
When bone conduction headphones first reached consumers in 2011 with AfterShokz (now Shokz), audiology commentary pushed back hard on early marketing claims. The main issue was “Bone Conduction Headphones and Hearing Loss”. The argument from manufacturers was that bone conduction headphones are convenient and safe. The audiology counter-argument was that the eardrum is not where noise-induced hearing damage originates — the cochlea is — and that pushing vibrations directly through the skull toward the cochlea might accelerate damage rather than prevent it.
Fifteen years on, with the category now mainstream and tens of millions of units in circulation, the predicted wave of bone-conduction-specific hearing loss has not appeared in the literature. The picture is more nuanced than the original prediction suggested — and also more nuanced than current marketing suggests.
The 2011 Concern Was Reasonable on Its Face
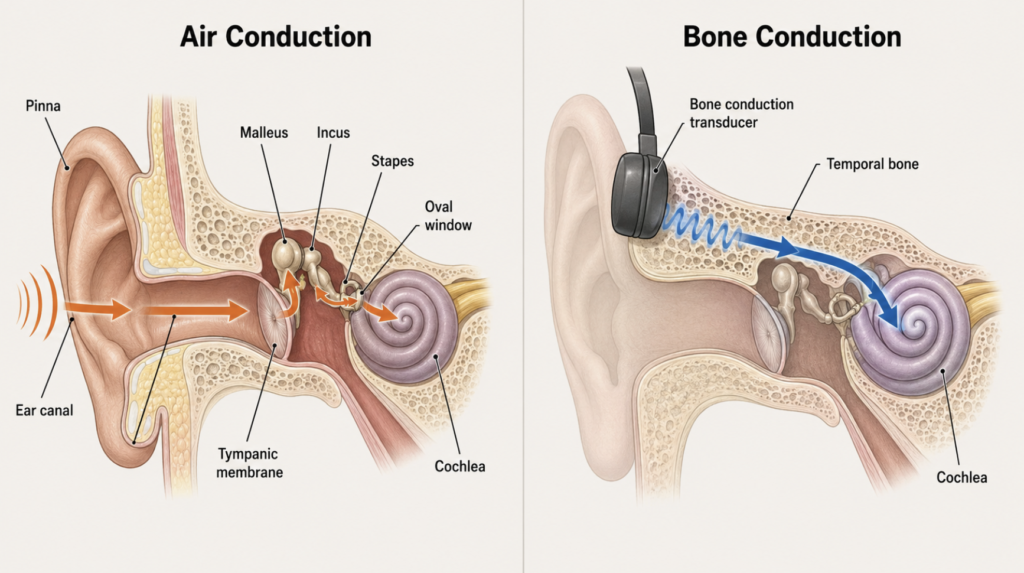
The mechanical worry made anatomical sense. Air-conducted sound travels through the external ear, vibrates the tympanic membrane, is transmitted through the ossicular chain, and only then reaches the cochlea. Each of those stages dissipates a portion of the input energy. Bone conduction, in contrast, sets the temporal bone itself into motion, and the cochlear capsule — embedded in that bone — is stimulated through several parallel mechanisms: ossicular inertia, inner ear fluid inertia, compression and expansion of the cochlear walls, and pressure transmission from the cranial cavity [Stenfelt, Bone-conducted sound: physiological and clinical aspects, 2005].
A reasonable hypothesis from those mechanics: bypass the eardrum and you might deliver more energy, more directly, to the same vulnerable structure — the outer hair cells of the organ of Corti. Combine that with the behavioral pattern long documented in personal-audio research (listeners turn the volume up to mask ambient noise), and the audiology community in 2011 had legitimate grounds for concern.
What Has Protected Users So Far
Two hardware-side factors appear to explain why the 2011 worry did not turn into a 2026 epidemic.
1. The pathway is genuinely less efficient
Subsequent measurement work has clarified that bone conduction is a less efficient route to the cochlea, not a more efficient one. The clinical evidence for this is built into audiometry itself: international standards (ISO 389-3) specify a substantially higher reference equivalent threshold force level for bone vibrators than the corresponding reference sound pressure level for air conduction. In plain terms, producing the same hearing threshold via bone conduction requires considerably more transducer output force than producing it via air conduction at the eardrum. Significant vibrational energy is absorbed and dispersed by the skull and surrounding soft tissue before vibration reaches the cochlear capsule [Stenfelt, Inner ear contribution to bone conduction hearing in the human, 2015].
