
In June 2022, Justin Bieber posted a video to his 240 million Instagram followers showing the right side of his face completely frozen — one eye unblinking, one side of his smile gone. The culprit was not stress or a neurological accident. It was a virus that most of us caught as children, one that has been quietly waiting in our nerve cells ever since. Ramsay Hunt syndrome is rare, frequently misdiagnosed, and — if treated late — can leave permanent marks on the face. This article covers what it is, who it affects, how it differs from Bell’s palsy, and what can be done to prevent it.
What Is Ramsay Hunt Syndrome?
Ramsay Hunt syndrome (RHS) — also called herpes zoster oticus with facial palsy — occurs when the varicella-zoster virus (VZV) reactivates specifically within the geniculate ganglion of the facial nerve (cranial nerve VII). It is the second most common cause of peripheral facial palsy after Bell’s palsy, accounting for roughly 12% of all facial nerve paralysis cases [Sweeney, “Ramsay Hunt syndrome,” 2001].
The Classic Triad
The textbook presentation consists of three findings occurring together on the same side of the face:
- Facial nerve palsy — weakness or complete paralysis of one side of the face
- Otalgia — severe, often excruciating ear pain
- Herpetic vesicles — fluid-filled blisters on or around the ear canal, pinna, or soft palate
Beyond the facial nerve, VZV reactivation frequently extends to cranial nerve VIII, producing sensorineural hearing loss, tinnitus, and vertigo in a meaningful proportion of patients [Monsanto, “Treatment and prognosis of facial palsy on Ramsay Hunt syndrome,” 2016]. This multi-nerve involvement is one of the features that sets RHS apart from a straightforward facial palsy.
A subtler variant — zoster sine herpete — presents with facial palsy and ear pain but no visible vesicles. This form is the hardest to diagnose and the most likely to be misclassified as Bell’s palsy.
The Virus Behind It: Chickenpox, Shingles, and RHS
To understand RHS, it helps to trace the full lifecycle of VZV.
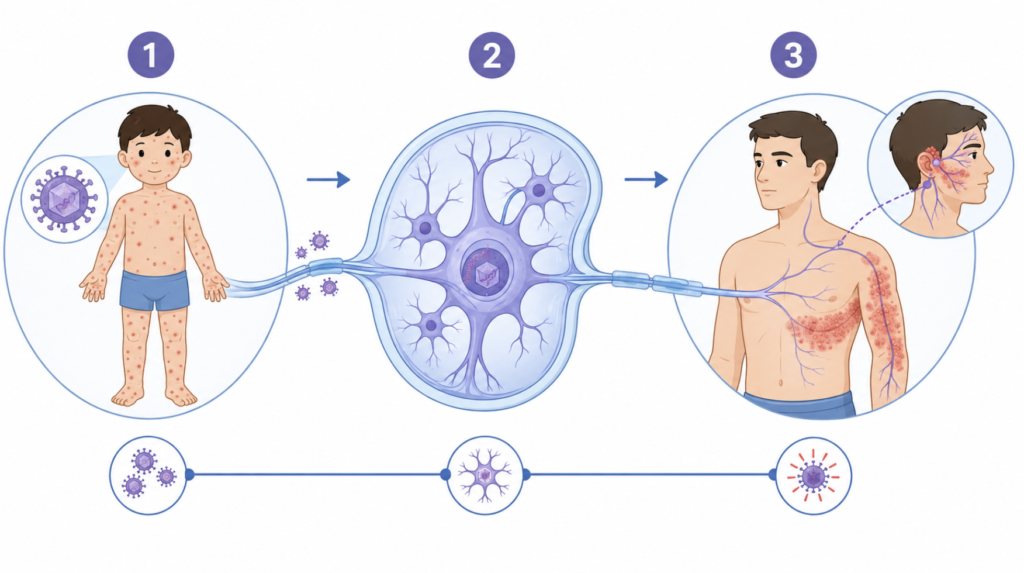
Chickenpox (varicella) is the primary infection, typically in childhood. The virus spreads systemically, producing the characteristic diffuse, itchy rash. The immune system eventually suppresses it — but never fully clears it. VZV retreats into the dorsal root ganglia and cranial nerve ganglia (part of our nerves, to put it simply), where it lies dormant, sometimes for decades.
Shingles (herpes zoster) occurs when immunity wanes and VZV reactivates. Unlike chickenpox, shingles is unilateral and follows a single dermatome (which means a specific skin area innervated by a single nerve) — a band of skin innervated by the affected nerve. Pain and vesicles appear together along that nerve’s path.
