
A flat white patch inside the cheek that will not wipe off seems harmless. Yet pooled data from 55 studies and 41,231 patients show that roughly 1 in 15 oral leukoplakias eventually becomes cancer [Pimenta-Barros, Malignant transformation of oral leukoplakia: Systematic review and comprehensive meta-analysis, 2025]. This article explains what leukoplakia looks like, why it forms, how its danger changes from the mouth to the vocal cords, and how it is treated.
What Leukoplakia Actually Is
Leukoplakia is defined by the World Health Organization as a predominantly white plaque of questionable risk, diagnosed only after other known white lesions have been excluded. In plain terms, it is a white patch on a mucous membrane that cannot be scraped away and has no other explanation.
The key word is questionable. Leukoplakia is not cancer, but it is an oral potentially malignant disorder (OPMD) — a lesion that carries a real, measurable risk of turning into squamous cell carcinoma over time.
How It Forms: The Pathophysiology
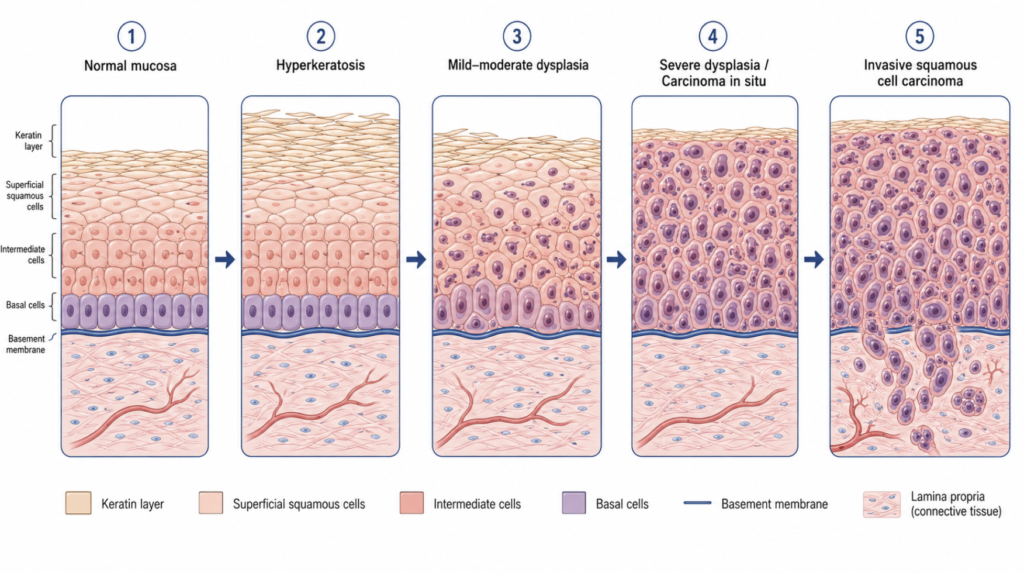
Mucosa responds to chronic irritation by thickening its keratin layer, a process called hyperkeratosis. That thickened keratin scatters light and looks white. Underneath, repeated injury and DNA damage can push some cells toward dysplasia — disordered, abnormal growth that is the biological step between healthy tissue and cancer.
The primary risk factors are tobacco (smoked and smokeless), alcohol, betel-nut chewing, and chronic friction, while certain viral infections (like HPV) and nutritional deficiencies may act as contributing factors. Dysplasia is the engine of risk: the higher its grade, the closer the lesion sits to malignancy.
