
Facial and neck lacerations look like suturing problems. Often they aren’t. A clean cut across the cheek can sever the facial nerve or transect the parotid duct; a few centimeters lower, the same blade opens the platysma into a vascular emergency. The most expensive mistakes in wound care are rarely the visible scar — they are the deep structure no one examined before closing.
This article is about lacerations — clean, linear cuts. It does not cover avulsions, flaps, abrasions, or wounds with significant tissue loss. Those involve devitalized edges, debris impregnation, or missing tissue, and they demand grafting or local-flap reconstruction that follows a different logic. Here the question is narrower and more useful: for each anatomic site, what must you rule out before you pick up a needle, and what changes your management?
Before suturing: the part that isn’t suturing
Every facial and neck laceration starts the same way. Assess airway, breathing, and circulation first; facial and neck trauma can hide an airway threat behind a “distracting” laceration. Take a focused history — timing, mechanism, and social context, since assault and domestic violence are common and medicolegally important. Then irrigate copiously, inspect for foreign bodies, and examine for damaged critical structures (nerves, ducts, cartilage) before anything else.
Two practical points, on timing and on prophylaxis. Facial skin is highly vascular, so primary closure of a clean wound can reasonably be considered up to roughly 12–24 hours after injury — but the “golden time” is not a fixed number. It should flex with the degree of contamination and tissue damage, and a grossly contaminated wound may be better served by delayed closure.
Antibiotics, meanwhile, are not routine — reserve them for exposed cartilage, through-and-through mucosal wounds, bites, open fractures, or immunosuppression. The specific agent and duration should defer to each institution’s clinical protocol and formulary and to the individual patient’s condition, rather than to any single rule. Structured wound-closure training measurably lowers early complication rates, which tells you the technique is learnable and the details matter [Yamamoto, Early Complications Following Facial Laceration Repair Performed by Emergency Physicians, 2018].
Face: a different question at each subunit
The face is built from aesthetic and functional subunits, and each one hides a structure you can quietly ruin [Sabatino, Facial Wound Management, 2013]. The table below is the decision spine; the high-stakes pearls follow.
| Subunit | Rule out first | How to check | Key action |
|---|---|---|---|
