
In 2018 the U.S. Food and Drug Administration approved plazomicin, a new antibiotic built to defeat some of the most resistant bacteria in the hospital. Its developer, Achaogen, had spent roughly fifteen years getting it there. In its first six months on the market the drug took in less than one million dollars, and within about a year the company filed for bankruptcy (ACS Infectious Diseases, 2021).
A single antiviral pill tells the opposite story. Biktarvy, one of Gilead’s HIV medicines, sold about $13.4 billion in 2024 (Gilead, 2025) — on its own, roughly a quarter of the entire global antibiotics market.
Both are anti-infectives. Both fight microbes that make people sick. Yet their commercial and scientific worlds look almost inverted. The puzzle of antibiotics vs. antivirals is not a story about one heroic molecule and one unlucky company; the same property runs through all of it — the biology, the way the drugs are discovered, and the economics that decide which ones get made. The very feature that lets antibiotics be broad and used on a hunch is the feature that keeps antivirals narrow, expensive, and few. Bacteria are strangers a drug can strike; a virus is built from the body’s own cells — which is exactly why it is so hard to hit.
Same Goal, Different Battlefield
Both drug classes chase the dream Paul Ehrlich named more than a century ago: a magic bullet that strikes the invader and spares the patient. In pharmacology this is selective toxicity, and it is the whole game. The wider the gap between the dose that harms the microbe and the dose that harms the person, the safer and more useful the drug.
That gap is where bacteria and viruses part ways. A bacterium is a complete, self-contained cell. It builds its own wall, runs its own ribosomes, and copies itself with its own enzymes — machinery that human cells simply do not have. A virus is not a cell at all. It is a set of genetic instructions in a protein coat that must break into a host cell and borrow that cell’s machinery to make copies of itself (He et al., Host-Targeting Antivirals, 2023; De Clercq & Li, Approved Antiviral Drugs, 2016).
The consequence is structural, not incidental. An antibiotic can aim at a part that hundreds of bacterial species carry and humans lack, so selectivity is almost built into the target. An antiviral has to disable something inside a human cell without wrecking the cell wrapped around it. One drug class fights on foreign ground; the other fights on home soil, with the patient standing on the battlefield.
Clinical Perspective. The asymmetry is not a matter of effort or cleverness — it is set by where the pathogen lives. Any honest account of “why we don’t have more antivirals” has to begin here, because every later difficulty inherits from this one.
Reading the Molecules
The cleanest way to see the gap is to look at what real drugs actually grab onto.
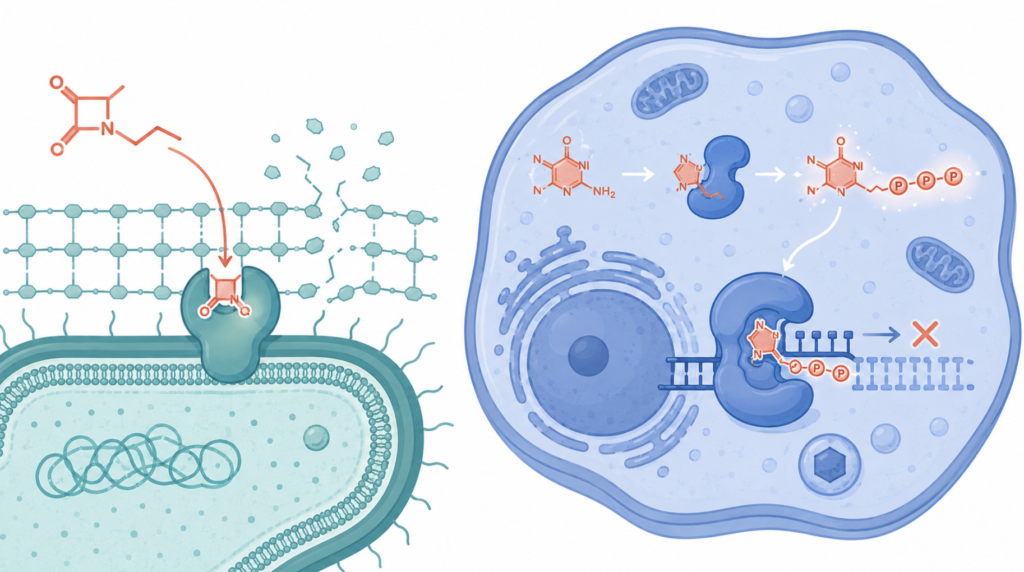
On the antibiotic side, the targets are parts the bacterium owns and the human body does not. β-lactams — penicillins and cephalosporins — lock covalently onto the enzymes that stitch the bacterial cell wall together, so the wall fails and the cell bursts; human cells have no such wall to defend (Mora-Ochomogo & Lohans, β-Lactam Targets and Resistance, 2021). Other antibiotics jam the bacterial ribosome, which differs from the human one, or block enzymes such as the bacterium’s own folate-making and DNA-coiling machinery. In each case the drug exploits a part of life that bacteria run and people borrow from their diet or build differently.
