Cotton swabs in your ears: are they harmful or not? If they are harmful, why? No boring old medical script.
A 29-year-old man presented with sudden hearing loss, fullness, and tinnitus after trying to retrieve a stuck cotton swab from his own ear. On exam, his incus — the second of three middle-ear bones — was protruding through his tympanic membrane. He needed tympanoplasty with ossicular chain reconstruction to recover his hearing [Gutiérrez Pérez ML, Management of Incus Dislocation From Attempted Foreign Body Removal With Alligator Forceps, 2025].
Everyone has heard that cotton swabs don’t belong in ears. Most people still use them. The reason isn’t ignorance — it’s that the four arguments people give back actually sound reasonable. Each one deserves a careful look at the evidence.
The Baseline
The American Academy of Otolaryngology–Head and Neck Surgery’s 2017 clinical practice guideline is explicit: clinicians should strongly advise against putting cotton-tipped swabs or other objects into the ear canal [Schwartz SR, Clinical Practice Guideline (Update): Earwax (Cerumen Impaction), 2017]. The American Academy of Family Physicians’ updated review reaches the same conclusion [Horton GA, Cerumen Management: An Updated Clinical Review and Evidence-Based Approach for Primary Care Physicians, 2020].
The ears are self-cleaning. Cerumen forms in the outer two-thirds of the canal and migrates outward through epithelial migration — the skin of the canal slowly moves laterally, aided by jaw motion during chewing and talking [Schwartz SR, 2017]. Cerumen itself is protective: slightly acidic, antimicrobial, and effective at trapping debris. It also functions as a natural lubricant for the thin canal skin.
The scale of harm is not theoretical. Between 1990 and 2010, an estimated 263,338 U.S. children under 18 were treated in emergency departments for cotton-tip applicator–related ear injuries — about 34 per day [Ameen ZS, Pediatric Cotton-Tip Applicator-Related Ear Injury Treated in United States Emergency Departments, 1990-2010, 2017]. Foreign body sensation, tympanic membrane perforation, and soft tissue injury were the most common diagnoses.
Now to the four arguments.
Counter-Argument 1: “But My Earwax Is the Sticky Kind”
Wet, dark, sticky earwax is real, and the assumption is that it doesn’t migrate out on its own, so it must be manually removed. The assumption has two problems.
First, wet versus dry earwax is determined by a single single nucleotide polymorphism in the ABCC11 gene [Yoshiura K, A SNP in the ABCC11 Gene Is the Determinant of Human Earwax Type, 2006]. The “dry” allele (A) is highly prevalent in East Asia — frequencies of 80–95% in Chinese and Korean populations, with some studies reporting up to 99% — and rare elsewhere. Most patients of East Asian descent who feel they have “sticky earwax stuck in there” do not actually have wet-type cerumen. What they usually have is dry cerumen that became sticky through one of two mechanisms.
The first mechanism is mechanical: water enters the canal during a shower, the canal is then probed with a cotton swab, and the swab pushes the now-hydrated dry wax inward where it congeals into a moist plug. The second mechanism is inflammatory: repeated swab use causes microabrasions and low-grade canal irritation, producing serous exudate (weeping fluid) that mixes with dry cerumen and turns it tacky. In both scenarios, the patient experiences “sticky earwax” and interprets it as a personal trait, when it is actually a created problem.
Second, even genuine wet-type cerumen still migrates outward. It dries as it moves laterally and exits the canal naturally. The AAFP guideline does not distinguish wet from dry earwax in its management recommendation. For symptomatic impaction — wet or dry — the recommended interventions are cerumenolytic drops (mineral oil, baby oil, saline, hydrogen peroxide), irrigation, or manual removal by a clinician [Horton GA, 2020]. Cotton swabs appear nowhere in that list.
The ear canal has an hourglass-like narrowing called the isthmus, located about 5 mm from the tympanic membrane. A cotton swab against sticky wax doesn’t remove it — it compacts it into that narrowing. What was a soft, mobile lump becomes a dense plug pressed against the bony portion of the canal.
Counter-Argument 2: “I Only Use One After a Shower”
Of all the times to use a cotton swab, just after a shower is the worst.
