
A patient comes in convinced something is crawling in their ear. It itches relentlessly, feels blocked, and in its pure form, barely hurts. However, if the canal is scratched raw or a bacterial infection joins in, it can turn quite painful. Under the microscope, the answer appears: a fuzzy white mat studded with tiny black dots, like pepper sprinkled on cotton wool. This is otomycosis, a fungal infection of the ear canal, and the colors you see inside the ear are one of the first clues to what is growing there.
This article walks through what otomycosis is, why it happens, how the appearance hints at the culprit fungus, what an ENT clinic does versus what you can safely do at home, and how to keep it from returning.
What Is Otomycosis?
Otomycosis is a superficial fungal infection of the external auditory canal, the roughly 2.5 cm tunnel between your outer ear and eardrum. It is common: reported prevalence ranges from about 9% to 30% depending on the region and climate [Bojanović, Etiology, Predisposing Factors, Clinical Features and Diagnostic Procedure of Otomycosis: A Literature Review, 2023].
What makes it sneaky is that it rarely behaves like a typical ear infection. Instead of throbbing pain, the dominant complaints are intense itching and a feeling of fullness, often with a watery or debris-like discharge. In a series of 108 patients in Shanghai, pruritus and otorrhea were the most common presenting symptoms [Jia, Otomycosis in Shanghai: aetiology, clinical features and therapy, 2011].
In otherwise healthy people, otomycosis is annoying rather than dangerous. The frustration lies in how stubborn it can be, since it often requires repeated cleaning, weeks of treatment, and follow-up.
Why It Happens
The ear canal is normally protected by earwax, which is mildly acidic and water-repellent, and by an intact skin barrier. Otomycosis tends to take hold when that environment is disturbed. The strongest setup is warmth plus moisture, which is why infections cluster in tropical and humid climates and after swimming or frequent water exposure [Bojanović, Etiology, Predisposing Factors, Clinical Features and Diagnostic Procedure of Otomycosis: A Literature Review, 2023].
Self-cleaning is a major and often overlooked trigger. Cotton buds, hairpins, and fingernails create tiny abrasions that give fungi an entry point, and they push debris deeper. Frequent scratching or cleaning of the ear canal was the single most common predisposing factor (about 80% of cases) in the Shanghai series [Jia, Otomycosis in Shanghai: aetiology, clinical features and therapy, 2011].
Two other contributors deserve attention. Prolonged use of antibiotic or steroid ear drops can wipe out competing bacteria and let fungi flourish, and conditions such as diabetes or a suppressed immune system raise both the risk and the difficulty of clearing it [Bojanović, Etiology, Predisposing Factors, Clinical Features and Diagnostic Procedure of Otomycosis: A Literature Review, 2023].
Reading the Color: Which Fungus Is It?
Most otomycosis is caused by Aspergillus species, with Candida a distant second. In the Shanghai cohort, Aspergillus niger accounted for roughly 55% of cases and Candida albicans for about 17% [Jia, Otomycosis in Shanghai: aetiology, clinical features and therapy, 2011]. The way each organism looks inside the canal gives a useful first impression.
