Consider an illustrative scenario: a 32-year-old recreational lifter pulls a 425-pound deadlift PR. He racks the bar, takes two steps, and the left ear goes underwater — muffled, full, with a high-pitched ring. Six hours later he is vertiginous and vomiting. An ER workup rules out stroke. The diagnosis, three weeks and four specialists later, is a perilymphatic fistula. He did not herniate a disc. He blew out an inner ear window.
Perilymphatic fistula from weightlifting is more common than most lifters or clinicians recognize. This article unpacks why a routine maximal lift can rupture the membranes of the inner ear, who is at risk, and what the lifter and the clinician should do about it.
What a Perilymphatic Fistula Actually Is
A perilymphatic fistula (PLF) is an abnormal opening between the fluid-filled inner ear and the air-filled middle ear, allowing perilymph to leak out. Most fistulae occur at the oval window or round window — the two thin membranes that seal the cochlea and vestibule from middle-ear air [Sarna B, Perilymphatic Fistula: A Review of Classification, Etiology, Diagnosis, and Treatment, 2020]. When perilymph drops, the hydraulic balance that lets hair cells transduce sound collapses, and the vestibular end-organs misfire.
Symptoms are nonspecific and that is part of the problem: sudden or fluctuating sensorineural hearing loss, vertigo (especially triggered by pressure changes), aural fullness, tinnitus, and autophony — hearing one’s own voice or heartbeat unnaturally loudly in the affected ear [Saliba I, Suspicion and Treatment of Perilymphatic Fistula: A Prospective Clinical Study, 2024]. The same symptoms appear in Ménière disease, vestibular migraine, and superior canal dehiscence, which is why the diagnosis is delayed in most cases.
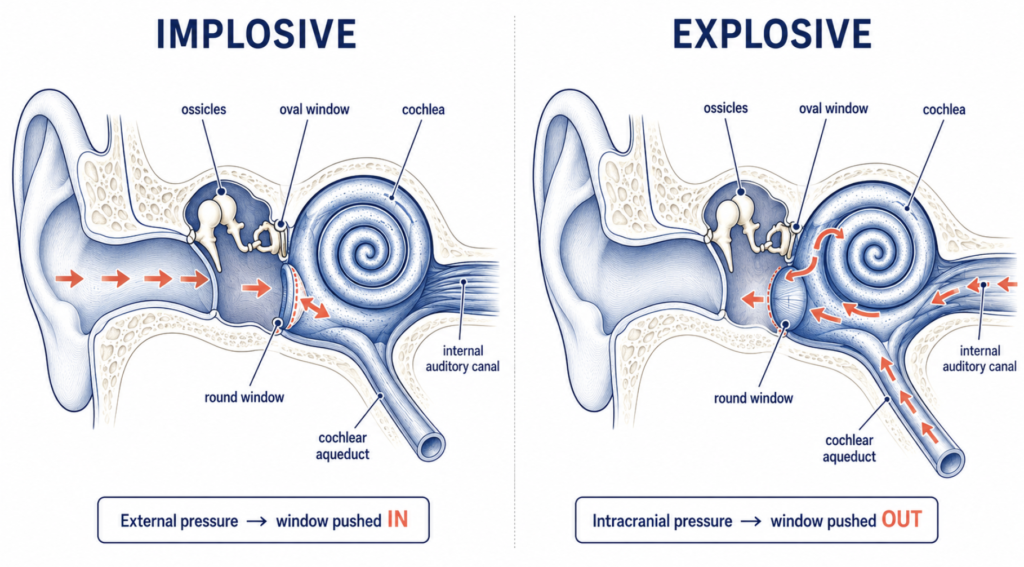
Goodhill’s Two Routes: Implosive vs Explosive
In 1971, Victor Goodhill described two hydrodynamic mechanisms that can rupture the inner-ear windows [Goodhill V, Sudden Deafness and Round Window Rupture, 1971]. The distinction still anchors how otologists think about PLF.
