
Smartphone BPPV detection sounds implausible until you read the 2025 numbers: a Johns Hopkins pilot study reported 100% sensitivity and 100% specificity for positional nystagmus — using nothing but an iPhone in a dark room (Phillips et al., Digital Biomarkers, 2025). That sounds like the end of in-clinic Dix-Hallpike testing as we know it. It is not. But the gap between “in clinic” and “at home” just narrowed in a real way.
Most BPPV attacks are short and unpredictable. By the time the patient reaches the clinic, the spinning has often stopped and the nystagmus is gone, leaving the physician to interpret a story rather than an eye sign. Smartphone-based nystagmus capture is the first practical tool that lets the patient hand over the eye sign instead of the story. This article walks through what the new evidence actually shows, what apps are out there, and — most importantly — how to record video that is useful when the patient is too dizzy to think straight.
Why Recording Nystagmus Matters in BPPV
BPPV diagnosis hinges on a single observable sign: the characteristic nystagmus that appears within seconds of a provocative head position. Direction, latency, duration, and whether the nystagmus has a torsional component — all of these decide which canal is involved and which repositioning maneuver to use.

When a patient arrives symptom-free, the in-office Dix-Hallpike or supine roll test is used to provoke the nystagmus on the spot. That works for most posterior-canal BPPV. It works less well for atypical cases, intermittent symptoms, or patients whose attacks happen only at 3 a.m. when they roll over in bed. Capturing the eye movement during the actual attack — what neurologists call ictal nystagmus — fills that diagnostic blind spot.
What the 2025 Evidence of Smartphone BPPV Actually Shows
EyePhone — Johns Hopkins Pilot
Phillips and colleagues developed EyePhone, an iPhone-based eye-tracking app that uses the front camera with no external attachment. In a controlled clinical setting, the app correctly detected positional nystagmus with 100% sensitivity and 100% specificity during Dix-Hallpike and supine roll testing (Phillips et al., Digital Biomarkers, 2025). A companion paper showed that 95% of patient-recorded videos had clear eye visibility on expert review, and most participants said they would use the app again (Bastani et al., Digital Biomarkers, 2025).
These numbers are striking. They are also pilot numbers — small samples, controlled conditions, and a clinical environment. The headline figure is a research signal, not a regulatory claim.
Low-Cost Alternative: $25 IR Camera + 3D-Printed Goggles
A 2025 case report from a Japanese group used a commercially available mini-infrared camera (about US$25) mounted in 3D-printed goggles (about US$13) to record a patient’s nystagmus during a vertigo attack at home (Sakazaki et al., JMIR Formative Research, 2025). The recording allowed an offsite physician to diagnose lateral semicircular canal BPPV without an in-person visit. The setup is inelegant but it solves the smartphone’s biggest weakness: standard phone cameras need ambient light, and BPPV examination is best done in the dark.
Real-World Adherence: The Honest Number
A larger study from Maastricht had 62 patients try to record their own ictal nystagmus using a smartphone adapter (Nystagmocatcher, Balansdiagnos, Stockholm). Only 51% provided usable eye-movement recordings (Melliti et al., Journal of Neurology, 2023). The most common reasons for failure were that the attack never recurred during the study period, attacks were too brief, or — telling — patients found it too hard to operate the phone while spinning.
That 51% is the number to keep in mind. The technology works in principle. The patient experience is the bottleneck.
How to Actually Record Nystagmus at Home
This is the section most articles skip. A patient in the middle of a vertigo attack cannot calmly open an app, frame their face, and tap record. Here is what works.
1. Set Up Before the Attack, Not During It
If your attacks are predictable — first turn in bed, getting up at night, looking up to a high shelf — pre-stage the equipment beside the bed. The phone should already be in a stand or holder, the camera app already open, the screen brightness lowered, and the position you plan to record from already identified. Treating the recording as a single-button action is the difference between getting useful video and getting nothing.
2. Recruit a Helper
The best recordings come from a family member holding the phone, not from the patient holding it. A spouse, a parent, or an adult child needs only three pieces of instruction: hold the phone roughly 20 cm from the patient’s eyes, keep the phone steady, and start recording before the patient changes position. If you live alone, a tabletop tripod or gooseneck phone mount on the bedside table is the next-best option. A small tripod costs less than a single co-pay.
3. Get the Lighting Right
BPPV nystagmus, especially the torsional component, is hardest to see in bright light because the pupil constricts and there is less iris detail to track. Record in a dim room with a single low side lamp, or use a red-filtered light. Do not point a phone flashlight at the patient’s face; the glare washes out everything useful and induces blinking. If the room is too dark for a standard camera, the $25 infrared camera workaround above becomes worth the effort.
