
A hoarse voice can be described in words — rough, breathy, strained — or it can be measured in numbers. MDVP voice analysis does the second, using the Multi-Dimensional Voice Program (MDVP) to turn a few seconds of sound into dozens of acoustic values. This guide explains what those values mean, how to read the result sheet, and where the numbers stop being reliable.
What Is MDVP and How Does It Work?
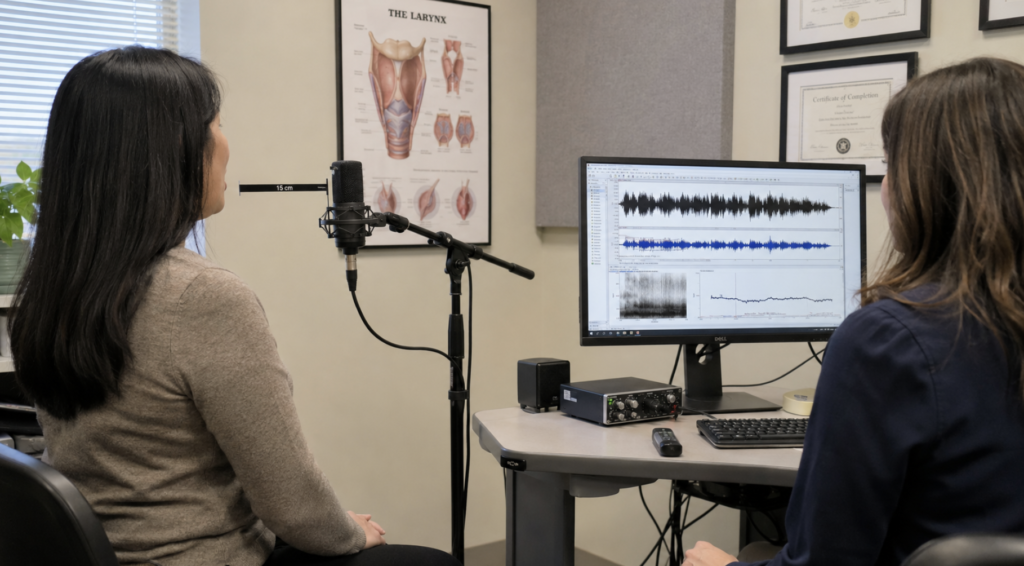
MDVP is a software program, first released by Kay Elemetrics in 1993 and later carried forward under KayPENTAX, that calculates up to 33 acoustic parameters from a single voice sample [Nicastri, MDVP amplitude variation parameters in euphonic adults, 2004]. It runs on a Computerized Speech Lab unit paired with a calibrated microphone. The underlying idea is simple: sound is a wave, and a disordered voice produces an irregular one.
The recording itself is quick. The patient sustains a steady vowel — usually /a/ — for about three seconds in a quiet room, with the microphone held at a fixed distance, and the software analyzes the central, most stable portion of that sample [Nicastri, MDVP amplitude variation parameters in euphonic adults, 2004]. Standardizing the setup matters, because the same voice can produce different numbers if intensity, pitch, or background noise drift during the recording.
From that short sample, MDVP sorts its measurements into a few families: fundamental frequency (F0, the baseline pitch), frequency perturbation (jitter), amplitude perturbation (shimmer), and noise measures such as the noise-to-harmonics ratio (NHR). Each family captures a different way a voice can stray from a clean, periodic signal.
What Is MDVP Used For?
The main appeal of MDVP is objectivity. Perceptual judgment — deciding by ear that a voice is “moderately rough” — varies between listeners, and even for the same listener on different days. A number does not. That reproducibility is why acoustic measures like jitter and shimmer were built into the European Laryngological Society’s basic protocol for assessing voice pathology, as one of five recommended approaches alongside perception, videostroboscopy, aerodynamics, and patient self-rating [Dejonckere, A basic protocol for functional assessment of voice pathology, 2001].
In practice, the test earns its place in three situations. It documents a baseline before treatment, whether that treatment is phonosurgery or voice therapy. It measures change afterward, giving an objective before-and-after comparison. And it supports monitoring and research, where consistent numbers let results be pooled across centers.