Ramsay Hunt syndrome is herpes zoster of the geniculate ganglion — a specific reactivation site within the facial nerve. When VZV wakes up here, the consequences reach beyond a simple skin rash. The facial nerve swells within its narrow bony canal, and the result is the paralysis, pain, and vesicles that define RHS. It is not a separate disease from shingles — it is shingles in a particularly consequential location.
| Condition | Trigger | Distribution | Facial Nerve Involvement |
|---|---|---|---|
| Chickenpox | Primary VZV infection | Diffuse, whole body | No |
| Shingles | VZV reactivation | Single dermatome, unilateral | Only if CN V/VII affected |
| Ramsay Hunt Syndrome | VZV reactivation in geniculate ganglion | pinna, auditory canal, eardrum | Yes — primary feature |
Prognosis: Does Severity at Onset Predict Recovery?
The short answer is yes — significantly. The House-Brackmann grading scale (I = normal, VI = complete paralysis) at presentation is known to be one of the strongest predictors of long-term outcome.
In a systematic review of RHS outcomes, patients who began treatment within 72 hours of symptom onset and presented with incomplete palsy had good recovery rates exceeding 80%. Among those with complete paralysis (House-Brackmann Grade V–VI) at onset, only around 51% ultimately achieved a favorable recovery grade, even with prompt treatment [Monsanto, “Treatment and prognosis of facial palsy on Ramsay Hunt syndrome,” 2016].
Overall, RHS carries a worse prognosis than Bell’s palsy. Compared to Bell’s palsy patients, RHS patients tend to be younger, present with more severe initial paralysis, and recover less completely [Murakami, “Treatment of Ramsay Hunt syndrome with acyclovir-prednisone,” 1997]. Sequelae — including synkinesis (involuntary co-movements of facial muscles), crocodile tears (tearing while eating), and postherpetic neuralgia — occur more frequently in RHS than in Bell’s palsy.
Clinical Perspective “The 72-hour window is not a soft guideline — it is the difference between most patients recovering well and many not. When a patient arrives on day 5 with complete palsy and asks about their chances, that is one of the harder conversations in outpatient ENT. Severity at presentation and time to treatment are the two variables that should be focused on immediately.”
When Famous Faces Froze: Celebrity Cases
Justin Bieber (2022)
On June 10, 2022, Bieber posted a now-viral video explaining that RHS had caused complete right-sided facial palsy. He showed the camera his unblinking eye and immobile half-smile, saying: “This eye is not blinking… I can’t smile on this side of my face.” The Justice World Tour was cancelled for several months, and Bieber recovered gradually over the following year. His public disclosure triggered a measurable global spike in searches for “Ramsay Hunt syndrome” — a phenomenon subsequently studied in a peer-reviewed paper examining how celebrity diagnoses influence public health awareness [Kasprowicz, “Impact on online research on celebrities’ uncommon diseases,” 2023].
Senator Dianne Feinstein (2023)
At age 89, Senator Feinstein was diagnosed with shingles complicated by Ramsay Hunt syndrome, causing an extended absence from the U.S. Senate. Her case illustrated the more severe clinical course seen in elderly patients, in whom immune senescence allows more aggressive VZV reactivation and limits recovery potential.
Together, these two cases — one young adult, one elderly — reflect the full spectrum of RHS presentations. Age and immune status are the major modifiers of how this disease behaves.
Ramsay Hunt Syndrome vs. Bell’s Palsy: The Critical Difference
Both RHS and Bell’s palsy cause unilateral peripheral facial palsy, and both can look identical on initial examination — particularly in zoster sine herpete, where no vesicles appear. Understanding the differences matters clinically because the prognosis and management diverge.
| Feature | Bell’s Palsy | Ramsay Hunt Syndrome |
|---|---|---|
| Cause | Unknown (HSV reactivation presumed) | VZV reactivation in geniculate ganglion (suspected) |
| Ear pain / vesicles | Absent | Present (pathognomonic when present) |
| CN VIII involvement | Rare | Common — hearing loss, vertigo |
| Spontaneous recovery (no treatment) | ~71%* | Lower |
| Prognosis with treatment | Generally good | More guarded |
| Role of surgery | Considered in selected severe, rapidly progressing cases | Not routinely recommended |
*Tiemstra JD, Khatkhate N. Bell’s palsy: diagnosis and management. Am Fam Physician. 2007;76(7):997-1002.