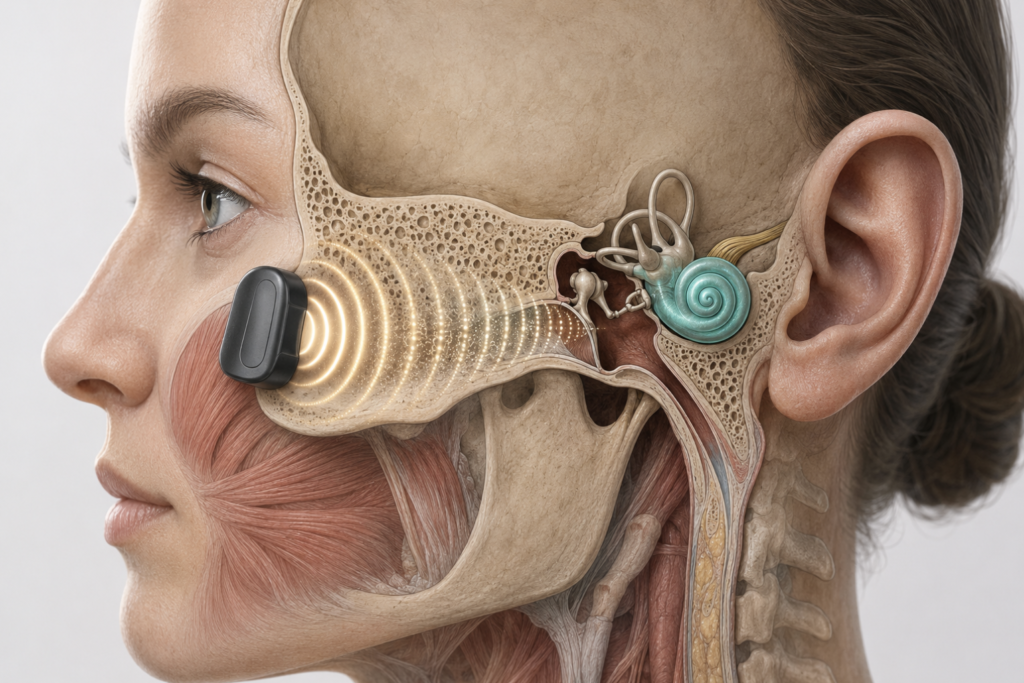
The most directly relevant study on consumer-style headsets characterized bone conduction transmission with transducers at the frontal position used by commercial headphones (rather than the clinical mastoid position) and found that the same physiological pathways are engaged — including a substantial ear-canal-radiated sound pressure component reaching 85 to 105 dB SPL depending on frequency — rather than some new high-efficiency cochlear shortcut [Surendran, Hearing Through Bone Conduction Headsets, 2023].
The original “direct stimulation” framing turned out to be a misleading shorthand. Bone conduction reaches the cochlea, but not more aggressively than air conduction does.
2. Consumer hardware imposes a physical ceiling
Commercial bone conduction headphones operate at modest output levels because pushing them harder is mechanically self-limiting. Higher output from a skull-coupled transducer produces vibration intense enough that the user feels uncomfortable buzzing on the cheekbone or temple long before the cochlea is in danger. Sealed in-ear monitors face no such constraint and can produce sound pressure exceeding 100 dB at the tympanic membrane.
In effect, the form factor itself imposes a noise-exposure ceiling that in-ear earbuds do not.
The Risk Bone Conduction Quietly Adds
There is one factor in the opposite direction that early marketing glossed over and that audiologists have been more vocal about in recent years.
Sealed in-ear monitors passively attenuate ambient noise. A user in a subway or on a busy street hears music and less of the surrounding noise, which means a moderate volume is often loud enough to enjoy the audio. Bone conduction headsets cannot attenuate ambient noise at all — the ear canal stays fully open. To overcome the masking effect of an 80 dB subway or a 75 dB roadway and actually hear the music, users tend to unconsciously crank the volume to its maximum.
This is the inverse of the protective behavioral argument that marketing has sometimes implied. In quiet environments, bone conduction users genuinely receive less cochlear stimulation at any given perceived loudness. In noisy environments, the same physics that prevents passive isolation also pushes users toward the upper limit of what the hardware can deliver — and the upper limit, as the Surendran data show, is not negligible. Heavy use of bone conduction headphones during loud commuting is not an obviously safer choice than heavy use of sealed earbuds at moderate volume.
Clinical Perspective:
Bone conduction Headphones and Hearing Loss
The 2011 prediction was a reasonable hypothesis from first principles, and the harm it forecast has not appeared. That is partly because the conduction physics is more forgiving than the original worry assumed, and partly because the hardware itself caps output below the level where cochlear damage typically accumulates. Neither of those reasons, though, is what the marketing usually claims. Bone conduction does not protect hearing because it bypasses the eardrum. It happens to be relatively gentle because it is mechanically inefficient and physically self-limiting.
The honest message for someone considering the switch: bone conduction offers real practical advantages — situational awareness during running or cycling, comfort for users with chronic ear canal inflammation, compatibility with behind-the-ear hearing aids — but treats the same cochlea by the same rules. The user who plays bone conduction headphones at full volume on a noisy subway every day is not in a meaningfully safer position than the user with sealed earbuds at moderate volume on the same subway.
What We Still Do Not Know
Fifteen years sounds like a long observation window. Biologically, it is not.
Sensorineural hearing loss from sub-clinical noise exposure can accumulate over decades, and the cohort of consumers who began using bone conduction headphones in 2011 is only now reaching the age range where presbycusis becomes routinely measurable. Untangling a small bone-conduction-specific contribution from background age-related decline will require longer follow-up than currently exists.