On the antiviral side, selectivity has to be engineered with more cunning, because the obvious targets belong to the host. Acyclovir, the workhorse against herpes and shingles, shows the trick at its most elegant. It is switched on — chemically activated — only by an enzyme the virus itself supplies, which exists mainly in infected cells; once activated, it shuts down the virus’s own copying enzyme. That double specificity is why a drug aimed at a virus hiding inside a host cell can still be unusually gentle on the rest of the body (Piret & Boivin, Resistance of Herpes Simplex Viruses to Nucleoside Analogues, 2011). The flu drugs zanamivir and oseltamivir mark another milestone: they were sculpted directly from the crystal structure of a viral surface enzyme’s active site, among the first medicines designed by looking at the target’s shape rather than by luck (von Itzstein et al., Rational Design of Sialidase Inhibitors, 1993). And HIV therapy stacks several inhibitors at once, each blocking a different viral enzyme — reverse transcriptase, integrase, protease (Arts & Hazuda, HIV-1 Antiretroviral Drug Therapy, 2012).
| Dimension | Antibiotics (example) | Antivirals (example) |
|---|---|---|
| Typical target | Bacterial cell wall, ribosome, bacterial enzymes (β-lactams) | One specific viral enzyme (acyclovir → viral DNA polymerase) |
| Is that target in human cells? | No — bacteria-only parts | The virus borrows host machinery; truly viral targets are scarce |
| How selectivity is achieved | Built into the target | Engineered (activation by a viral enzyme; structure-based design) |
| Spectrum | Often many species at once | Usually one virus or virus family |
The contrast resolves into a single image. A broad antibiotic is close to a master key, opening many locks because so many bacteria share the same lock. An antiviral is a key cut for one lock, and the next virus is a different lock entirely.
Clinical Perspective. Specificity is not a marketing weakness here; it is the source of these drugs’ safety. The same precision that makes acyclovir so well tolerated is what guarantees it will do nothing for influenza.
Two Ways to Find a Drug
How a drug is discovered follows from where its target sits, and the two histories diverged early.
Antibiotics came largely from nature. For decades the method was to grow bacteria on a plate, expose them to soil microbes and their products, and watch for whatever stopped the bacteria from growing — no need to know the molecular target in advance. The field leaned on these traditional discovery methods for a long time, and they delivered class after class of drugs (Cook & Wright, The Past, Present, and Future of Antibiotics, 2022). Because so many bacterial species share the same vulnerable parts, a single hit could work across many of them, which is why physicians can start a broad antibiotic on suspicion before any lab has named the exact bug.
Viruses refused that approach. A virus will not grow on a plate by itself; it needs living host cells to replicate, and for a long time there were no good systems to screen against. Antiviral discovery therefore became deliberate and target-based — cloning a viral enzyme, solving its structure, and designing a molecule to fit. That toolkit only matured alongside molecular virology and protein crystallography, and the HIV/AIDS crisis of the 1980s and 1990s is what forced it into being (De Clercq & Li, Approved Antiviral Drugs, 2016).
The arithmetic of the result is stark. Across roughly five decades after the first antiviral was approved in 1963 — a tally taken before the recent wave of COVID-19 drugs — only about ninety antiviral medicines had reached approval, and they covered just nine human diseases (De Clercq & Li, Approved Antiviral Drugs, 2016). That is on the order of ten drugs per disease, with almost all of them clustered on a short list of viruses, while antibiotics span dozens of chemical families and a far wider range of infections. Shared targets gave antibiotics breadth; unshared targets gave antivirals a separate research project for nearly every virus.
Clinical Perspective. Breadth and empiric use are two sides of one coin. An antibiotic can be reasonable before a culture comes back precisely because its target is common; an antiviral rarely can, because the right drug depends entirely on which virus is present.