The implosive route transmits pressure from outside the inner ear. A rapid spike in middle-ear pressure — airplane descent without equalization, scuba descent, a pinched-nose sneeze, an open-handed slap to the ear — drives the ossicles inward against the oval window, or pushes the round window membrane inward from middle-ear air. The membrane fails from the outside in.
The explosive route goes the other way. A surge in intracranial pressure (ICP) transmits to the perilymph through the cochlear aqueduct or through the lamina cribrosa of the internal auditory canal. The pressure builds inside the labyrinth and blows the window out from within. Heavy lifting, straining at stool, prolonged coughing, childbirth pushing, and forceful nose blowing all fall in this category [Sarna B, Perilymphatic Fistula: A Review of Classification, Etiology, Diagnosis, and Treatment, 2020].
Weight training sits squarely in the explosive category — and the data on how much pressure a heavy lift produces is striking.
The Lifting Cascade: From Barbell to Cochlea
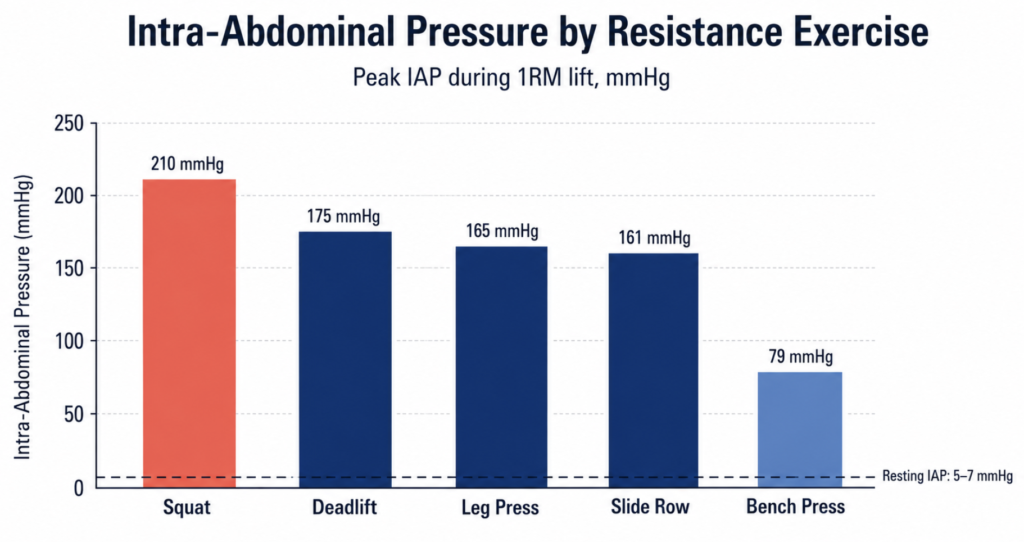
When a lifter holds breath against a closed glottis under maximal load, intra-abdominal pressure (IAP) rises sharply. A 2019 systematic review measured the actual numbers: IAP above 200 mmHg during heavy squats, 161–176 mmHg during the deadlift, leg press, and slide row, and lower values during the bench press [Blazek D, Systematic Review of Intra-Abdominal and Intrathoracic Pressures Initiated by the Valsalva Manoeuvre During High-Intensity Resistance Exercises, 2019]. For reference, normal IAP at rest sits around 5–7 mmHg.

That pressure does not stay in the abdomen. Direct intracranial recordings during resistance exercise with a Valsalva maneuver show that ICP rises sharply alongside systolic blood pressure during the lift [Haykowsky MJ, Resistance Exercise, the Valsalva Maneuver, and Cerebrovascular Transmural Pressure, 2003]. The pathway: intrathoracic pressure compresses the great veins, blood backs up through the vertebral venous plexus, cerebrospinal fluid pressure rises, and the wave is transmitted to the perilymph via the cochlear aqueduct and the porous lamina cribrosa of the internal auditory canal [Sarna B, Perilymphatic Fistula: A Review of Classification, Etiology, Diagnosis, and Treatment, 2020].