What It Looks Like: Two Clinical Faces
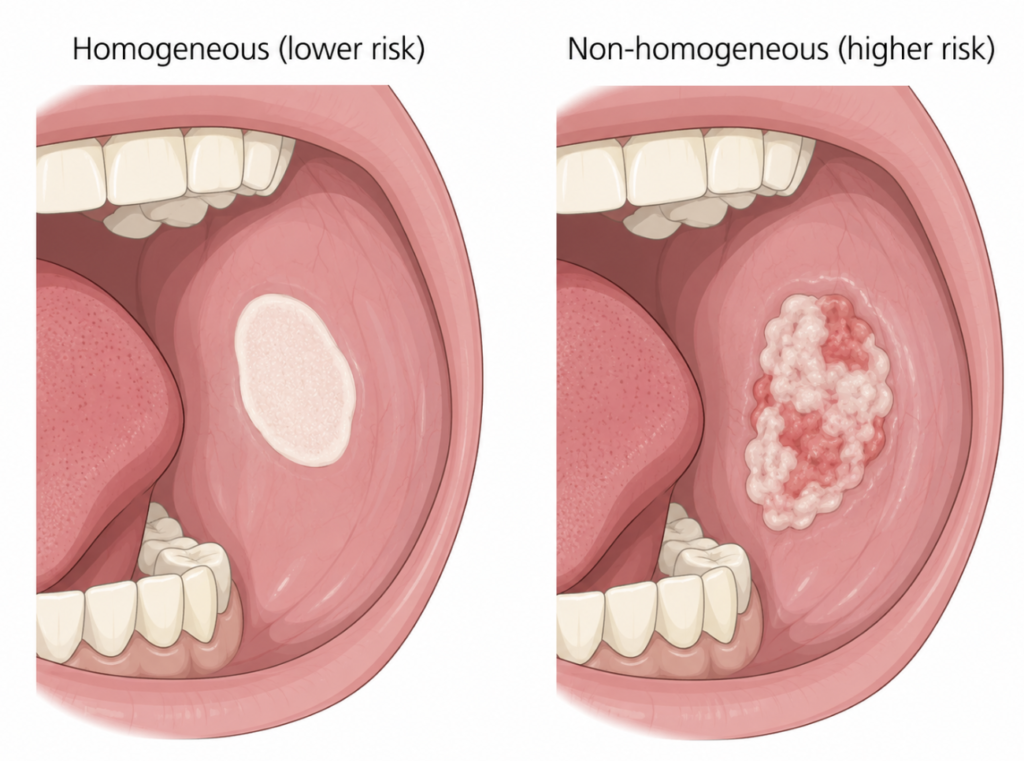
Clinicians sort leukoplakia by appearance, and appearance tracks risk closely.
Homogeneous (lower risk). A thin, flat, uniformly white plaque with a smooth or slightly wrinkled surface and well-defined edges. Usually painless and often stable.
Non-homogeneous (higher risk). Anything that breaks that uniform pattern:
- Speckled / erythroleukoplakia — mixed white and red areas
- Nodular — raised lumps within the patch
- Verrucous — a rough, wart-like surface
These often cause mild pain or a rough sensation. The distinction matters: in the 2025 meta-analysis, 21.88% of non-homogeneous lesions transformed versus 5.02% of homogeneous ones — a relative risk of 4.23 [Pimenta-Barros, Malignant transformation of oral leukoplakia: Systematic review and comprehensive meta-analysis, 2025].
A separate aggressive subtype, proliferative verrucous leukoplakia (PVL), appears as multiple patches, resists treatment, and carries a far higher transformation rate than ordinary leukoplakia. Any patient with multifocal, recurring white plaques deserves specialist referral.
Telling Leukoplakia Apart From Other White Patches
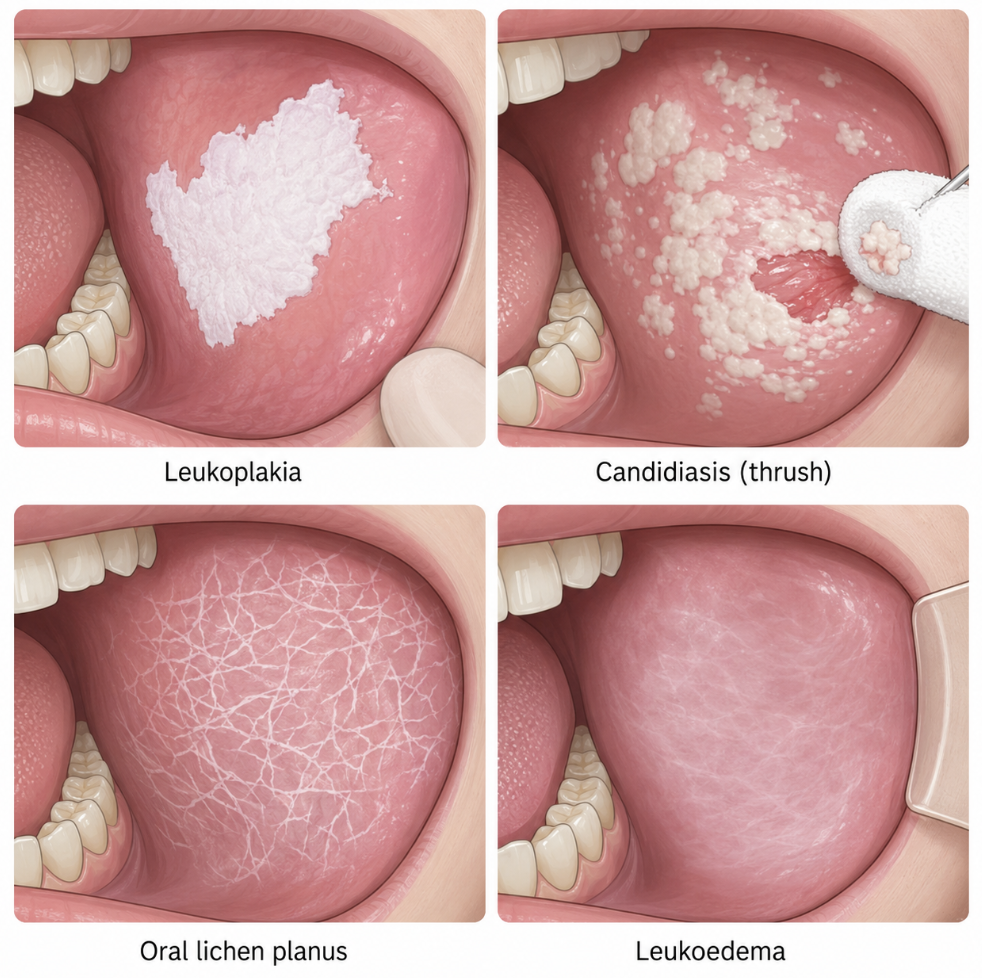
Not every white patch is leukoplakia, and the differences are practical:
- Oral thrush (candidiasis) wipes off, leaving a red base. Leukoplakia does not.
- Frictional keratosis sits exactly where a sharp tooth or denture rubs and fades once the irritant is removed.
