
A patient with a three-day-old cold leans forward and asks a question that comes up every winter: “It’s a virus, right? So can I get an antiviral?” It’s a fair question. After years of headlines about COVID-19 pills and flu medication, many people assume viruses, like bacteria, have a shelf of drugs waiting for them. They usually don’t. This is the heart of the antivirals vs. antibiotics question: why one antibiotic can treat dozens of different infections while antivirals are reserved for a short list of specific situations—and why we can’t simply build one antiviral for every virus.
Bacteria and Viruses Are Not the Same Kind of Enemy
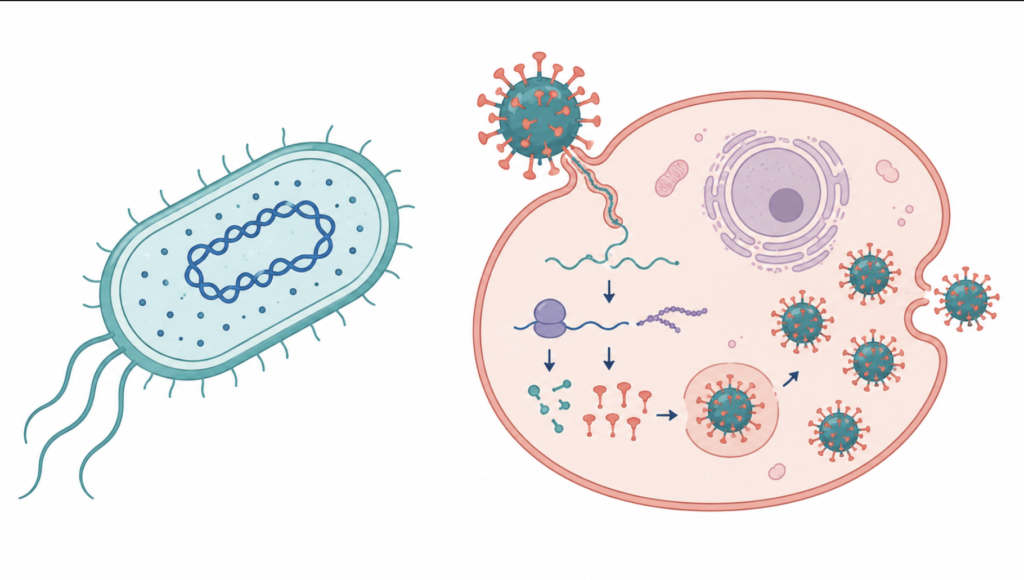
The reason the two drug types aren’t interchangeable starts with basic biology. Bacteria are complete, self-sufficient cells: they make their own energy, build their own proteins, and copy themselves. Viruses are not cells at all. A virus is essentially a set of genetic instructions in a protein shell that has to break into one of your cells and borrow its machinery to reproduce.
That single difference shapes everything else. Antibiotics work by attacking structures that bacteria have but human cells do not—the bacterial cell wall, the bacterial ribosome, specific bacterial enzymes. Because many different bacterial species share those same structures, one antibiotic can treat a sinus infection, a urinary tract infection, and a skin infection. Antibiotics do nothing to viruses, and antivirals do nothing to bacteria; they are aiming at completely different targets.