A clear illustration comes from a randomized trial of patients intubated for surgery. When intubation caused vocal fold swelling, the pre- to post-operative changes in jitter and shimmer moved together almost in lockstep (correlation of 0.95), tracking the induced edema — evidence that these numbers reflect real tissue change, not just measurement noise [Sørensen, Normative values of MDVP parameters before and after intubation, 2015].
How to Read the MDVP Result Sheet
MDVP’s signature output is a circular diagram. Each acoustic parameter is drawn as a spoke radiating from the center, and a green ring marks the upper limit of the normal range. Spokes that stay inside the ring are within normal limits; spokes that push past it flag parameters that are abnormal for that voice. The further a spoke extends beyond the green, the larger the deviation.
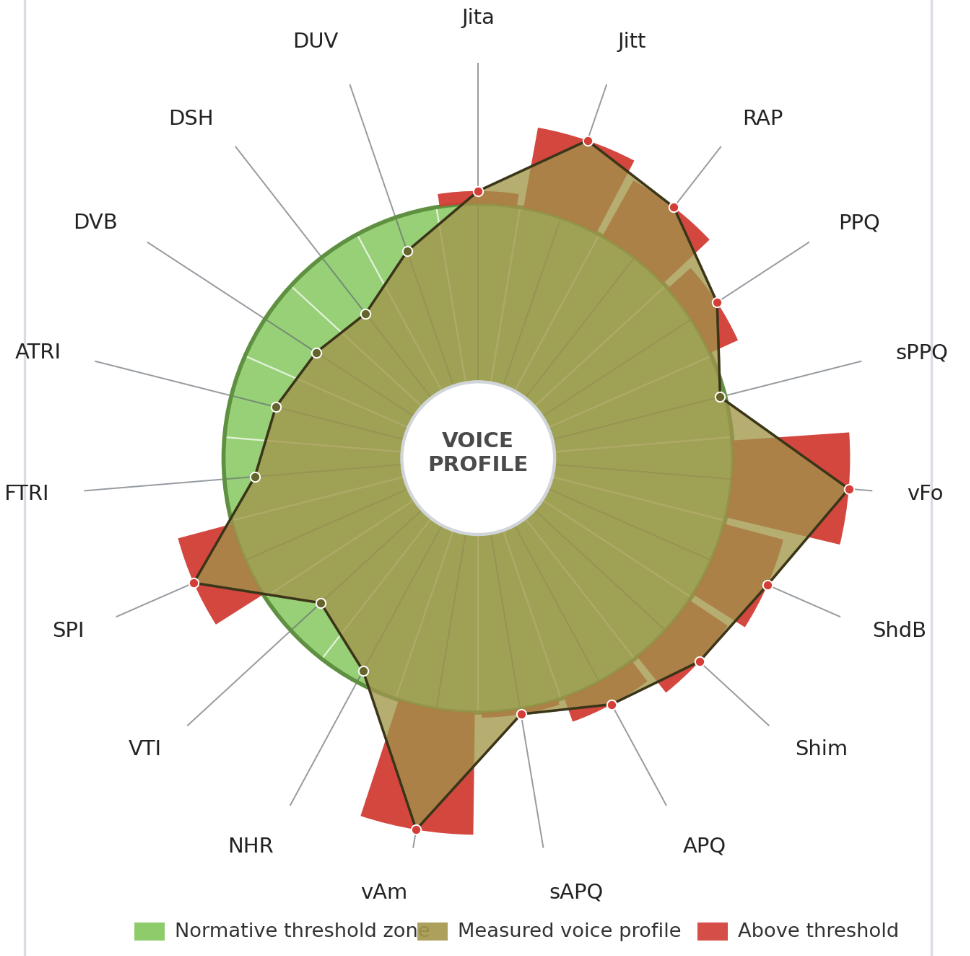
To read it well, you need to know what the main spokes represent.