Resistance Writes the Rules
Microbes fight back, and how they resist shapes how each class is used.
Viruses, especially those that store their genes as RNA, copy themselves sloppily and mutate fast, throwing off variants that can shrug off a drug (He et al., Host-Targeting Antivirals, 2023; Arts & Hazuda, HIV-1 Antiretroviral Drug Therapy, 2012). For HIV this is not a footnote but a founding constraint: a single drug would be outrun within months, so treatment was built from the start as a combination of agents hitting different steps at once (Arts & Hazuda, HIV-1 Antiretroviral Drug Therapy, 2012). Bacteria resist too — some manufacture enzymes that chop β-lactam drugs apart before they can act (Mora-Ochomogo & Lohans, β-Lactam Targets and Resistance, 2021) — yet many bacterial infections are still treated with a single agent.
There is a frontier worth naming without overselling it. Rather than chasing one virus at a time, some researchers are pursuing host-targeting antivirals, aimed at cellular factors that many different viruses depend on, in the hope of one drug that reaches across several of them. This is an active line of investigation rather than a delivered class of medicines, and its central trade-off — touching the host’s own machinery raises the risk of harming the host — is exactly the selective-toxicity problem returning in a new form (He et al., Host-Targeting Antivirals, 2023).
The rule underneath both stories is uncomfortable. The better and more precise the target, the more a single mutation can take it away.
Same Size, Opposite Shape
The economics is where the puzzle from the opening finally makes sense, and the surprise is that it does not start with size.
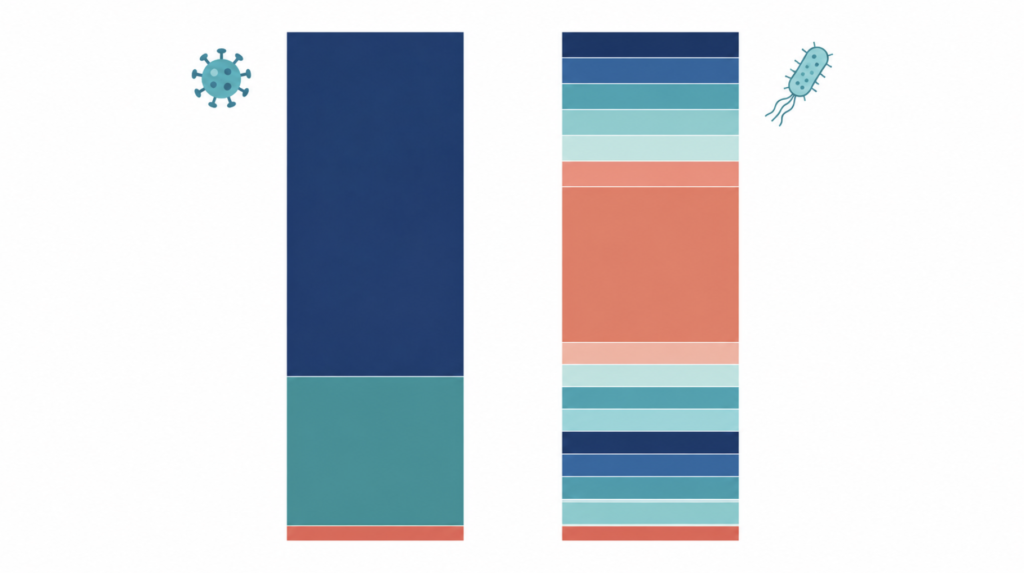
In aggregate the two markets are roughly the same order of magnitude. Industry analyses place the global antibiotics market and the global antiviral market each in the broad range of about $40–66 billion for 2024–2025, with wide variation between firms and definitions. So the shortage of new drugs is not a story of one tiny market. It is a story of opposite shapes.
Antivirals are concentrated in a few blockbusters. HIV medicines alone make up more than half of antiviral sales, and a single product, Biktarvy, sold about $13.4 billion in 2024 (Gilead, 2025). Put plainly, one antiviral pill out-earns the world’s entire effort at new antibiotics several times over. These are chronic, often lifelong treatments with durable pricing — the commercial opposite of a three-day course.