Otitis externa — swimmer’s ear — has two principal risk factors, and the major one is the combination of water in the ear canal plus microtrauma. Water disrupts the skin–cerumen barrier and soften the canal lining; microabrasions from a cotton swab become entry points for Pseudomonas and Staphylococcus species [Hobson JC, Use and Abuse of Cotton Buds, 2005].
A single use is enough to start this. The thin keratin layer of the canal can be disrupted in one pass. Once it’s open, the wet environment finishes the job.
A cotton swab is also poor at removing water. The cotton tip absorbs some moisture from the outer canal, but it doesn’t reach the bony portion deeper in, where most of the trapped water actually sits. Worse, the wet cotton pushes residual water medially as it advances.
What actually works: tilt the head so the affected ear faces down and let gravity drain it, pat the auricle (outer ear) with a towel, and if needed use a hair dryer on low heat held about 30 cm away from the ear.
Counter-Argument 3: “I Only Clean the Part I Can See”
This is the most reasonable-sounding counter-argument, and it’s where the anatomy is most revealing. Two problems sit underneath it: most people’s definition of “the part I can see” is wrong, and even if it were right, a cotton swab cannot actually clean what they’re trying to clean.
The visible part is the auricle and concha — not the canal entrance. In a mirror, the pinna and the bowl-shaped concha are visible. The inside of the external auditory canal is not. Standard otoscopic examination technique requires grasping the auricle and pulling it upward, backward, and away from the head to mechanically straighten the canal enough to see the eardrum. If a trained examiner needs to manipulate the auricle with an otoscope to gain a line of sight, a casual user with a cotton swab is, by definition, working blind once the cotton tip crosses the canal entrance.
The canal is not a straight tube. The external auditory canal in adults is approximately 2.5 cm long and forms an italic S-curve, with two natural narrowings — one at the bony-cartilaginous junction and the isthmus about 5 mm from the eardrum [Schwartz SR, 2017]. The outer one-third is cartilaginous and somewhat flexible; the inner two-thirds is bony, with skin only a few cell layers thick directly adherent to periosteum.
This geometry means that a straight, rigid cotton swab cannot actually clean the inside of the ear canal. The swab enters horizontally, meets the first bend in the cartilaginous portion, and either presses against the canal wall at that bend or slides along one wall pushing wax inward. It cannot conform to the S-curve and sweep wax outward from the bony portion. The cotton tip’s shape and the swab’s rigidity together make it geometrically incapable of doing what it appears to do.
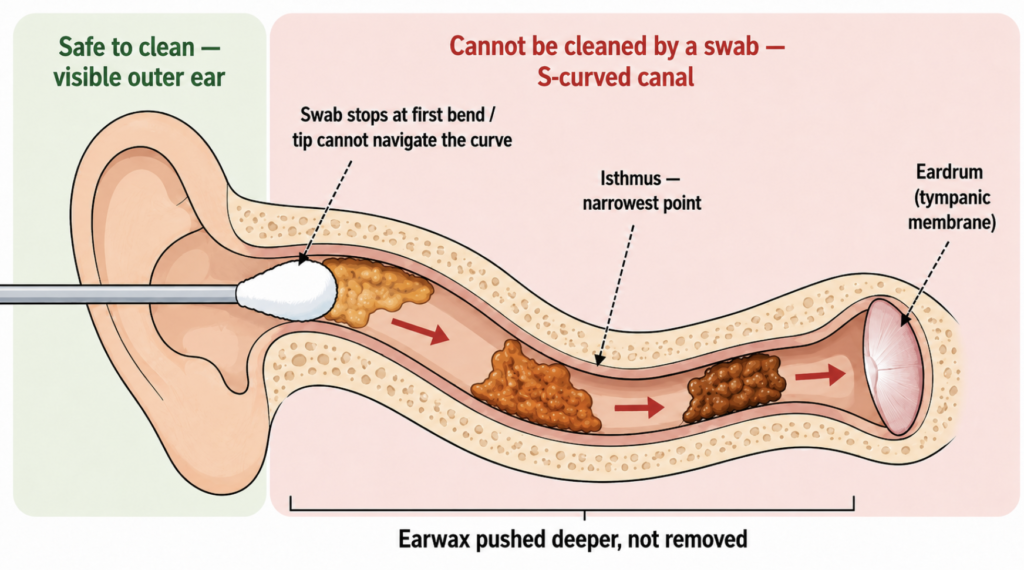
In practice, what cotton swab use does is: remove a thin smear of cerumen from the canal entrance, deposit fragments of cotton fiber further in, and push the rest of the wax deeper. The wax that comes out on the cotton is the wax that was already migrating out on its own.