| Parameter | What it measures | What elevation suggests |
|---|---|---|
| F0 | Fundamental frequency (baseline pitch) | Pitch shifted from age/sex norms |
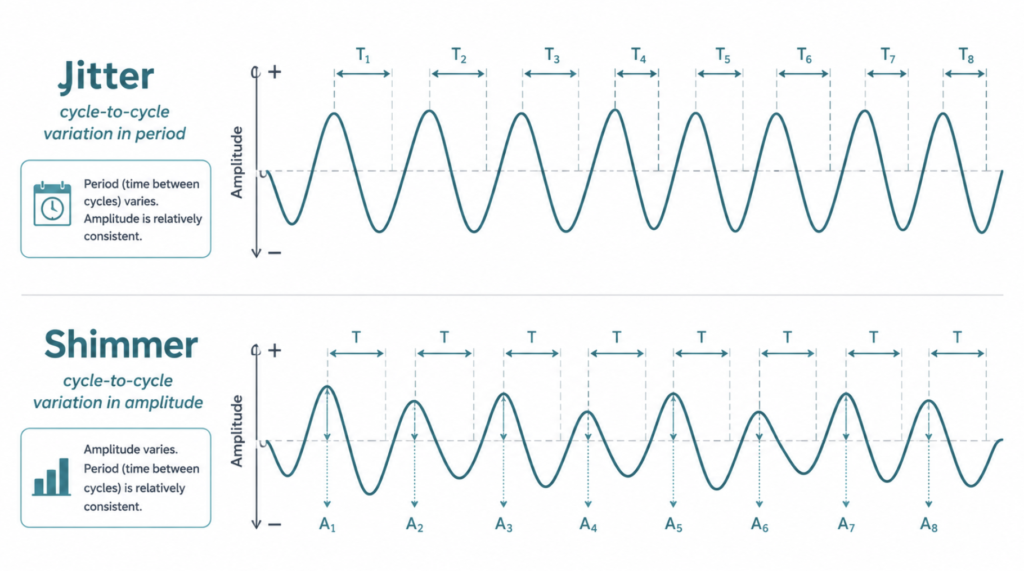
| Jitter (Jitt %) | Cycle-to-cycle frequency variation | Roughness; unstable vocal fold vibration |
| Shimmer (Shim %, ShdB) | Cycle-to-cycle amplitude variation | Roughness and breathiness |
| NHR | Ratio of noise to harmonic energy | Breathiness, hoarseness, turbulence |
When jitter, shimmer, and NHR rise together, they can indicate a rough, irregular, and noisy dysphonic voice — but this is a nonspecific acoustic pattern, not a fingerprint for any one lesion, and identifying the cause requires laryngoscopy alongside other assessments. Individual measures can also dissociate: a breathy voice may show elevated noise while jitter stays normal, and raised NHR can reflect incomplete glottic closure rather than aperiodic vibration. The diagram is a starting map that tells you which features are off, and by how much, so you know where to look next.
Why MDVP Voice Analysis Matters
The honest answer is that the ear is powerful but not reproducible. Two skilled clinicians can disagree on whether a voice is mild or moderate dysphonia, and neither can easily prove improvement to a patient — or an insurer — with a number. Acoustic analysis fills that gap by producing measurements that can be repeated and charted [Kent, Voice dysfunction in dysarthria, 2003].
It also catches change that is too small or too gradual to hear. A patient three weeks into voice therapy might sound “about the same” to everyone in the room while their jitter and NHR have measurably dropped. Numbers turn a vague impression into a trend line, which is exactly what you need to judge whether a treatment is working or a lesion is progressing.
Clinical Perspective
MDVP is a measuring tape, not a diagnosis. Its perturbation measures assume the voice is periodic enough to track cycle by cycle, and that assumption breaks down in severely disordered voices — once vibration becomes near-chaotic, jitter and shimmer grow unreliable and can mislead.
The numbers also shift with recording conditions and how steadily the patient phonates, so a single poor take should never be read as a result on its own. This is part of why the field has moved toward cepstral and multiparametric measures — indices such as the Acoustic Voice Quality Index (AVQI) and smoothed cepstral peak prominence — which hold up better in severe dysphonia and in connected speech, and which carry meaningful information about overall severity [Gölaç, multiparametric index scores and cepstral-based methods, 2025]. Read MDVP alongside the laryngoscopy and the patient’s own report, never in isolation.