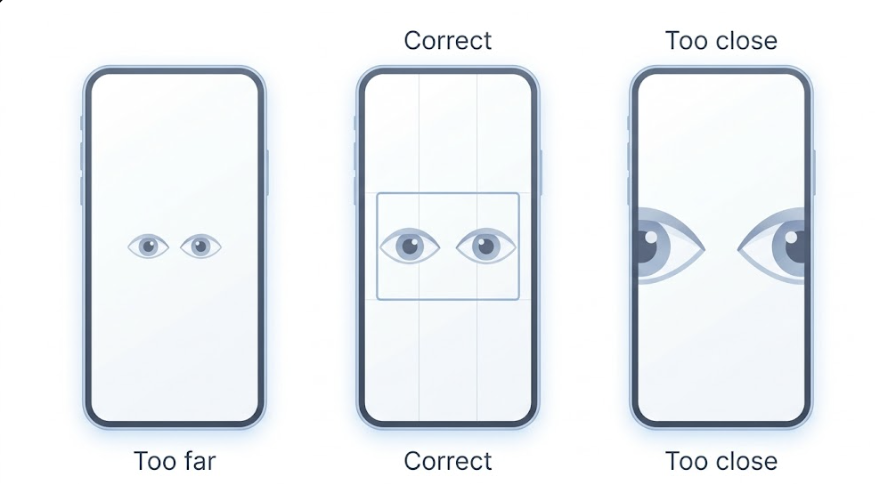
4. Frame the Eyes Properly
Aim for both eyes filling roughly the middle third of the screen. Too far and the eyes are pixelated; too close and the camera will not focus. Use the rear camera for unaided helper-assisted recording, since it is sharper than the front camera on most phones; if you are using a dedicated eye-tracking app like EyePhone, follow the app’s specified camera (typically the front camera). Remove glasses (the reflections will obscure the pupils). Push back any hair covering the eyes. Heavy eye makeup, particularly mascara on the lower lash line, can confuse pupil-tracking algorithms in apps like EyePhone.
5. Record the Right Movements for the Right Duration
For suspected posterior-canal BPPV, the most useful sequence is a Dix-Hallpike attempt: sit upright, then quickly lie back with the head turned 45 degrees and hanging slightly off the edge of the bed. Hold that position for at least 60 seconds while the camera records. Repeat to the other side. For suspected horizontal-canal BPPV, a supine roll test — lying flat, then turning the head fully to one side, then to the other — is more useful. Each position needs at least 60 seconds of footage because BPPV nystagmus has a latency of several seconds and then evolves.
Do not stop recording when the room stops spinning. The fading of the nystagmus is itself diagnostic information.
6. Send the Video Right Way
A WhatsApp or any SNS video sent at full resolution is fine for most clinical purposes. Avoid editing or trimming the file — your physician needs the timestamps and the whole arc, not the dramatic middle. If your clinic has a patient portal that accepts video upload, that is the most secure route. Send the file along with a brief note describing what you were doing when symptoms started and how long they lasted.

7. Common Reasons Recordings Fail
The Maastricht data (Melliti et al., 2023) and routine clinic experience converge on the same five culprits: the patient tried to hold the phone instead of pre-positioning it; the room was too bright or too dark; the recording was under 30 seconds; glasses or hair obscured the eyes; or the patient stopped the camera the moment they felt better, missing the directional reversal that distinguishes one canal from another.
Existing Apps Compared
| App / Device | Purpose | Diagnostic value | Availability |
|---|---|---|---|
| EyePhone | Eye tracking + nystagmus detection | Pilot-stage research data | Not publicly released |
| iCapNYS | Patient self-recording with gyro | Front-camera capture, clinical use | iOS app store |
| Nystagmocatcher | Smartphone optical adapter | Real-world adherence data published | Hardware purchase (Sweden) |
| BPPV Relief / DizzyFix | Maneuver guidance animations | Treatment aid, not diagnostic | App stores |
As of 2026, none of these is FDA-cleared as a standalone diagnostic device. The diagnostic-grade tools are in research; the publicly available apps are mostly maneuver tutors.
Clinical Perspective: An ENT’s Take
When a clinician receives a patient’s phone video, the first item to check is not the eye movement itself — it is the metadata. When was the video recorded? Was it during symptoms or hours after? A good recording during a real attack is worth more than three weeks of clinic visits between attacks. A blurry recording of an asymptomatic patient is worth almost nothing.
The second consideration is whether the recording captures the directional pattern over time. BPPV nystagmus has a signature shape — latency, crescendo, decrescendo, and often a directional reversal when the patient sits back up. A 10-second clip of nystagmus is suggestive. A 90-second clip showing the full envelope is diagnostic in many cases.