The working rule: if the cotton tip disappears from view, it is no longer cleaning — it is pushing.
Counter-Argument 4: “I Wear Earphones for Hours and I’m Fine”
This argument has two flaws stacked on top of each other.
First, “I’m fine” is survivorship bias. A 2024 cross-sectional study of 130 adults in Central India compared 65 heavy earphone users with 65 non-users. Among earphone users, 18.5% had impacted cerumen, 9.2% had otomycosis (fungal canal infection), and 12.3% had otitis externa. In non-users the rates were 13.8%, 3.1%, and 3.1% respectively [Ghosh Moulic A, A Study of Hearing Acuity and the Health of the External Auditory Canal Among Earphone Users in Central India, 2024]. Overall, 40% of earphone users had some canal abnormality versus 20% of non-users — twice the baseline rate. Hearing loss was present in 69% of users versus 17% of non-users. The conclusion isn’t that earphones are safe; it’s that roughly two in five regular users develop a canal problem they may attribute to something else.
Second, the mechanism is different. Earphones cause passive harm: occlusion of the canal entrance, trapped moisture and heat, microbial transfer from a contaminated device, and contact dermatitis. The injury, when it happens, stays in the cartilaginous portion near the canal entrance. Cotton swabs cause active mechanical harm: direct abrasion of the canal wall, deep penetration past the cartilaginous-bony junction, and the possibility of striking the eardrum or ossicles. The bony portion of the canal has skin only a few cell layers thick, with no protective subcutaneous tissue [Schwartz SR, 2017].
The two devices do not reach the same anatomy. Earphones do not perforate eardrums. Cotton swabs are a leading cause of penetrating tympanic membrane perforation [Carniol ET, Traumatic Tympanic Membrane Perforations Diagnosed in Emergency Departments, 2018].
Clinical Perspective: The Itch-Scratch Cycle
Clinically, the patients who feel most strongly that they need to clean their own ears are often the ones who already have a cotton-swab–dependent cycle established. The mechanism is well-described in the otolaryngology literature: repeated swab use strips the canal of cerumen, which is both a physical barrier and a natural oil coating for the canal skin. Without this lubricating film, the canal skin becomes dry and pruritic. Scratching with a swab provides momentary relief but causes further microtrauma, stimulates histamine release, and triggers more cerumen production. The patient feels fullness, swabs more, and any new wax gets pushed inward against the isthmus. The brief relief from each swab reinforces the habit.
Breaking the cycle does not require better swab technique — it requires a complete pause combined with active replacement of the lost lubrication. A reasonable approach: stop all cotton swab use, and instill 2–3 drops of sweet oil (olive oil) into the canal two to three times daily for one to two weeks. The oil restores the lubricating barrier that swab use removed, controls the dryness-driven itch, and softens any compacted wax so it can migrate out naturally. For patients with severe itching that does not respond to oil alone, a short course of a topical low-potency steroid (such as 1% hydrocortisone otic preparation) can be considered, but this should be prescribed and supervised by a clinician after the canal has been examined.
Most patients find the itch and fullness resolve within two to three weeks once the cycle is broken and the canal re-establishes its barrier. The two genuine indications for clinician-led ear cleaning are symptomatic impaction (hearing loss, pain, fullness, tinnitus, dizziness) and the need to examine the eardrum.
Key Takeaways
- The external ear canal is self-cleaning; cerumen is a protective and lubricating substance, not waste.
- Wet versus dry earwax does not change the recommendation — both are managed without cotton swabs. In East Asian patients, most “sticky earwax” is actually dry cerumen mixed with water or inflammatory exudate from prior swab use.
- The S-curve of the canal means a straight cotton swab cannot reach or clean the inner canal; it only pushes wax inward.