Key Takeaways
- MDVP calculates up to 33 acoustic parameters from a few seconds of a sustained vowel.
- Jitter measures frequency variation, shimmer measures amplitude variation, and NHR measures the ratio of noise to harmonic energy in the voice.
- On the MDVP result chart, any parameter whose spoke extends past the green ring is outside the normal range.
- Acoustic analysis is valued because its numbers are reproducible, unlike judging a voice by ear.
- In severely disordered voices, jitter and shimmer become unreliable, and cepstral measures such as AVQI are often more robust.
FAQ
What is a normal jitter value in MDVP? Jitter percent below roughly 1% is generally treated as within normal limits in MDVP, though the exact threshold depends on the normative database and recording setup. The software compares each value against built-in reference thresholds and flags anything above them on the diagram. Because normative values differ noticeably between studies and populations [Nicastri, MDVP amplitude variation parameters in euphonic adults, 2004], a result just over the line should be read in context rather than as a hard cutoff.
Is MDVP the same as Praat? No — both analyze voice acoustically, but they are different tools. MDVP is a commercial package that outputs up to 33 parameters plus a normative diagram, while Praat is free, open-source software widely used in research. Their jitter and shimmer values are computed with different algorithms and are not always interchangeable, so comparing results across the two requires caution.
Does MDVP diagnose vocal cord disease? No, MDVP does not make a diagnosis. It quantifies how a voice deviates from a clean signal, which helps localize and grade a problem, but the diagnosis comes from laryngoscopy or stroboscopy and clinical evaluation. It is best understood as evidence that supports a diagnosis, not the diagnosis itself.
How long does the test take? The recording takes only seconds — typically a sustained vowel held for about three seconds, sometimes repeated to capture the best of three attempts. The full appointment runs longer because it includes setup, instructions, and often other assessments such as laryngoscopy, but the acoustic capture itself is brief and non-invasive.
References
Kent RD, Vorperian HK, Kent JF, Duffy JR. Voice dysfunction in dysarthria: application of the Multi-Dimensional Voice Program. J Commun Disord. 2003;36(4):281-306.
Nicastri M, Chiarella G, Gallo LV, Catalano M, Cassandro E. Multidimensional Voice Program (MDVP) and amplitude variation parameters in euphonic adult subjects. Normative study. Acta Otorhinolaryngol Ital. 2004;24(6):337-341.
Dejonckere PH, Bradley P, Clemente P, Cornut G, Crevier-Buchman L, Friedrich G, Van De Heyning P, Remacle M, Woisard V. A basic protocol for functional assessment of voice pathology, especially for investigating the efficacy of (phonosurgical) treatments and evaluating new assessment techniques. Eur Arch Otorhinolaryngol. 2001;258(2):77-82.
Sørensen MK, Durck TT, Bork KH, Rasmussen N. Normative values and interrelationship of MDVP voice analysis parameters before and after endotracheal intubation. J Voice. 2015;30(5):626-630.
Gölaç H, Gülaçtı A, Atalık G, Çabuk GB, Yılmaz M. What do the voice-related parameters tell us? The multiparametric index scores, cepstral-based methods, patient-reported outcomes, and durational measurements. Eur Arch Otorhinolaryngol. 2025;282(3):1355-1365.
Joonpyo Hong, MD is a board-certified otolaryngologist practicing in Korea. This article reflects his clinical interpretation of published research and does not constitute individual medical advice.
For more intersting contents:
https://curiousmd.com/neuralink-voice-speech-first/
https://curiousmd.com/how-ai-voice-cloning-works/
https://curiousmd.com/ai-laryngeal-cancer-detection/
Link out to:
- ASHA Practice Portal: Voice Disorders — a professional-body overview of comprehensive voice assessment, including clinical and instrumental evaluation.
- Praat Manual — Voice 2. Jitter — technical definitions of the jitter variants and the pathology thresholds MDVP uses.
- PhonaLab — Jitter and Shimmer: What They Really Tell You — when perturbation measures are valid, where they fail, and the move toward cepstral measures.