In a window membrane with normal compliance, the pressure dissipates harmlessly. In a window with a pre-existing weakness — an idiopathic thinning, an old undiagnosed micro-tear, a congenital fissula ante fenestram — the membrane gives way.
Clinical Perspective: Two points are easy to miss in the lifting context. First, the symptom does not always announce itself at the moment the bar racks; a micro-leak can declare itself hours later as endolymphatic hydrops develops secondarily. Second, the implicated lift is rarely a sloppy attempt — it is usually a clean, hard-braced 1RM where the Valsalva was sustained the longest.
Daily-Life Triggers: A Spectrum, Not a Light Switch
Heavy lifting is the loudest example, but the explosive mechanism quietly causes PLF in much more ordinary activities. The literature documents fistulae after a single forceful sneeze, after a hard nose blow, after straining to pass a stool, during the second stage of labor, and during a coughing fit in a patient with bronchitis [Comacchio F, Sneezing and Perilymphatic Fistula of the Round Window: Case Report and Systematic Review of the Literature, 2018; Klokker M, Perilymphatic Fistula in Cabin Attendants: An Incapacitating Consequence of Flying With Common Cold, 2005].
How Often Is PLF Truly Spontaneous?
The largest dataset on this question comes from a nationwide Japanese multicenter study using the cochlin-tomoprotein (CTP) biomarker to confirm perilymph leakage [Matsuda H, A Nationwide Multicenter Study of the Cochlin Tomo-Protein Detection Test: Clinical Characteristics of Perilymphatic Fistula Cases, 2017]. The investigators classified confirmed PLF cases into four etiologic categories. The breakdown was striking.
Category 1 (trauma, middle/inner ear disease, otologic surgery), Category 2 (external barotrauma — flying, diving), and Category 3 (internal barotrauma — lifting, sneezing, coughing, straining) together accounted for roughly 61% of cases. The remaining 38.6% fell into Category 4: no identifiable antecedent event — true spontaneous or idiopathic PLF [Sarna B, Perilymphatic Fistula: A Review of Classification, Etiology, Diagnosis, and Treatment, 2020]. Read the other way: in nearly four out of ten patients with biomarker-confirmed perilymph leakage, there was no preceding lift, sneeze, dive, flight, or trauma to point to.
This is more than an academic taxonomy. Recent CTP-based studies estimate that approximately 20% of cases of idiopathic sudden sensorineural hearing loss (ISSNHL) may in fact harbor an unrecognized perilymphatic fistula [Sasaki A, Prevalence of Perilymphatic Fistula in Patients With Sudden-Onset Sensorineural Hearing Loss as Diagnosed by Cochlin-Tomoprotein (CTP) Biomarker Detection, 2024]. A meaningful fraction of patients diagnosed with idiopathic sudden deafness — and treated only with steroids — may actually have a structural lesion that could benefit from window sealing.
The likely explanations for spontaneous cases include congenital weakness of the otic capsule, microfissures around the round window niche, a thinned oval window annulus, or an old sub-threshold injury that finally decompensated. The mechanism is still explosive or implosive at the cellular level — it just happened too quietly for the patient to register.
The practical implication for lifters: a fistula that opens during a deadlift is the same lesion that may have started after a flu-induced coughing fit two years earlier, or with no remembered event at all. Mechanism does not care about the venue, and absence of an obvious trigger does not rule out the diagnosis.
Red Flags: When a Clinician Should Suspect PLF
After heavy training, a brief sensation of ear pressure or muffled hearing that resolves within minutes is usually benign barotrauma. The findings that warrant ENT evaluation, ideally within 48–72 hours, are different. The following constellation should raise serious suspicion for PLF [Sarna B, Perilymphatic Fistula: A Review of Classification, Etiology, Diagnosis, and Treatment, 2020; Saliba I, Suspicion and Treatment of Perilymphatic Fistula: A Prospective Clinical Study, 2024]:
- Sudden unilateral sensorineural hearing loss following an exertional event — a lift, a sneeze, a dive, a flight, a strain. The temporal link is the single most informative piece of history.