- Oral lichen planus typically shows a lacy, net-like white pattern (Wickham’s striae) on both cheeks.
- Leukoedema is a faint, milky film that disappears when the cheek is stretched.
This is why the formal definition requires excluding known disorders first. A patch that resists wiping, has no obvious mechanical cause, and persists beyond two weeks should be examined rather than watched indefinitely.
Same Diagnosis, Different Site, Different Danger
A common question is whether leukoplakia in the mouth is the same disease as leukoplakia elsewhere. The histology — hyperkeratosis with or without dysplasia — is shared across mucosal sites. The risk, however, is not.
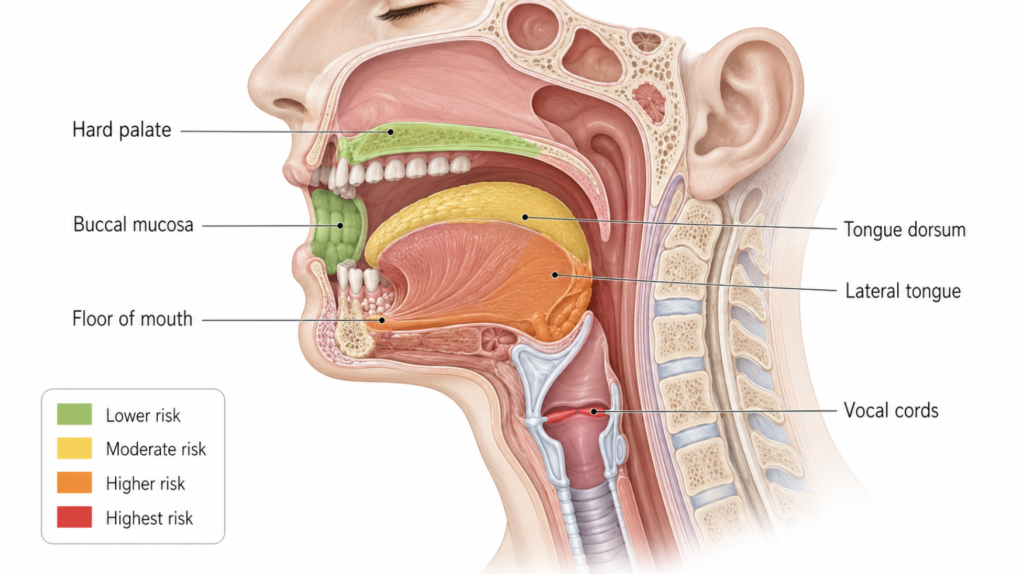
While limited by a smaller laryngeal sample size, a direct comparison from a Hungarian cohort of 253 patients (221 oral, 32 laryngeal) found a 10-year estimated malignant transformation of 15.1% for oral versus 42% for laryngeal lesions [Bukovszky, Malignant Transformation and Long-Term Outcome of Oral and Laryngeal Leukoplakia, 2023]. The directional finding aligns with older literature reporting laryngeal transformation rates anywhere from a few percent to over 60%. Within the mouth, the tongue and floor of mouth behave more aggressively than the cheek or palate [Guan, Malignant transformation rate of oral leukoplakia in the past 20 years: A systematic review and meta-analysis, 2023].
