and irrigate your nasal passages with saline before sitting down.
These measures will not eliminate exposure in a season this extreme, but they reduce allergen load — and every reduction matters when the baseline is 4× above normal.
Part B — Pharmacotherapy
Primary Treatments
Antihistamines
Antihistamines block H1 receptors and are effective for sneezing, itching, and watery discharge — but they are less effective for nasal congestion, which is mediated largely by leukotrienes rather than histamine alone. Second- or third-generation antihistamines are preferred over first-generation: they are non-sedating or minimally sedating, provide once-daily dosing, and do not carry the anticholinergic side effects (dry mouth, urinary retention, QT prolongation risk) of older agents. For best effect, antihistamines should be taken 2–5 hours before anticipated exposure — they are pharmacological antagonists, meaning they compete with histamine but cannot reverse tissue changes that have already occurred. Specific drug selection should be guided by your physician or pharmacist.
Intranasal Corticosteroids (INCS)
This is the single most effective class of medication for allergic rhinitis, as confirmed by the ARIA (Allergic Rhinitis and its Impact on Asthma) 2016 guidelines [Brozek JL et al., J Allergy Clin Immunol, 2017]. INCS suppress the entire inflammatory cascade at the mucosal level — histamine, leukotrienes, prostaglandins, and cytokines — making them superior to antihistamines for nasal congestion and comparable or superior for all other symptoms. Key practical points:
- Full effect takes 5–7 days to develop. Start at least one week before pollen season peaks (ideally before April in Seoul).
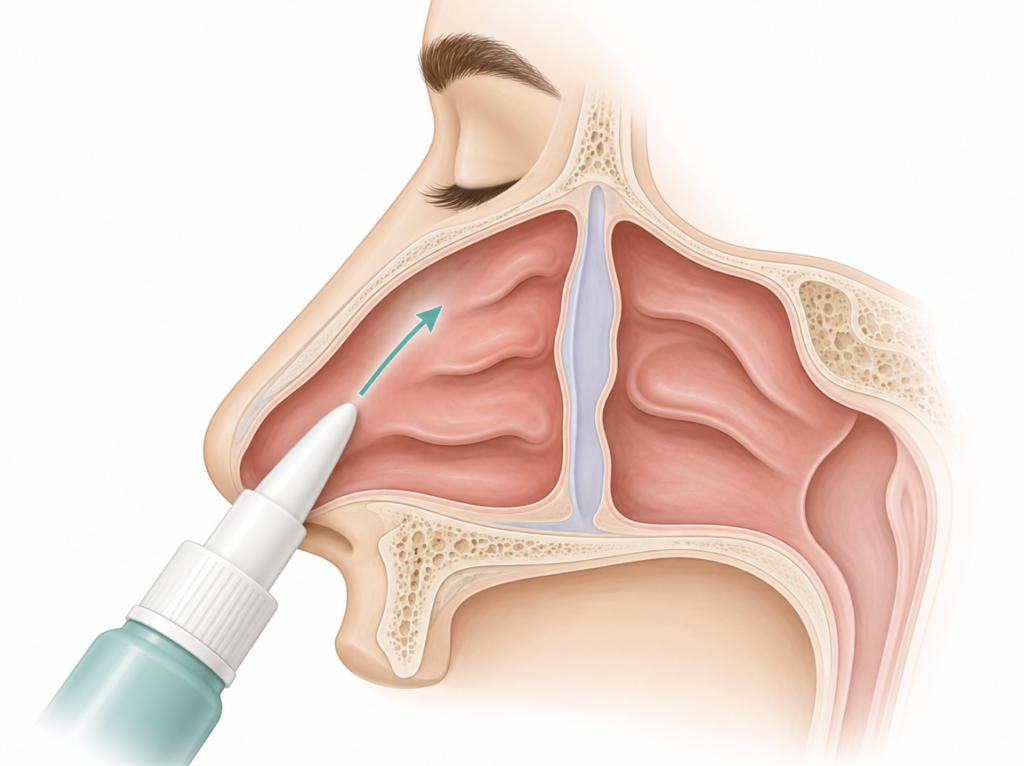
- Spray in the evening: most patients experience peak symptoms in the morning, so evening dosing provides maximum effect at the right time.
- Direct the spray away from the nasal septum (toward the outer eye on the same side) to reduce risk of nosebleeds and septal irritation.