Surgery: A Tale of Two Diagnoses
This is one of the most clinically important distinctions between the two conditions.
For Bell’s palsy, facial nerve decompression — via middle fossa approach or transmastoid approach depending on CT findings — has a defined, if narrow, role. The classic indication is severe, rapidly progressing paralysis with electroneurography (ENoG) showing greater than 90–95% neural degeneration within the first one to two weeks of onset. In this subset, surgical decompression of the labyrinthine segment (or any segment of swollen facial nerve) might improve recovery outcomes [Gantz, “Surgical management of Bell’s palsy,” 1999].
For Ramsay Hunt syndrome, the picture is different. Studies examining facial nerve decompression in RHS show inconsistent results, and no established guidelines recommend it as a standard intervention. The evidence base is insufficient to justify routine surgery, and most centers — particularly outside of specialized settings — do not offer it. RHS is managed medically, not surgically.

Prevention: Can You Stop RHS Before It Starts?
The Shingles Vaccine
The most effective prevention strategy is the recombinant zoster vaccine (Shingrix). In the landmark ZOE-50 trial, Shingrix demonstrated 97.2% efficacy against herpes zoster in adults aged 50 and older [Lal, “Efficacy of an adjuvanted herpes zoster subunit vaccine in older adults,” 2015]. In adults aged 70 and older, efficacy remained at 91.3% [Cunningham, “Efficacy of the herpes zoster subunit vaccine in adults 70 years of age or older,” 2016]. By reducing overall shingles incidence, Shingrix proportionally lowers the risk of RHS — though it does not eliminate it entirely.
The vaccine is given as two intramuscular doses, with the second dose administered two to six months after the first. It is currently recommended for immunocompetent adults aged 50 and over, as well as immunocompromised adults aged 19 and over.
The childhood varicella vaccine provides additional downstream protection: by preventing primary VZV infection, it reduces the lifetime pool of latent virus available to reactivate.
Other Prevention Considerations
There is no guaranteed method to prevent VZV reactivation beyond vaccination. Known triggers include immunosuppression from medications (corticosteroids, chemotherapy), untreated HIV, and severe physiological stress. Optimizing immune health — treating underlying conditions, avoiding prolonged immunosuppression where possible — reduces reactivation risk. These are general principles, not substitutes for vaccination.
Treatment
The 72-Hour Window
The cornerstone of RHS treatment is early combined antiviral and corticosteroid therapy. Treatment initiated within 72 hours of symptom onset produces the best outcomes. After this window, effectiveness diminishes, though treatment is still warranted.
- Antivirals: Acyclovir or valacyclovir are the agents of choice. Valacyclovir offers superior oral bioavailability and is often preferred in clinical practice.
- Corticosteroids: Methylprednisolone has shown higher recovery rates than prednisone or prednisolone in comparative analyses — 81.3% versus 69.2% and 61.4% respectively [Monsanto, “Treatment and prognosis of facial palsy on Ramsay Hunt syndrome,” 2016].
Supportive Care
Eye protection is non-negotiable in any patient with incomplete eye closure. Corneal exposure keratopathy — drying and ulceration of the cornea due to incomplete blinking — is a serious and preventable complication. Lubricating eyedrops during the day, ophthalmic ointment at night, and eye taping while sleeping are standard measures.
Postherpetic neuralgia — pain persisting beyond the acute phase — may require additional management with gabapentinoids or tricyclic antidepressants. Vestibular rehabilitation is useful when vertigo is prominent. Facial physical therapy helps prevent synkinesis and restore muscle balance once the nerve begins to recover.
Surgery — Not Recommended for RHS
As noted above, facial nerve decompression is not a standard treatment for Ramsay Hunt syndrome. Published literature examining decompression in RHS shows mixed and generally unimpressive results; no major guideline body currently endorses it as a routine intervention. Medical management remains the standard of care.
Key Takeaways
- Ramsay Hunt syndrome is caused by VZV reactivation in the geniculate ganglion of the facial nerve — the same virus responsible for chickenpox and shingles.
- The classic triad is unilateral facial palsy, ear pain, and herpetic vesicles near the ear; cranial nerve VIII involvement (hearing loss, vertigo) is common.
- Initial palsy severity predicts recovery: complete paralysis at onset carries only about a 51% chance of good recovery even with treatment.