Antibiotics, by contrast, are dominated by cheap generics — roughly four-fifths of sales — and the innovative end of the business has effectively collapsed. A newly approved antibiotic, plazomicin, earned under $1 million in six months; other recent launches brought in around $11 million in their first year, against an estimated $300 million a year needed merely to be sustainable (npj Antimicrobials and Resistance, 2025). The modeled private value of a new antibiotic at discovery runs from slightly negative to about $37 million, while a new drug for a chronic, non-infectious disease can be worth on the order of a billion (ACS Infectious Diseases, 2021). Most small companies that actually brought an antibiotic to market since 2010 went bankrupt or exited at a loss (Humanities and Social Sciences Communications, 2024).
| Dimension | Antibiotics | Antivirals |
|---|---|---|
| Total market (2024–25, industry estimates) | ~$40–55B | ~$40–66B |
| Revenue shape | Generic-dominated, low margin | Concentrated in a few blockbusters |
| Exemplar | New launch earned <$1M in 6 months | Biktarvy ≈ $13.4B in 2024 |
| Generic share | ~80% of sales | Branded innovators dominate |
| New-entrant economics | Private value near zero or negative | Durable where the virus is chronic |
Even antiviral riches can be fragile, which is the honest other half of the picture. Hepatitis C offers the strangest case: the cures were so effective that they shrank their own market as patients were cured and not replaced (industry reporting, 2016). And Paxlovid fell from about $18.9 billion in 2022 to roughly $1 billion in 2023 as the pandemic ebbed, with Pfizer even reversing $4.2 billion in revenue when the U.S. government returned millions of unused courses. The durable money in antivirals lives almost entirely in chronic, lifelong infection — HIV above all.
Clinical Perspective. The market is not rewarding the most clinically valuable drug; it is rewarding the most repeatedly purchased one. A medicine taken for life beats a medicine taken for a week, and a medicine deliberately held in reserve to slow resistance is punished for its own virtue.
Same Disease, Different Symptoms
Stepping back, the two stories turn out to be one. Acute, self-limiting infections do not sustain a market. That single fact surfaces twice — as the scarcity of antivirals for short viral illnesses, and as the financial collapse of novel antibiotics. The difference is that antivirals found an escape hatch and antibiotics largely did not. Chronic viruses such as HIV and hepatitis B and C created lifelong, high-value markets that pulled enormous investment; bacterial infections, mostly acute and increasingly met with drugs we are told to use sparingly, offered no such refuge.
The clinical corollary is the part patients feel directly. For the common cold and most sore throats there is no targeted antiviral at all, and national guidance is explicit that antibiotics should not be prescribed for the common cold, because they do nothing against a virus (Harris et al., Appropriate Antibiotic Use for Acute Respiratory Tract Infection, 2016). “No prescription” is frequently the most accurate thing a clinician can say.
The proposed fixes follow the diagnosis. On the economic side, the leading idea is to decouple a new antibiotic’s reward from its sales volume — paying for its value to public health through subscription-style arrangements, so that a drug held in reserve is still worth developing. On the scientific side, broader-spectrum strategies and faster, more specific diagnostics would make narrow drugs usable by telling clinicians exactly which microbe, and when (Cook & Wright, The Past, Present, and Future of Antibiotics, 2022).
Clinical Perspective. The scarcity of antivirals and the drought of new antibiotics are not two problems but one wearing two faces. Bacteria were strangers, and a drug could strike them; viruses were built from the body itself, and it could not — and the market, indifferent to clinical need, finished what biology started. Understanding that is what lets a clinician explain, without apology, why the right answer to an ordinary cold is rest and time rather than a pill.
Key Takeaways
- A broad antibiotic can treat many bacterial infections at once, while each antiviral usually works against a single virus.
- The root cause is biological: bacteria are foreign cells with their own targets, whereas viruses hijack our cells, leaving few safe targets to attack.
- Discovery method followed from biology — antibiotics from natural-product screening, antivirals from deliberate, structure-based design that only matured during the HIV era.
- The antibiotic and antiviral markets are similar in total size but opposite in shape: a single HIV pill out-earns the entire effort to develop new antibiotics, which is commercially broken.
- One fact unites both: acute, self-limiting infections do not sustain a market — antivirals escaped through chronic viruses, antibiotics mostly did not.
- For an everyday cold, neither an antibiotic nor an antiviral is indicated; supportive care is the standard.
FAQ
Why is there no antiviral for the common cold? There is none because of biology and economics together. The cold’s viruses offer few safe targets to attack, each would need its own drug, and a short, self-limiting illness cannot repay the cost of one. Care focuses on relieving symptoms while the immune system clears the infection (De Clercq & Li, Approved Antiviral Drugs, 2016).