- Second- and third-generation INCS have minimal systemic absorption (<2%) and are safe for long-term use in adults and children.
- If congestion is severe enough that the spray cannot reach the mucosa, a short course of a decongestant to open the airway first — then begin INCS — is a reasonable clinical approach.
Optional and Add-On Treatments
Anti-leukotriene agents (LTRA)
Leukotrienes are particularly important in the late-phase inflammatory response and in nasal congestion. LTRA can be a useful add-on — or primary agent — for patients with comorbid asthma or exercise-induced respiratory symptoms alongside allergic rhinitis, as the ARIA guidelines specifically recommend in this population. One important caution: the FDA issued a 2020 warning about neuropsychiatric adverse events (anxiety, depression, suicidal ideation) with a specific agent in this class, restricting its use in allergic rhinitis to cases where other medications are inadequate. Prescribing decisions must involve a physician.
Decongestants
Decongestants produce rapid vasoconstriction of nasal mucosal vessels, clearing congestion within minutes. They come in two forms:
- Topical (nasal spray): Fast and potent, but do not use for more than 3–7 days. Prolonged use downregulates α-adrenergic receptors, causing rebound congestion worse than the original — a condition called rhinitis medicamentosa. Appropriate for short-term relief during the worst days of the season, or as a pre-treatment to allow INCS to reach congested mucosa.
- Oral: Less prone to rebound congestion, but with systemic sympathomimetic effects (elevated blood pressure, insomnia, palpitations). ARIA guidelines recommend limiting use to 5 days or fewer in combination with other agents for severe congestion. Not recommended for children under school age, and use should be avoided in patients with hypertension, cardiac arrhythmia, or thyroid disease.
Saline nasal irrigation
This is not just a folk remedy. A 2018 Cochrane systematic review demonstrated that saline irrigation significantly reduces patient-reported allergic rhinitis severity and decreases medication use, with no adverse events reported [Head K et al., Cochrane Database Syst Rev, 2018]. The mechanism is straightforward: physically washing pollen, mucus, and inflammatory mediators off the mucosal surface, while improving mucociliary clearance. Isotonic (0.9%) saline is recommended; hypertonic solutions can irritate the mucosa and paradoxically worsen symptoms. Safe in pregnancy and for children. Think of it as a reset button you can use multiple times daily — especially after outdoor exposure.
Mast cell stabilizers
Mast cell stabilizers prevent histamine and leukotriene release from mast cells before degranulation occurs. Because they must be in place before allergen contact to work, they are most useful as preventive agents for patients who know when their season begins. Effect onset requires 1–2 weeks of consistent use. Efficacy is lower than INCS or antihistamines for established symptoms, making them a better fit for mild, early-season prophylaxis. They are among the safest options available — used in pregnancy and young children without known risk.
Intranasal anticholinergics
These agents target the cholinergic receptors driving mucus gland secretion. They are effective specifically for watery, profuse rhinorrhea that persists even after antihistamines and INCS have been optimized. They do not address nasal congestion, sneezing, or itching. Best used as an add-on in patients with refractory watery discharge.
Part C — Immunotherapy: Global Standard vs. Korean Reality
Allergen immunotherapy — administered as subcutaneous injections (SCIT) or sublingual tablets/drops (SLIT) — is the only treatment that modifies the underlying immune response rather than suppressing symptoms. Its efficacy for pollen allergy is well-established internationally. In the United States, the FDA has approved sublingual tablets for grass pollen (timothy grass) and ragweed, and subcutaneous immunotherapy (allergy shots) for a wide range of pollen allergens — including birch, oak, grass, and ragweed — is standard clinical practice, endorsed by the AAAAI/ACAAI guidelines and the AAO-HNS 2024 clinical practice guideline on immunotherapy. In Europe, both SLIT and SCIT for grass and birch pollen are mainstream, EMA-regulated treatment options backed by large randomized controlled trials (AAO-HNS, 2024; FDA, 2014)
In Korea, the clinical picture is different. Immunotherapy here is predominantly offered for house dust mite (HDM) allergic rhinitis, where standardized domestic and imported products are widely available and clinical infrastructure is well-developed. Pollen-specific immunotherapy products have more limited commercial availability and clinical experience in the Korean market. This gap is not a reflection of efficacy data — the evidence for pollen immunotherapy is robust — but of regulatory and market realities. If you are a reader in Europe or the US with confirmed pollen sensitization and inadequate symptom control, pollen immunotherapy is a legitimate option to discuss with your allergist or ENT specialist. For readers in Korea, allergen testing to identify your sensitization profile remains the right first step, after which your ENT specialist can advise on what is realistically available.