- Pressure-induced or Valsalva-induced vertigo. Symptoms reliably reproduced by bending forward, coughing, straining, blowing the nose, or attempting another lift.
- Tullio phenomenon — vertigo or nystagmus triggered by loud sound in the affected ear.
- Hennebert sign — vertigo or nystagmus elicited by tragal pressure or pneumatic otoscopy on the affected side.
- Autophony — hearing one’s own voice, breathing, or heartbeat unnaturally loudly in the affected ear.
- Fluctuating hearing that worsens with altitude change, barometric shift, or physical exertion.
- Delayed onset of cochleovestibular symptoms hours to days after the inciting event, rather than at the moment of trauma.
- Low-frequency tinnitus or a pulsatile auditory sensation, often described as “underwater” or “muffled.”
- Failure of standard sudden-SNHL treatment (systemic and intratympanic steroids) to produce expected improvement at 1–2 weeks.
- Positional symptoms — vertigo or aural fullness reproducibly worse when lying on the affected ear, or relieved by lying on the contralateral side.
A patient who hits three or more of these on history alone deserves a CTP test where available, high-resolution temporal bone CT to exclude superior semicircular canal dehiscence and pneumolabyrinth, and a low threshold for exploratory tympanotomy if symptoms progress.
Differential diagnosis on the spot matters. Superior semicircular canal dehiscence produces similar Valsalva-induced vertigo and autophony but is a bony defect visible on CT, not a soft-tissue tear. Sudden sensorineural hearing loss without an obvious antecedent demands its own urgent workup with steroids — and, as the CTP data above suggest, may itself be an occult PLF.
Management: Conservative First, Surgical When Needed
First-line treatment is strict bed rest with head elevation, avoidance of all Valsalva (stool softeners are routinely prescribed), no lifting, no nose blowing, and no air travel. The standard initial window is one to two weeks of strict conservative care, followed by formal reassessment of hearing and vestibular symptoms. When sensorineural hearing loss or significant vertigo fails to improve at the two-week mark, exploratory tympanotomy with window sealing is generally considered, rather than further prolonged observation [Sarna B, Perilymphatic Fistula: A Review of Classification, Etiology, Diagnosis, and Treatment, 2020].
The procedure itself is either an intratympanic blood patch — autologous blood injected into the middle ear to encourage sealing of the windows — or exploratory tympanotomy with graft reinforcement of both oval and round windows using temporalis fascia, perichondrium, or fat [Saliba I, Suspicion and Treatment of Perilymphatic Fistula: A Prospective Clinical Study, 2024]. The latter remains the definitive treatment when conservative care fails or when symptoms recur.
Return to lifting is the conversation lifters most want and clinicians most dread. A reasonable post-surgical framework restricts lifting to light, everyday loads under approximately 5 kg for the first two to four weeks, with complete avoidance of any activity that raises intra-abdominal pressure for at least one month. Beyond that, return is graded rather than binary: submaximal training with strictly controlled breathing — exhaling on exertion, never grinding a repetition with a closed glottis — is reasonable for many patients. Maximal-effort 1RM attempts, however, are strongly discouraged because they reapply precisely the pressure that produced the original rupture. The final decision belongs to a shared-decision conversation between the patient and the otologist, weighing structural vulnerability, recurrence risk, and the lifter’s individual goals.
Key Takeaways
- Perilymphatic fistula from weightlifting follows the explosive route: heavy Valsalva raises intracranial pressure, which transmits through the cochlear aqueduct and ruptures the inner-ear windows from within.
- Squats produce the highest measured intra-abdominal pressures of any resistance exercise — over 200 mmHg under heavy load — followed by deadlift and leg press.
- In the largest biomarker-confirmed series, about 38.6% of PLF cases were spontaneous with no identifiable trigger, and roughly 20% of idiopathic sudden sensorineural hearing loss may in fact be unrecognized PLF.
- Red flags include sudden unilateral hearing loss after exertion, Valsalva-induced vertigo, Tullio and Hennebert signs, autophony, delayed onset of symptoms, and failure of standard sudden-SNHL treatment to improve.