Are antivirals just the antiviral version of antibiotics? No. Antibiotics often work across many bacterial species, while antivirals are typically built for one virus and do not transfer. A flu antiviral and a COVID-19 antiviral are not interchangeable, because each is approved only for its specific virus (De Clercq & Li, Approved Antiviral Drugs, 2016).
If new antibiotics are so needed, why don’t companies make them? Mostly because they lose money. A new antibiotic’s modeled value at discovery can be near zero or negative, and recent launches earned a few million dollars when hundreds of millions are needed to break even, driving developers into bankruptcy (ACS Infectious Diseases, 2021; npj Antimicrobials and Resistance, 2025).
Will broad-spectrum antivirals ever exist? Possibly, but not yet. Researchers are actively exploring host-targeting drugs aimed at factors many viruses share, though the approach risks harming the host’s own cells and remains a research direction rather than an available class of medicines (He et al., Host-Targeting Antivirals, 2023).
References
- von Itzstein M, Wu WY, Kok GB, et al. Rational design of potent sialidase-based inhibitors of influenza virus replication. Nature. 1993;363(6428):418-423.
- Mora-Ochomogo M, Lohans CT. β-Lactam antibiotic targets and resistance mechanisms: from covalent inhibitors to substrates. RSC Med Chem. 2021;12(10):1623-1639.
- Piret J, Boivin G. Resistance of herpes simplex viruses to nucleoside analogues: mechanisms, prevalence, and management. Antimicrob Agents Chemother. 2011;55(2):459-472.
- Arts EJ, Hazuda DJ. HIV-1 antiretroviral drug therapy. Cold Spring Harb Perspect Med. 2012;2(4):a007161.
- He Y, Zhou J, Gao H, Liu C, Zhan P, Liu X. Broad-spectrum antiviral strategy: host-targeting antivirals against emerging and re-emerging viruses. Eur J Med Chem. 2023;265:116069.
- De Clercq E, Li G. Approved antiviral drugs over the past 50 years. Clin Microbiol Rev. 2016;29(3):695-747.
- Harris AM, Hicks LA, Qaseem A. Appropriate antibiotic use for acute respiratory tract infection in adults: advice for high-value care from the American College of Physicians and the Centers for Disease Control and Prevention. Ann Intern Med. 2016;164(6):425-434.
- Cook MA, Wright GD. The past, present, and future of antibiotics. Sci Transl Med. 2022;14(657):eabo7793.
- Cama J, Leszczynski R, Tang PK, Khalid A, Lok V, Dowson CG, Ebata A. To push or to pull? In a post-COVID world, supporting and incentivizing antimicrobial drug development must become a governmental priority. ACS Infect Dis. 2021;7(8):2029-2042. https://pubs.acs.org/doi/10.1021/acsinfecdis.0c00681
- Gargate N, Laws M, Rahman KM. Current economic and regulatory challenges in developing antibiotics for Gram-negative bacteria. npj Antimicrob Resist. 2025;3:50. https://www.nature.com/articles/s44259-025-00123-1
- Wells N, Nguyen VK, Harbarth S. Novel insights from financial analysis of the failure to commercialise plazomicin: implications for the antibiotic investment ecosystem. Humanit Soc Sci Commun. 2024;11:941. https://www.nature.com/articles/s41599-024-03452-0
- Gilead Sciences. Gilead Sciences announces fourth quarter and full year 2024 financial results. February 11, 2025. https://www.gilead.com/news/news-details/2025/gilead-sciences-announces-fourth-quarter-and-full-year-2024-financial-results
- Pfizer Inc. Pfizer amends U.S. government Paxlovid supply agreement and updates full-year 2023 guidance. October 13, 2023. https://www.pfizer.com/news/press-release/press-release-detail/pfizer-amends-us-government-paxlovid-supply-agreement-and
- Grand View Research. Antibiotics market size, share & trends report, 2024 (generic share ~81%): https://www.grandviewresearch.com/industry-analysis/antibiotic-market — and Anti-infective agents market report, 2024 (antiviral segment ~51%): https://www.grandviewresearch.com/industry-analysis/anti-infective-agents-market (industry estimates vary by definition).
Joonpyo Hong, MD is a board-certified otolaryngologist practicing in Korea. This article reflects his clinical interpretation of published research and does not constitute individual medical advice.
For more interesting contents:
https://curiousmd.com/antivirals-vs-antibiotics-why-so-few/