Clinical Perspective: Vocal cord leukoplakia is the quiet one. It produces no pain — only hoarseness — and a thin white streak on a vocal fold can be the sole warning of a higher-risk lesion. Persistent hoarseness lasting more than two weeks is a reason to look at the larynx, not to wait.
Leukoplakia on other mucosa, such as genital sites, is treated as a distinct entity with its own evaluation pathway and should not be assumed to behave like its oral or laryngeal form.
Which Leukoplakias Are Safe, and Which Are Not
Lower-risk features: homogeneous appearance, small size, cheek location, no dysplasia on biopsy, and improvement after stopping tobacco and alcohol. Without dysplasia, transformation rates fall to the low single digits [Bukovszky, Malignant Transformation and Long-Term Outcome of Oral and Laryngeal Leukoplakia, 2023].
Higher-risk features: non-homogeneous appearance, location on the tongue (especially lateral), floor of mouth, or vocal cords, larger size, moderate-to-severe dysplasia, and female sex [Guan, Malignant transformation rate of oral leukoplakia in the past 20 years: A systematic review and meta-analysis, 2023].
Clinical appearance alone cannot reliably predict malignancy. Biopsy is the essential step for diagnosis and risk stratification.
How Leukoplakia Is Treated
Management is matched to risk, not applied uniformly.
- Remove the cause first. Stopping tobacco and alcohol is the single most effective step, and many homogeneous lesions regress afterward.
- Biopsy any non-homogeneous lesion, or any lesion that changes — new ulceration or firmness can signal early cancer.
- Surveillance for low-risk, dysplasia-free lesions, typically every 3 to 12 months.
- Surgical removal for higher-risk lesions: cold-knife excision or CO2 laser in the mouth.
- In the larynx, voice-preservation microsurgery and angiolytic lasers have replaced old “vocal cord stripping,” which caused permanent hoarseness, while achieving comparable cancer control [Park, Laryngeal Leukoplakia: State of the Art Review, 2021].
Even after complete removal, leukoplakia can recur or transform at the same site, making long-term follow-up essential.
Key Takeaways
- Leukoplakia is a precancerous white mucosal patch, and about 6.6% of oral cases eventually become cancer.
- Non-homogeneous lesions transform roughly four times more often than homogeneous ones (21.88% vs 5.02%).
- Vocal cord leukoplakia appears more dangerous than oral; one comparative study estimated 10-year transformation near 42% versus 15.1%, and consistent direction has been reported elsewhere.
- Dysplasia grade, not appearance alone, is the strongest predictor of malignant transformation.
- First-line treatment is stopping tobacco and alcohol; biopsy and surgery follow for higher-risk lesions, with long-term monitoring.
FAQ
Is leukoplakia cancer?
No — leukoplakia is a potentially malignant lesion, not cancer itself. Most cases never transform, but a measurable minority do, which is why persistent patches are biopsied and monitored rather than ignored.
Will my mouth patch go away if I stop smoking?
Many homogeneous lesions improve or resolve after stopping tobacco and alcohol. Non-homogeneous or dysplastic lesions usually need more than lifestyle change, including biopsy and possible removal.
My only symptom is a hoarse voice — should I worry?
Persistent hoarseness beyond two weeks deserves a laryngeal exam. Vocal cord leukoplakia is typically painless, so hoarseness may be the only clue to a high-risk lesion.
Does surgery cure leukoplakia for good?
Not always. Lesions can recur or transform at the same site even after complete excision, so long-term follow-up remains necessary regardless of treatment.
References
Pimenta-Barros MA, et al. Malignant transformation of oral leukoplakia: Systematic review and comprehensive meta-analysis. Oral Dis. 2025.
Bukovszky B, Fodor J, Tóth E, et al. Malignant Transformation and Long-Term Outcome of Oral and Laryngeal Leukoplakia. J Clin Med. 2023.
Guan JY, Luo YH, Lin YY, et al. Malignant transformation rate of oral leukoplakia in the past 20 years: A systematic review and meta-analysis. J Oral Pathol Med. 2023;52(8):691-700.
Park JC, Altman KW, Prasad VMN, et al. Laryngeal Leukoplakia: State of the Art Review. Otolaryngol Head Neck Surg. 2021.