| Forehead | Facial nerve temporal branch, frontal sinus, supraorbital nerve, galea | Brow-elevation symmetry; CT if deep or over the sinus | Repair galea as a separate layer |
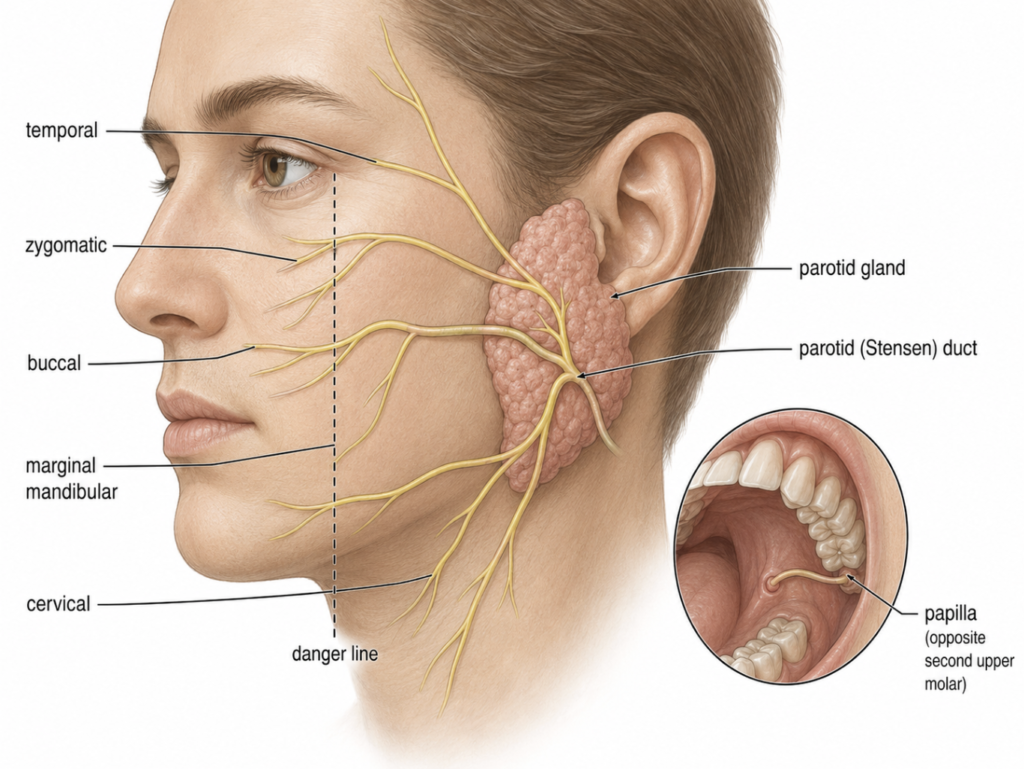
| Cheek | Facial nerve (buccal/zygomatic), parotid (Stensen) duct | Motor exam; intraoral duct papilla, milk/probe the duct | Refer nerve or duct injury for operative repair |
| Auricle | Cartilage exposure, subperichondrial hematoma | Inspect and palpate for fluctuance | Drain any hematoma immediately; cover bare cartilage |
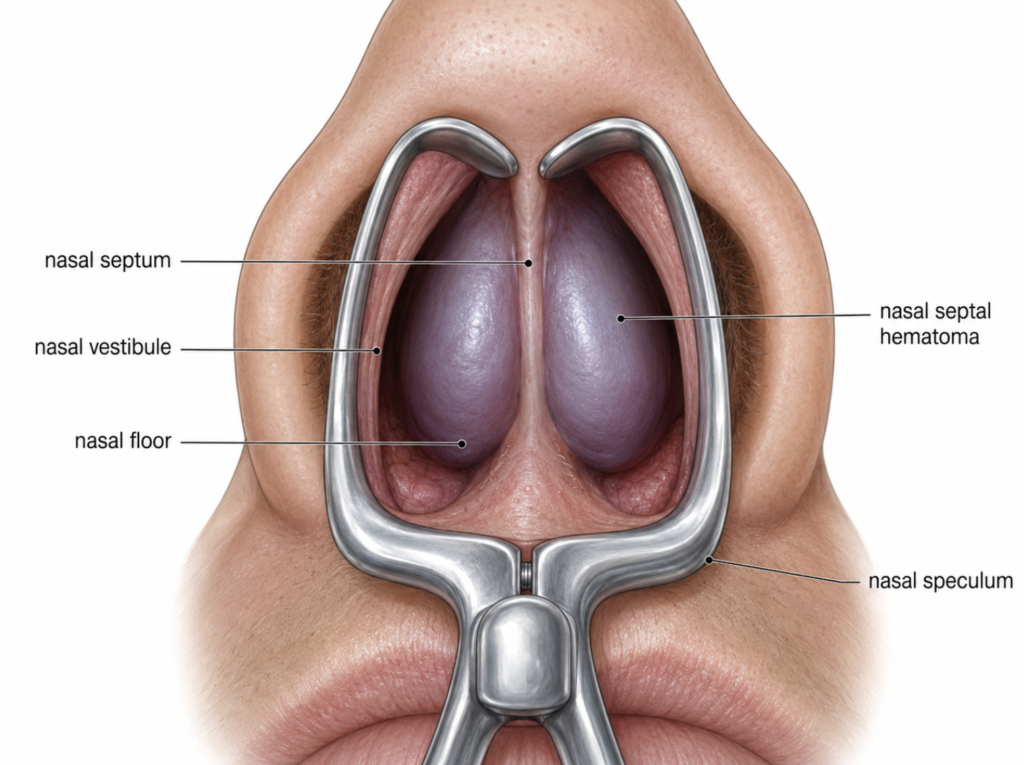
| Nose | Septal hematoma, cartilage, nasal-bone fracture | Speculum/otoscope inside both nares | Drain a septal hematoma immediately |
| Lip | Vermilion malalignment, orbicularis oris, through-and-through | Inspect the border; test muscle continuity | Align the vermilion border first |
| Tongue | Airway, ongoing bleeding, lingual artery | Inspect size, gaping, bleeding | Repair only by indication (see below) |
| Oral mucosa | Stensen duct (buccal wounds), through-and-through, tooth injury | Duct papilla opposite 2nd upper molar; dental exam | Selective antibiotics; refer duct injury |
Nose — the one you cannot afford to miss. Always look inside the nose. A nasal septal hematoma is a boggy, often bluish swelling of the septum, and if it isn’t drained it can necrotize the cartilage and collapse the dorsum into a saddle nose. Drainage is the emergency, not the skin closure.
Auricle — drain first, suture second. The ear’s skin lies directly over avascular cartilage that feeds through the perichondrium. A subperichondrial hematoma strips that blood supply; left alone it organizes into “cauliflower ear.” Evacuate it and apply a bolster before you close skin [Sabatino, Facial Wound Management, 2013].
Cheek — two structures, one line. Picture a vertical line down from the lateral canthus. A deep cheek laceration lateral to it can divide a major branch of the facial nerve, or the parotid (Stensen) duct, which runs toward a papilla opposite the second upper molar. Both are easy to miss and costly to ignore — an unrecognized duct transection leads to a sialocele or salivary fistula [Mardani, Surgical Management of Parotid Duct Injury Using a Feeding Tube, 2020]. Test facial motor function and inspect the duct papilla; if either is involved, this is an operative referral, not an ED closure.
Lip — the millimeter that everyone sees. The vermilion border is the most unforgiving landmark on the face; a 1 mm step-off is visible across a room. Align it with the first stitch, before anything else, and repair through-and-through lip wounds in layers [Tsao, Emergency Facial Injuries in Athletics, 2023].