Where smartphone recordings genuinely change clinical management is in three situations: atypical attack patterns that cannot be reproduced in clinic; suspected horizontal-canal BPPV, where the side of the affected ear is hard to determine without watching the supine roll in real time; and follow-up after an Epley or Lempert maneuver to confirm resolution without another office visit.
Realistically, however, these devices are likely to be persuasive only to a narrow group: patients with frequently recurring BPPV who already understand the diagnostic difficulty firsthand. For a one-off vertigo episode, the setup cost — the holder, the dark room, the rehearsal — outweighs the benefit. For a patient on their fifth recurrence in two years, the same setup begins to look like a sound investment.
The medico-legal frame is straightforward. A phone video is documentation, not a diagnosis. The diagnosis still belongs to the clinician — and the responsibility for treatment decisions still belongs to the clinician.
Key Takeaways
- A 2025 Johns Hopkins pilot reported 100% sensitivity and specificity for smartphone detection of positional nystagmus, but the data are preliminary (Phillips et al., 2025).
- In real-world use, only about 51% of patients managed to provide usable ictal nystagmus recordings on their own (Melliti et al., 2023).
- Pre-staging the phone in a holder before symptoms start, and recruiting a family member, are the two single biggest predictors of a useful recording.
- Each position should be recorded for at least 60 seconds in a dimly lit room, with the eyes framed in the middle third of the screen.
- Smartphone video is a complement to clinical examination, not a replacement, and as of 2026 no consumer app is FDA-cleared as a diagnostic device.
Frequently Asked Questions
Q: Can a smartphone diagnose BPPV by itself?
A: No. Recent 2025 pilot studies show smartphone eye tracking can reliably detect the nystagmus that suggests BPPV, but a definitive diagnosis still requires interpretation by a physician familiar with positional testing. The video is evidence; the diagnosis is a clinical judgment.
Q: Which phone app is most accurate for vertigo recording?
A: As of 2026, no consumer app is FDA-cleared as a standalone diagnostic device. EyePhone has the strongest published feasibility data but is not publicly released. iCapNYS is available in the iOS app store and uses the front camera plus the phone's gyro. BPPV Relief and DizzyFix are designed to teach maneuvers, not to diagnose.
Q: How do I record nystagmus at home if I am too dizzy to hold the phone?
A: Pre-stage the phone in a tabletop stand or gooseneck holder beside your bed before symptoms start, and recruit a family member to start the recording for you. Hold each position for at least 60 seconds and keep the room dim. Trying to hold the phone while spinning is the most common reason recordings fail.
Q: Is it worth bringing a phone video to my ENT appointment?
A: Yes. Even a partial recording can give your physician real-time information they would otherwise miss, especially for atypical or intermittent symptoms. Send the original file unedited, along with a note about what you were doing when symptoms started.
References
- Phillips V, Bastani PB, Rieiro H, Hale DE, Otero-Millan J, Zee DS, Newman-Toker DE, Saber Tehrani A. A Pilot Study of Smartphone Eye Tracking for Detection of Positional Nystagmus. Digit Biomark. 2025;9(1):124-129.
- Bastani PB, Phillips V, Rieiro H, Otero-Millan J, Zee DS, Newman-Toker DE, Saber Tehrani A. Feasibility of Using Smartphone Eye Tracking for Self-Recording Positional Tests. Digit Biomark. 2025;9(1):98-110.
- Melliti A, Lucieer FMP, van Stiphout L, et al. Capturing nystagmus during vertigo attacks using a smartphone: adherence, characteristics, pearls and pitfalls. J Neurol. 2023;270(12):6044-6056.
- Sakazaki H, Imai T, Higashi-Shingai K, et al. Monitoring Nystagmus in a Patient With Vertigo Using a Commercial Mini-Infrared Camera and 3D Printer: Cost-Effectiveness Evaluation and Case Report. JMIR Form Res. 2025;9:e70015.
Joonpyo Hong, MD is a board-certified otolaryngologist practicing in Korea. This article reflects his clinical interpretation of published research and does not constitute individual medical advice.
For more interesting contents:
https://curiousmd.com/vestibular-neuritis/
https://curiousmd.com/room-spins-when-youre-drunk/
https://curiousmd.com/motion-sickness-aftereffects/
Link out to:
https://karger.com/dib/article/9/1/124/929483/A-Pilot-Study-of-Smartphone-Eye-Tracking-for
https://pubmed.ncbi.nlm.nih.gov/37610446/
https://formative.jmir.org/2025/1/e70015