- Treatment with antivirals plus corticosteroids must begin within 72 hours of onset for best results.
- Surgical facial nerve decompression is not routinely recommended for RHS — unlike Bell’s palsy, where decompression has a defined role in severe, rapidly progressing cases meeting specific ENoG criteria.
- Shingrix vaccine reduces shingles risk by 97% in adults aged 50 and older with healthy immune systems. It also lowers postherpetic neuralgia risk by 91% in this group
FAQ
Is Ramsay Hunt syndrome the same as Bell’s palsy? No. Both cause unilateral facial palsy, but they differ in cause, severity, and prognosis. Bell’s palsy has an unknown cause (possibly viral, presumed HSV-1 or VZV), no vesicles, and generally better outcomes. RHS is caused by confirmed VZV reactivation in the facial nerve ganglion, typically presents with ear pain and vesicles, and carries a worse prognosis overall.
Will I fully recover from Ramsay Hunt syndrome? Recovery depends heavily on two factors: how severe the paralysis was at onset and how quickly treatment was started. With prompt treatment and incomplete initial palsy, the majority of patients do well. With complete paralysis at onset, full recovery occurs in roughly half of patients. Some degree of synkinesis or residual weakness is not uncommon.
Can young people get Ramsay Hunt syndrome? Yes. Anyone who has had chickenpox carries latent VZV and can develop RHS at any age if the virus reactivates. Justin Bieber was 28 at the time of his diagnosis. Reactivation is more common with advancing age and immune suppression, but young adults are not immune.
Does the shingles vaccine prevent Ramsay Hunt syndrome? The Shingrix vaccine does not specifically target RHS, but by preventing shingles broadly, it reduces the risk of RHS. Efficacy is over 97% against shingles in adults 50 and older. It does not provide 100% protection.
What happens if Ramsay Hunt syndrome is left untreated? Untreated RHS carries a significantly higher risk of permanent facial weakness, persistent pain (postherpetic neuralgia), and long-term hearing loss. The viral inflammation continues unchecked, causing greater nerve damage. Early treatment is the single most important factor in determining outcome.
Joonpyo Hong, MD is a board-certified otolaryngologist practicing in Korea. This article reflects his clinical interpretation of published research and does not constitute individual medical advice.
References
- Sweeney CJ, Gilden DH. Ramsay Hunt syndrome. J Neurol Neurosurg Psychiatry. 2001;71(2):149-154.
- Murakami S, Hato N, Horiuchi J, Honda N, Gyo K, Yanagihara N. Treatment of Ramsay Hunt syndrome with acyclovir-prednisone: significance of early diagnosis and treatment. Ann Neurol. 1997;41(3):353-357.
- Monsanto RD, Bittencourt AG, Neto NJ, Beilke MA, Lorenzetti FT, Salomone R. Treatment and prognosis of facial palsy on Ramsay Hunt syndrome: results based on a review of the literature. Int Arch Otorhinolaryngol. 2016;20(4):394-400.
- Lal H, Cunningham AL, Godeaux O, Chlibek R, Diez-Domingo J, Hwang SJ, et al. Efficacy of an adjuvanted herpes zoster subunit vaccine in older adults. N Engl J Med. 2015;372(22):2087-2096.
- Cunningham AL, Lal H, Kovac M, Chlibek R, Hwang SJ, Díez-Domingo J, et al. Efficacy of the herpes zoster subunit vaccine in adults 70 years of age or older. N Engl J Med. 2016;375(11):1019-1032.
- Gantz BJ, Rubinstein JT, Gidley P, Woodworth GG. Surgical management of Bell’s palsy. Laryngoscope. 1999;109(8):1177-1188.
- Kasprowicz M, Kasprowicz K, Guzik P. Impact on online research on celebrities’ uncommon diseases: the curious case of Justin Bieber and Ramsay Hunt syndrome. J Public Health (Berl). 2023;31(4):609-613.
- Tiemstra JD, Khatkhate N. Bell’s palsy: diagnosis and management. Am Fam Physician. 2007;76(7):997-1002.
For more interesting contents:
https://curiousmd.com/duchenne-smile-vs-fake-smile/
https://curiousmd.com/shingles-vaccine-and-hearing-loss/
Link out to:
https://www.cdc.gov/shingles/vaccines/index.html
https://www.nejm.org/doi/full/10.1056/NEJMoa1501184
https://jnnp.bmj.com/content/71/2/149