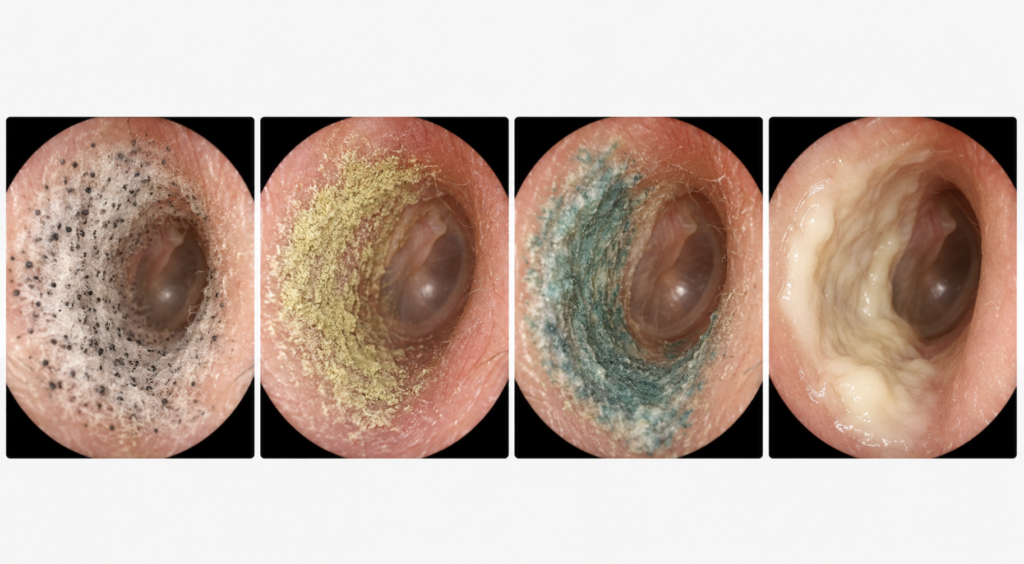
| What the ENT sees in the canal | Likely organism | Notes |
|---|---|---|
| Cottony white filaments dotted with grayish-black specks | Aspergillus niger group | The classic “salt-and-pepper” look; the black dots are spore heads |
| Yellow to yellow-green powdery growth | Aspergillus flavus | — |
| Blue-green to greenish growth | Aspergillus fumigatus | Rare in healthy ears; in weakened immunity it can invade deeper tissue, so warrants caution |
| No visible fungus, but a thick creamy-white discharge | Candida albicans | The discharge itself is the clue, not colored dots |
One important caveat: color is a starting point, not a diagnosis. The “black Aspergillus” that clinicians have long called A. niger is, under DNA testing, frequently a closely related cryptic species. When researchers sequenced 66 black Aspergillus isolates from ear canals, A. welwitschiae and A. tubingensis were actually more common than true A. niger [Gits-Muselli, Different repartition of the cryptic species of black aspergilli according to the anatomical sites in human infections, in a French University hospital, 2021]. For everyday treatment this rarely changes the plan, but it explains why definitive identification relies on microscopy and culture rather than the eye alone [Bojanović, Etiology, Predisposing Factors, Clinical Features and Diagnostic Procedure of Otomycosis: A Literature Review, 2023].
Treatment: The Clinic vs. Home
Effective treatment has two parts that work together: physically removing the fungus and then treating the cleaned surface with an antifungal. Skipping the first step is why home-only approaches so often fail.
In the ENT Clinic
The cornerstone is thorough cleaning of the canal under direct vision, usually with microsuction or careful debridement. Fungal debris forms a dense mat that shields the organisms and blocks medication from reaching the skin, so removing it matters as much as the drug. In the Shanghai series, mechanical debridement combined with a topical antifungal (fluconazole) cleared about 83% of cases on the first attempt [Jia, Otomycosis in Shanghai: aetiology, clinical features and therapy, 2011]. More broadly, topical azoles such as clotrimazole are the usual first-line choice in clinics worldwide and perform well.

After cleaning, the clinician applies or prescribes that antifungal. There are no formal international guidelines, but topical polyenes, imidazoles, and related agents are all used, with systemic triazoles reserved for severe disease [Bojanović, Etiology, Predisposing Factors, Clinical Features and Diagnostic Procedure of Otomycosis: A Literature Review, 2023]. Across different topical agents, resolution rates above 80% are typical [Ho, Otomycosis: clinical features and treatment implications, 2006]. For stubborn Aspergillus infections that fail local therapy, oral voriconazole has been used successfully [Ho, Treatment of refractory Aspergillus otomycosis with voriconazole: case series and review, 2014].
A safety check belongs here too: before any drops go in, the clinician confirms whether the eardrum is intact. Many common ear preparations contain ingredients that can be toxic to the inner ear or cause severe pain if they reach it through a perforated eardrum. This is exactly why ear drops left over from a past problem should never be poured in on a guess — only an examination can confirm the eardrum is whole.
At Home: Care, Not Cleaning
Home management is about supporting recovery, not digging the fungus out yourself. The most useful things you can do are keep the ear dry, finish the full course of prescribed drops exactly as directed, and stop any unnecessary antibiotic drops that may have started the problem.