One Antibiotic, Many Infections—One Antiviral, One Virus
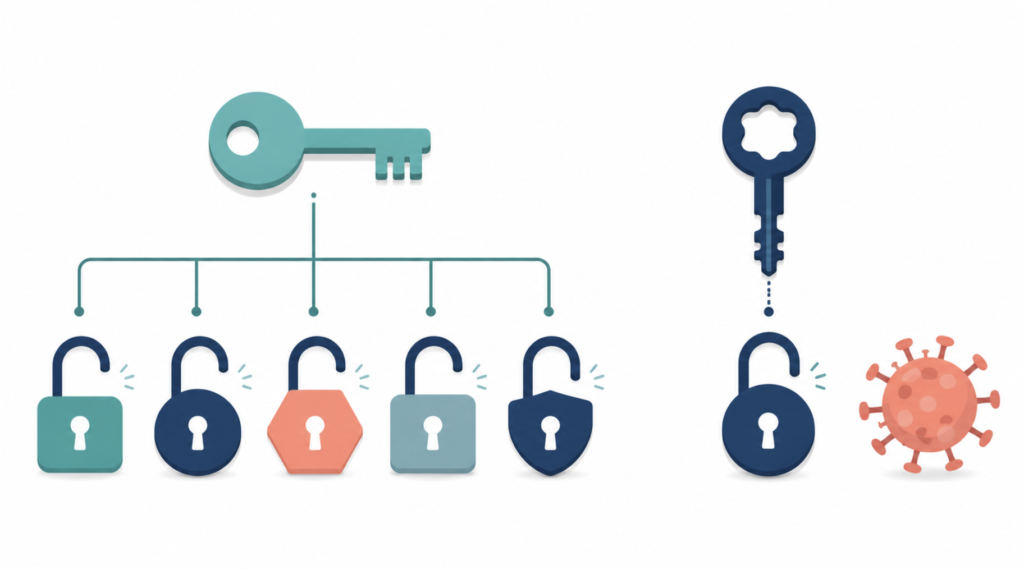
Here is the asymmetry that surprises most people. A broad-spectrum antibiotic is like a master key that opens many locks. An antiviral is more like a key cut for a single lock.
Concretely: a flu antiviral will not treat COVID-19, and a COVID-19 antiviral is not approved to treat the flu—even though both are respiratory viruses you might catch in the same week. Each antiviral is built to jam one specific step in one specific virus’s life cycle. Drugs for HIV, for instance, are grouped by the exact viral step they block, such as reverse transcriptase, integrase, or protease [Arts, HIV-1 Antiretroviral Drug Therapy, 2012]. A drug that blocks HIV’s integrase has nothing to grab onto in an influenza virus.
The numbers make the gap vivid. A comprehensive review found that in the roughly five decades after the first antiviral was approved in 1963, only about 90 antiviral drugs had reached approval—and they covered just nine human diseases, including HIV, hepatitis B and C, herpes, and influenza [De Clercq, Approved Antiviral Drugs Over the Past 50 Years, 2016]. That tally was compiled before the recent wave of COVID-19 antivirals, but the basic imbalance against the much larger and more varied shelf of antibiotics still holds.
So Why Not Just Make One Antiviral for Every Virus?
This is the natural follow-up, and the honest answer has two layers.
Layer one: they are genuinely hard to make
Because a virus hides inside your cells and runs on your machinery, there is very little that belongs to the virus alone for a drug to attack. A useful antiviral has to disable the virus without poisoning the healthy cell wrapped around it [He, Broad-Spectrum Antiviral Strategy: Host-Targeting Antivirals Against Emerging and Re-Emerging Viruses, 2023]. Bacteria, sitting outside our cells with their own distinct parts, offer far easier and safer targets.
Viruses are also strikingly different from one another—some store their genes as DNA, others as RNA, with little in common between families. A drug shaped to fit one virus’s protein usually finds nothing to grip on the next, which is why broad-spectrum antivirals are rare and most drugs must be designed almost from scratch for each virus. Viruses also mutate quickly and can evolve resistance, shortening the useful life of any drug that does reach the market. Even so, broader-spectrum antivirals are an active research goal: approaches such as host-targeting antivirals—aimed at cellular factors that many different viruses depend on—are being actively explored as a way to reach more viruses with a single drug [He, Broad-Spectrum Antiviral Strategy: Host-Targeting Antivirals Against Emerging and Re-Emerging Viruses, 2023].
Layer two: the economics discourage it
Even when a drug is scientifically possible, someone has to pay to develop it, and the math is often discouraging. Bringing a new anti-infective through development costs an enormous amount, yet many of the infections it would treat are short and self-limiting—an ordinary cold or flu clears on its own in days—so the commercial reward is small. This is not unique to antivirals; the same weak economics have pushed many companies away from antibiotic development as well. A “one drug, one virus” model splits an already thin market into smaller pieces still, and viruses that appear only in sporadic outbreaks offer almost no predictable market at all.
Put the two layers together and antivirals sit in an unlucky spot: among the hardest medicines to invent and among the least rewarding to sell. It isn’t a lack of effort—it’s biology and economics pulling in the same direction.
When Are Antivirals Actually Used?