- Conservative care (strict bed rest, no Valsalva, no lifting) is the initial approach for one to two weeks; persistent hearing loss or vertigo at the two-week mark warrants consideration of intratympanic blood patch or exploratory tympanotomy. Maximal-effort 1RM attempts after repair are strongly discouraged, with submaximal training under controlled breathing decided through shared decision-making.
FAQ
Can lifting weights really cause hearing loss? Yes, through a recognized mechanism: a maximal Valsalva maneuver raises intracranial pressure, which is transmitted to the inner ear and can rupture the round or oval window. The result is a perilymphatic fistula, which presents as sudden one-sided muffled hearing, fullness, tinnitus, and often vertigo. The connection is documented across decades of otology literature.
Why would symptoms appear after the workout, not during? A small tear can leak slowly. As perilymph volume drops, secondary endolymphatic hydrops develops, and the resulting fluid imbalance produces the muffled hearing and rotational vertigo that the patient finally notices in the car ride home or at dinner. Delayed onset is common and does not rule out the diagnosis.
Should I stop lifting forever after a perilymphatic fistula? Not necessarily. After full recovery, many patients return to submaximal lifting with strict breathing technique — exhaling on exertion rather than holding the breath against a closed glottis. Maximal-effort 1RM attempts, however, are strongly discouraged because they reapply the exact pressure that caused the original rupture. The decision is individualized through shared decision-making with the otologist, weighing structural vulnerability against the lifter’s goals.
How is this different from a Ménière attack? Ménière disease produces episodic vertigo and fluctuating low-frequency hearing loss with no consistent trigger and tends to recur over years. A perilymphatic fistula typically begins with a specific exertional event and worsens with pressure changes — coughing, straining, bending forward, the next gym session. The history, more than any single test, distinguishes the two.
References
Blazek D, Stastny P, Maszczyk A, Krawczyk M, Matykiewicz P, Petr M. Systematic review of intra-abdominal and intrathoracic pressures initiated by the Valsalva manoeuvre during high-intensity resistance exercises. Biol Sport. 2019;36(4):373-386.
Comacchio F, Mion M. Sneezing and perilymphatic fistula of the round window: case report and systematic review of the literature. J Int Adv Otol. 2018;14(1):106-111.
Goodhill V. Sudden deafness and round window rupture. Laryngoscope. 1971;81(9):1462-1474.
Haykowsky MJ, Eves ND, Warburton DE, Findlay MJ. Resistance exercise, the Valsalva maneuver, and cerebrovascular transmural pressure. Med Sci Sports Exerc. 2003;35(1):65-68.
Klokker M, Vesterhauge S. Perilymphatic fistula in cabin attendants: an incapacitating consequence of flying with common cold. Aviat Space Environ Med. 2005;76(1):66-68.
Matsuda H, Sakamoto K, Matsumura T, Saito S, Shindo S, Fukushima K, et al. A nationwide multicenter study of the cochlin tomo-protein detection test: clinical characteristics of perilymphatic fistula cases. Acta Otolaryngol. 2017;137(sup565):S53-S59.
Saliba I, Bawazeer N, Belhassen S. Suspicion and treatment of perilymphatic fistula: a prospective clinical study. Audiol Res. 2024;14(1):62-76.
Sarna B, Abouzari M, Merna C, Jamshidi S, Saber T, Djalilian HR. Perilymphatic fistula: a review of classification, etiology, diagnosis, and treatment. Front Neurol. 2020;11:1046.
Sasaki A, Ikezono T, Matsuda H, Araki R, Matsumura T, Saitoh S, et al. Prevalence of perilymphatic fistula in patients with sudden-onset sensorineural hearing loss as diagnosed by cochlin-tomoprotein (CTP) biomarker detection: its association with age, hearing severity, and treatment outcomes. Eur Arch Otorhinolaryngol. 2024;281(5):2373-2381.
Joonpyo Hong, MD is a board-certified otolaryngologist practicing in Korea. This article reflects his clinical interpretation of published research and does not constitute individual medical advice.