What not to do is just as important. Avoid cotton buds, ear candles, and improvised tools, since self-cleaning is one of the leading triggers in the first place and risks pushing debris deeper or injuring the eardrum [Jia, Otomycosis in Shanghai: aetiology, clinical features and therapy, 2011]. If symptoms are worsening, painful, or not improving after treatment, that is a reason to be seen rather than to clean harder.
How to Stop It Coming Back
Recurrence is the defining frustration of otomycosis. Even with appropriate treatment, recurrence occurred in roughly 15% of patients in one academic series, and was higher in those with a mastoid cavity from previous surgery [Ho, Otomycosis: clinical features and treatment implications, 2006].
Prevention works by removing the conditions the fungus needs. Keep the canal dry after swimming or showering, break the habit of cleaning your ears with anything, and manage underlying contributors such as poorly controlled diabetes, which makes eradication harder [Jia, Otomycosis in Shanghai: aetiology, clinical features and therapy, 2011]. Hearing aids and earplugs should be kept clean and dry, and antibiotic ear drops should not be used longer than necessary.
Clinical Perspective
A common and costly mistake is treating relentless ear itch with repeated courses of antibiotic ear drops. That often backfires, wiping out the helpful bacteria that normally keep fungi in check and leaving an open, unguarded niche where fungi can multiply rapidly. The second point worth emphasizing is that, in otomycosis, the cleaning frequently matters more than the prescription. A meticulous debridement under the microscope can do more than another bottle of drops, which is exactly why this is a condition to bring to a clinic rather than fight with a cotton bud at home.
Key Takeaways
- Otomycosis is a fungal ear-canal infection that itches and feels blocked far more than it hurts.
- A cottony white mat with black dots points to Aspergillus, while a thick creamy-white discharge points to Candida.
- The first treatment is not a drug but cleaning the canal; antifungal drops work best on a debrided ear.
- Self-cleaning with cotton buds is a leading cause and a leading reason it comes back.
- Recurrence is common, so keeping the ear dry and avoiding antibiotic-drop overuse is central to prevention.
FAQ
What do the black dots in my ear mean?
They are most often the spore heads of Aspergillus, the commonest cause of fungal ear infection. On examination they look like fine black specks scattered over a fuzzy white mat. Color is only a clue, though; confirming the exact organism needs microscopy or culture.
Is otomycosis contagious?
No. The fungi that cause it are environmental organisms already present around us, and the infection is not passed from person to person. It develops when local conditions in your ear, such as moisture or a broken skin barrier, let the fungus take hold.
Can otomycosis clear up on its own?
It usually does not resolve fully without treatment, because fungal debris shields the organisms in the canal. The reliable path is professional cleaning followed by an antifungal, and recurrence is common if the underlying triggers are not addressed.
References
Bojanović M, Stalević M, Arsić-Arsenijević V, et al. Etiology, predisposing factors, clinical features and diagnostic procedure of otomycosis: a literature review. J Fungi (Basel). 2023;9(6):662.
Gits-Muselli M, Hamane S, Verillaud B, et al. Different repartition of the cryptic species of black aspergilli according to the anatomical sites in human infections, in a French University hospital. Med Mycol. 2021;59(10):985-992.
Ho HC, Hsiao SH, Lee CY, Tsai CC. Treatment of refractory Aspergillus otomycosis with voriconazole: case series and review. J Laryngol Otol. 2014;128(6):547-551.
Ho T, Vrabec JT, Yoo D, Coker NJ. Otomycosis: clinical features and treatment implications. Otolaryngol Head Neck Surg. 2006;135(5):787-791.
Jia X, Liang Q, Chi F, Cao W. Otomycosis in Shanghai: aetiology, clinical features and therapy. Mycoses. 2011;55(5):404-409.
Joonpyo Hong, MD is a board-certified otolaryngologist practicing in Korea. This article reflects his clinical interpretation of published research and does not constitute individual medical advice.
For more interesting contents:
https://curiousmd.com/random-stabbing-ear-pain-few-seconds/
https://curiousmd.com/cotton-swabs-in-your-ears/