There is also no large prospective cohort study tracking bone conduction users against matched in-ear users. The current evidence base is composed of mechanistic studies (which show no reason to expect worse outcomes), clinical reports of bone conduction therapy in hearing-impaired populations [Hampton, Improved Speech Recognition in Adults With Conductive or Mixed Hearing Loss Using a Direct-to-Consumer Bone-Conduction Device, 2025], and the absence of an emerging clinical signal in audiology practice. Absence of evidence is not, as the phrase goes, evidence of absence — although in this case it is consistent with the mechanistic prediction.
The chronic complaints that have surfaced in user surveys are mechanical rather than auditory: pressure soreness at the temple, occasional tension headaches, and temporomandibular joint fatigue from sustained contact pressure. These are not trivial, but they are not hearing loss.
Key Takeaways
- Bone conduction headphones entered the consumer market in 2011, and a decade and a half of widespread use has not produced a distinct, bone-conduction-specific pattern of hearing loss in the audiology literature.
- The original 2011 concern — that bypassing the eardrum would expose the cochlea to more aggressive stimulation — was anatomically reasonable but has not been borne out; bone conduction is a less efficient pathway to the cochlea, as reflected in international audiometric calibration standards (ISO 389-3).
- Consumer bone conduction devices are mechanically self-limiting at modest output levels and cannot match the sound pressure that sealed in-ear monitors deliver at the tympanic membrane.
- The open-ear form factor offers situational awareness but provides no passive ambient noise attenuation, which can push users toward maximum volume in noisy environments — a real countervailing risk that early marketing glossed over.
- Fifteen years is not yet long enough to rule out a small contribution to age-stratified hearing decline, and no large prospective cohort comparing bone conduction users to in-ear users has been published.
FAQ
Do bone conduction headphones cause hearing loss? At typical listening volumes in quiet environments, there is no evidence they cause more hearing loss than in-ear earbuds. At high volumes — particularly the maximum volumes users tend to reach in noisy environments because the open ear cannot block ambient sound — the cochlear hair cells are damaged the same way regardless of the conduction pathway. The widely cited 60/60 heuristic — no more than 60 percent volume for no more than 60 minutes at a time — applies to bone conduction as it does to any personal audio device.
Are bone conduction headphones safer than in-ear earbuds? Not categorically. In quiet environments, bone conduction delivers slightly less cochlear stimulation at the same perceived loudness because the pathway is less efficient. In noisy environments, the open-ear design actually pushes users to crank the volume higher to overcome ambient masking, which can offset that advantage. The cochlea is treated by the same rules either way.
Why did audiologists initially warn against bone conduction? The concern was that direct skull stimulation would deliver vibration to the cochlea more efficiently than air conduction, bypassing the natural energy losses in the middle ear. Measurement work has since shown that bone conduction is actually a less efficient pathway, and the skull dissipates significant energy before vibration reaches the inner ear.
Can I use bone conduction headphones with a hearing aid? Yes. This is one of the genuine practical advantages of the form factor — the ear canal stays free, so a behind-the-ear hearing aid is not displaced or occluded.
What are the documented long-term side effects? The complaints that appear consistently in user surveys are mechanical: pressure soreness at the temple, mild tension-type headache, and temporomandibular joint fatigue from sustained contact pressure. Sensorineural hearing changes attributable specifically to bone conduction use have not been reported.
References
- Stenfelt S, Goode RL. Bone-conducted sound: physiological and clinical aspects. Otol Neurotol. 2005;26(6):1245-61.
- Stenfelt S. Acoustic and physiologic aspects of bone conduction hearing. Adv Otorhinolaryngol. 2011;71:10-21.
- Stenfelt S. Inner ear contribution to bone conduction hearing in the human. Hear Res. 2015;329:41-51.
- Surendran S, Prodanovic S, Stenfelt S. Hearing Through Bone Conduction Headsets. Trends Hear. 2023;27:23312165231168741.
- Hampton T, Fletcher M, Sanderson A, Loureiro M, Mortimer K, Bhutta MF. Improved Speech Recognition in Adults With Conductive or Mixed Hearing Loss Using a Direct-to-Consumer Bone-Conduction Device: A Multiple Methods Intervention Study. JMIR Rehabil Assist Technol. 2025;12:e66013.
Joonpyo Hong, MD is a board-certified otolaryngologist practicing in Korea. This article reflects his clinical interpretation of published research and does not constitute individual medical advice.
For more interesting contents:
https://curiousmd.com/ai-hearing-aids-2026-ent-review/
https://curiousmd.com/brain-controlled-hearing-aid-2026/
https://curiousmd.com/psap-vs-hearing-aid-clinical-evidence/
https://curiousmd.com/objective-hearing-tests-abr-assr-oae/
Link out to:
https://doi.org/10.1177/23312165231168741
https://www.iso.org/standard/59759.html
https://www.nidcd.nih.gov/health/noise-induced-hearing-loss