- The most harmful time to use a cotton swab is immediately after a shower, when the canal is wet and the keratin barrier is softened.
- The cycle of “swab → dry, itchy canal → more swabbing” is broken by stopping swab use entirely and replacing the lost lubricant with sweet oil drops for one to two weeks.
FAQ
Can I use a cotton swab on the outside of my ear?
Yes — the auricle and the bowl of the concha (the visible outer ear) are safe to wipe with a cotton swab or a soft towel. The rule applies once the cotton tip enters the canal opening.
My ears feel wet after a shower. What should I do instead of a cotton swab?
Tilt your head so the affected ear faces down, gently pull the auricle up and back to straighten the canal, and let gravity drain. Pat the outer ear with a towel. If needed, use a hair dryer on low heat held about 30 cm away.
What if I’m certain my earwax is actually impacted?
First, the safety prerequisite: home softening is only appropriate if you have never had ear surgery, a perforated eardrum, ear tubes, or current ear pain or drainage. If any of these apply, see an otolaryngologist directly rather than self-treating. Otherwise, soften the wax with a few drops of mineral oil, baby oil, or saline once daily for three to five days, then let it work its way out. If symptoms persist — hearing loss, pain, fullness, tinnitus — see an otolaryngologist for microscopic removal.
Is it safer if my partner or parent does it for me?
No. In the U.S. pediatric injury data, parents handled the cotton swab in 16% of all swab-related ear injuries; among children under 4, parents were involved in nearly 80% of cleaning-related injuries [Ameen ZS, 2017]. Another person cannot see into the canal any better than the patient can.
My ear canal feels itchy all the time. How do I stop?
Itch in the canal is most often a result of cotton swab use stripping away the protective oil layer, not a sign that more cleaning is needed. Stopping all swab use and instilling 2–3 drops of sweet oil (olive oil) into the canal two to three times daily for one to two weeks usually restores the barrier and relieves the itch. If itching persists beyond that, see an otolaryngologist to exclude eczema, fungal infection, or other canal pathology.
How often should healthy adults have their ears cleaned?
For most people, never. People who wear hearing aids, have narrow ear canals, or have a history of impaction may benefit from a clinic visit every 6–12 months [Schwartz SR, 2017].
References
- Schwartz SR, Magit AE, Rosenfeld RM, et al. Clinical Practice Guideline (Update): Earwax (Cerumen Impaction). Otolaryngol Head Neck Surg. 2017 Jan;156(1_suppl):S1–S29.
- Ameen ZS, Chounthirath T, Smith GA, Jatana KR. Pediatric Cotton-Tip Applicator-Related Ear Injury Treated in United States Emergency Departments, 1990-2010. J Pediatr. 2017 Jun;185:202–207.
- Horton GA, Simpson MTW, Beyea MM, Beyea JA. Cerumen Management: An Updated Clinical Review and Evidence-Based Approach for Primary Care Physicians. J Prim Care Community Health. 2020;11:2150132720904181.
- Yoshiura K, Kinoshita A, Ishida T, et al. A SNP in the ABCC11 Gene Is the Determinant of Human Earwax Type. Nat Genet. 2006 Mar;38(3):324–330.
- Gutiérrez Pérez ML, Vahidi R, Kani N, Shohet JA, Djalilian HR. Management of Incus Dislocation From Attempted Foreign Body Removal With Alligator Forceps. Ear Nose Throat J. 2025.
- Ghosh Moulic A, Deshmukh P, Jain S, et al. A Study of Hearing Acuity and the Health of the External Auditory Canal Among Earphone Users in Central India. Cureus. 2024 Sep 18;16(9):e69664.
- Hobson JC, Lavy JA. Use and Abuse of Cotton Buds. J R Soc Med. 2005 Aug;98(8):360–361.
- Carniol ET, Bresler A, Shaigany K, et al. Traumatic Tympanic Membrane Perforations Diagnosed in Emergency Departments. JAMA Otolaryngol Head Neck Surg. 2018 Feb;144(2):136–139.
Joonpyo Hong, MD is a board-certified otolaryngologist practicing in Korea. This article reflects his clinical interpretation of published research and does not constitute individual medical advice.