Part D — When to Come to the ENT Clinic
Do not wait through these symptoms:
| Symptom Pattern | What It May Signal |
|---|---|
| Symptoms persisting >2 weeks, no fever, recurring every spring | Allergic rhinitis requiring formal diagnosis and testing |
| Facial pressure, pain over sinuses, thick discolored discharge | Allergic rhinitis-triggered sinusitis |
| Ear fullness, muffled hearing, sensation of fluid in ear | Otitis media with effusion — Eustachian tube dysfunction |
| Sleep disruption due to congestion despite medication | Inadequate treatment; possible anatomical contributing factors |
Clinical Perspective: What an ENT Sees During a 4× Pollen Season
In a typical spring, a significant fraction of allergic rhinitis patients manage well enough with over-the-counter antihistamines and intermittent saline rinses. This season is not typical. What I am seeing clinically is a pattern I associate with sustained high-allergen load: patients arriving not just with classic rhinitis, but with the pressure and fullness that signals early sinusitis, and — more frequently than usual — with unilateral ear symptoms that turn out to be Eustachian tube dysfunction progressing toward effusion.
The common thread is delayed treatment escalation. Patients have been using the same antihistamine dose that worked last year, not realizing that a fourfold increase in pollen load requires a different first-line response — INCS, not antihistamines alone. The other pattern: patients who started INCS correctly but applied it incorrectly (spraying at the septum, inhaling too hard after spraying, expecting instant results), and concluded it wasn’t working after two days. Technique matters as much as drug selection.
My clinical recommendation this season: if you are already sensitized to spring pollen, begin INCS and saline irrigation before you become symptomatic. Treat this season as you would a known annual event — with advance preparation, not reactive scrambling.
Key Takeaways
- Korea’s 2026 cumulative pollen index (April 1–16: 1,178) is 4.25× higher than the same period in 2025 (277), driven by the urban heat island effect and climate-change-extended pollen seasons.
- Birch (Betula) and oak (Quercus) pollen are the dominant spring allergens in Korea, peaking in April–May; both are capable of triggering severe IgE-mediated nasal inflammation.
- Intranasal corticosteroids (INCS) are the most effective single agent for allergic rhinitis across all symptom domains and are recommended as first-line treatment for moderate-to-severe persistent disease by ARIA guidelines.
- Antihistamines are fast-acting and appropriate for mild intermittent disease; their effectiveness for nasal congestion is limited compared to INCS, because congestion is primarily leukotriene-mediated.
- Ear fullness or muffled hearing accompanying rhinitis symptoms need cautious attention — it may indicate Eustachian tube dysfunction or otitis media with effusion, requiring specialist evaluation.
FAQ
Is Korea’s 2026 pollen count really 4× higher than last year?
Yes. The Korea Meteorological Administration data shows the cumulative pollen index from April 1–16, 2026 reached 1,178, versus 277 during the same period in 2025 — a 4.25-fold increase, with the steepest rise occurring after April 12 as Seoul’s daytime temperatures climbed above 20°C.
Why are my allergies worse this spring even though I’m taking the same medication?
Because the allergen dose has quadrupled. Antihistamines work by competitive antagonism — they compete with histamine for receptor binding. At much higher pollen loads, more histamine is released, and the same antihistamine dose provides proportionally less coverage. If you have been managing with antihistamines alone, this season likely warrants adding an intranasal corticosteroid and consistent saline irrigation.
What is the difference between antihistamines and intranasal corticosteroids for allergic rhinitis?
Antihistamines block the effects of histamine specifically — effective for sneezing, itching, and runny nose, but limited for congestion. Intranasal corticosteroids suppress the entire inflammatory cascade at the mucosal level — effective across all four major nasal symptoms including congestion — and are the first-line recommendation for moderate-to-severe disease according to ARIA guidelines. They are not interchangeable; they work through different mechanisms and are often most effective in combination.
When should I see an ENT specialist for spring allergies?
Seek ENT evaluation if: symptoms persist beyond two weeks without fever; facial pressure or pain suggests possible sinusitis; ear fullness or hearing changes develop; or your symptoms are not adequately controlled despite appropriate pharmacotherapy. Formal allergen testing guides long-term management decisions.