Antivirals shine in specific scenarios, not as a catch-all. They exist mainly for a defined set of viruses—influenza, herpes and shingles, HIV, hepatitis B and C, cytomegalovirus, and COVID-19, among a few others [De Clercq, Approved Antiviral Drugs Over the Past 50 Years, 2016].
Timing matters, too. Antivirals work by slowing viral copying, so they help most when started early, while the virus is still ramping up. They are also frequently reserved for people at higher risk of complications—older adults, those with weakened immune systems, or significant underlying illness—rather than every healthy person with mild symptoms.
For the everyday viral infections an ENT clinic sees most—the common cold and most sore throats—there is usually no targeted antiviral at all, and the standard of care is rest, fluids, and symptom relief. Antibiotics are no substitute, because they have no effect on viruses; national guidance is explicit that antibiotics should not be prescribed for the common cold [Harris, Appropriate Antibiotic Use for Acute Respiratory Tract Infection in Adults, 2016].

Clinical Perspective
For most viral infections—the common cold and the majority of sore throats—no prescription is the appropriate course, even though patients often expect one. Antibiotics are still prescribed for clearly viral infections, where they provide no benefit and only push bacteria toward resistance [Harris, Appropriate Antibiotic Use for Acute Respiratory Tract Infection in Adults, 2016]. Recognizing that antivirals are special-purpose tools, reserved for specific viruses and specific situations, helps set realistic expectations and preserves antibiotics for the bacterial infections that truly need them.
Key Takeaways
- Antibiotics can treat many different bacterial infections, but each antiviral usually works against only one specific virus.
- Antivirals are scarce because viruses hijack our own cells, leaving few safe targets to attack.
- A flu antiviral will not treat COVID-19, and a COVID-19 antiviral will not treat the flu.
- Antivirals are special-situation drugs: most effective when started early, and often reserved for higher-risk patients.
- A common cold needs neither an antibiotic nor an antiviral—supportive care is the standard.
FAQ
Why can’t I take an antiviral for a cold? For the common cold there simply is no targeted antiviral to take. Colds are usually caused by rhinoviruses, for which no specific drug exists, so treatment focuses on easing symptoms while your immune system clears the infection. Antibiotics won’t help either, since they only work on bacteria.
Are antivirals just the antiviral version of antibiotics? Not really. Antibiotics often work against many bacteria at once, while antivirals are usually built for a single virus and won’t work on others. The two attack entirely different kinds of targets, which is why one type cannot stand in for the other.
Why isn’t there an antiviral for every virus? Because viruses copy themselves using our own cells, a drug struggles to hit the virus without harming the cell, and each virus differs enough to need its own drug [He, Broad-Spectrum Antiviral Strategy: Host-Targeting Antivirals Against Emerging and Re-Emerging Viruses, 2023]. The high development cost and small markets for many viral illnesses add a second barrier.
Does a flu antiviral still help if I start it late? Antivirals slow viral replication, so they generally help most when started early in the illness. Started late, after the virus has already peaked, the benefit is smaller. Decisions about timing and whether an antiviral is appropriate are best made with your own clinician.
References
De Clercq E, Li G. Approved antiviral drugs over the past 50 years. Clin Microbiol Rev. 2016;29(3):695-747.
He Y, Zhou J, Gao H, Liu C, Zhan P, Liu X. Broad-spectrum antiviral strategy: host-targeting antivirals against emerging and re-emerging viruses. Eur J Med Chem. 2023;265:116069.
Arts EJ, Hazuda DJ. HIV-1 antiretroviral drug therapy. Cold Spring Harb Perspect Med. 2012;2(4):a007161.
Harris AM, Hicks LA, Qaseem A. Appropriate antibiotic use for acute respiratory tract infection in adults: advice for high-value care from the American College of Physicians and the Centers for Disease Control and Prevention. Ann Intern Med. 2016;164(6):425-434.
Joonpyo Hong, MD is a board-certified otolaryngologist practicing in Korea. This article reflects his clinical interpretation of published research and does not constitute individual medical advice.
For more interesting contents:
https://curiousmd.com/acetaminophen-vs-nsaids-evidence/
https://curiousmd.com/cough-that-wont-go-away-after-a-cold/