Can immunotherapy treat pollen allergies — and does the answer differ by country?
Yes, and yes. In the US and Europe, immunotherapy for grass, birch, and ragweed pollen is a well-established, guideline-endorsed treatment — FDA-approved sublingual tablets exist for grass pollen in the US, and subcutaneous immunotherapy for multiple pollen types is standard clinical practice in both regions. In Korea, however, allergen immunotherapy is predominantly offered for house dust mite (HDM) allergic rhinitis, and pollen-specific immunotherapy has more limited product availability and clinical infrastructure. This reflects market and regulatory realities, not a lack of efficacy data. Readers in any country should discuss allergen testing with their ENT specialist as the first step.
A Final Thought: Medicine Is Entering a Climate Era
Climate change is touching every corner of our lives — and the practice of medicine is no exception. Allergic rhinitis is one of the first conditions where the signal is unmistakable: longer seasons, higher pollen loads, expanding geographic ranges of allergens, and a patient population that is growing faster than our management frameworks can keep pace with. But it will not be the last. Many diseases that once followed predictable seasonal or geographic patterns are beginning to shift — in timing, severity, and distribution. As patients, awareness and proactive management matter more than ever. As physicians, we must be willing to update our clinical intuitions and protocols as the baseline keeps changing. The numbers coming out of Korea this spring are not just a local story. They are a preview.
Joonpyo Hong, MD is a board-certified otolaryngologist practicing in Korea. This article reflects his clinical interpretation of published research and does not constitute individual medical advice.
References
The Lancet Countdown on Health and Climate Change. Europe report 2026: health and climate change in Europe. The Lancet Public Health. 2026.
Brozek JL, Bousquet J, Agache I, et al. Allergic Rhinitis and its Impact on Asthma (ARIA) guidelines: 2016 revision. J Allergy Clin Immunol. 2017;140(4):950-958.
Head K, Snidvongs K, Glew S, et al. Saline irrigation for allergic rhinitis. Cochrane Database Syst Rev. 2018;6(6):CD012597.
Rosenfeld RM, et al. Clinical Practice Guideline: Immunotherapy for Inhalant Allergy. Otolaryngol Head Neck Surg. 2024;170(suppl 2):S1-S36. Accessed May 2, 2026.
FDA. Grastek (timothy grass pollen allergen extract) [package insert]. Bridgewater, NJ: Merck; 2014.
Oh JW, Lee HB, Kang IJ, et al. The revised edition of Korean calendar for allergenic pollens. Allergy Asthma Immunol Res. 2012;4(1):5-11.
Jeong KY, Park JW. Allergens of regional importance in Korea. Front Allergy. 2022;2:652275.
Zhang K, Li AR, Miglani A, Nguyen SA, Schlosser RJ. Effect of medical therapy in allergic rhinitis: a systematic review and meta-analysis. Am J Rhinol Allergy. 2022;36(2):269-280.
Sources (News / Reports)
- Dong-a Ilbo. (2026, April 17). “Spring outing turns into sneezing: Citizens suffer from accelerated pollen dispersal”. faq.donga.com. https://faq.donga.com/NEWS/Society/article/all/20260417/133757552/1
- Health Insurance Review and Assessment Service. (2023). https://www.hira.or.kr/bbs/68/2024/01/BZ202401259554226.pdf
- Seoul Economic Daily. “Pollen Allergies Worsen as Spring Index Quadruples Year-on-Year.” April 20, 2026. https://en.sedaily.com/…
- Korea Meteorological Administration — Pollen Forecast Service. weather.go.kr
- Korean Society of Rhinology. Allergic Rhinitis Update, 4th ed. 2024. (Chapter 5: Avoidance Therapy; Chapter 6: Pharmacotherapy; Chapter 7: Immunotherapy)
For more interesting contents:
https://curiousmd.com/evolutionary-reason-for-allergies/
https://curiousmd.com/ai-allergy-forecast-personalized-prediction/
Link out to:
https://doi.org/10.1016/j.jaci.2017.03.050
https://doi.org/10.1002/14651858.CD012597.pub2
https://www.fda.gov/drugs/drug-safety-communications/fda-requires-boxed-warning-about-serious-mental-health-side-effects-asthma-and-allergy-drug