Tongue — most don’t need stitches. Many tongue lacerations heal well on their own. Reserve repair for wounds that are large or gaping, bisect the tongue, involve the free edge, or keep bleeding — after airway and hemostasis are secured [Tsao, Emergency Facial Injuries in Athletics, 2023].
Neck: stop before you probe
The neck flips the priority order. Here the cut itself is the smaller problem; what lies beneath — carotid, jugular, trachea, esophagus — is the emergency. The first decision is binary: does the wound penetrate the platysma? If it does, never blindly probe or explore it at the bedside. You can dislodge a clot and convert a contained injury into a catastrophe.
Sort findings into hard signs and soft signs. Hard signs — expanding or pulsatile hematoma, active bleeding, bruit or thrill, airway compromise, massive subcutaneous emphysema, or hematemesis — point toward the operating room. Soft signs (minor non-expanding hematoma, mild dysphagia, dysphonia, a little subcutaneous air) warrant imaging in a stable patient.
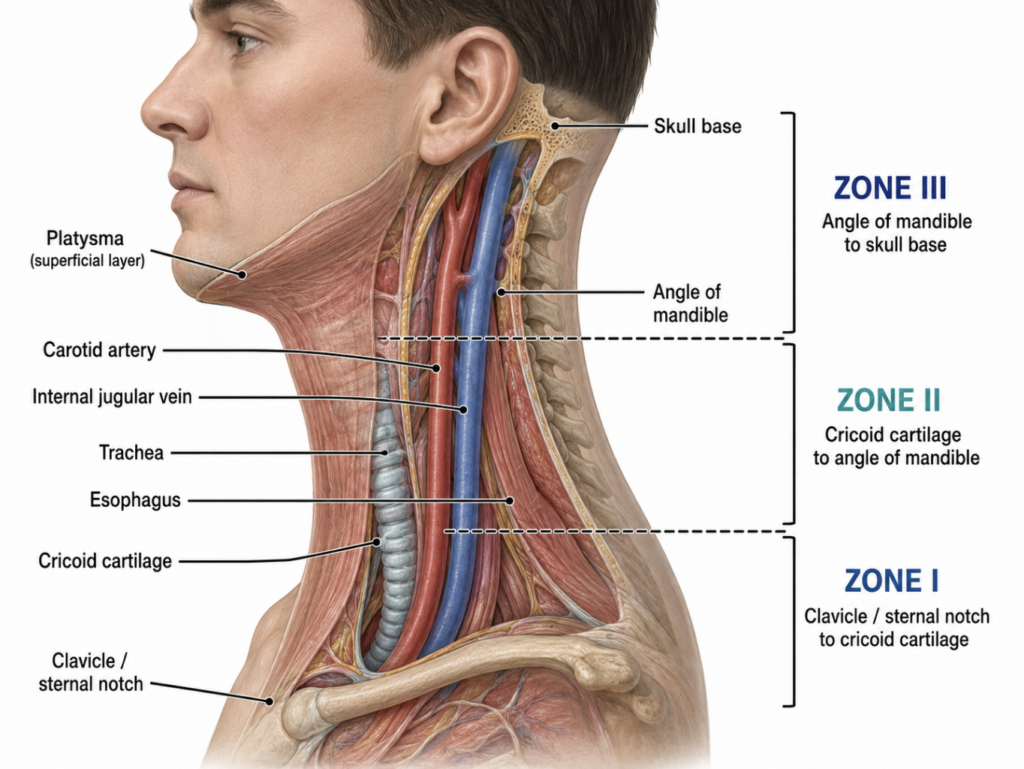
Classic teaching divides the neck into three zones, and the zone still shapes what you worry about and how you image:
- Zone I — sternal notch/clavicle to the cricoid cartilage. Great vessels, lung apices, trachea, and esophagus crowd this thoracic-outlet region; injuries here need vascular plus aerodigestive evaluation.
- Zone II — cricoid to the angle of the mandible. The most common and the most surgically accessible zone. Stable patients are imaged; hard signs go to exploration.
- Zone III — angle of the mandible to the skull base. The distal carotid here is hard to expose surgically, so vascular injuries often lean on angiography and endovascular options.
Modern practice has shifted from “operate by zone” toward a physical-exam-driven, “no-zone” approach in stable patients, with CT angiography (CTA) as the workhorse. A systematic review found CTA combined with examination reliably sensitive and specific for detecting injuries in stable penetrating-neck-trauma patients with soft signs [Ibraheem, Computed Tomography Angiography in the “No-Zone” Approach Era for Penetrating Neck Trauma, 2020]. That said, the zones are far from obsolete. The no-zone approach governs whether to image a stable patient, but the anatomic zone classification remains the shared language for deciding surgical access and for communicating with consulting services such as general and thoracic surgery [Petrone, Diagnosis Management and Treatment of Neck Trauma, 2019]. The balance to strike is using the exam to trigger imaging while still describing the injury by zone when you pick up the phone.
Clinical Perspective
The reflex with a facial cut is to think about the scar. Reverse it. Clear the dangerous structures first — septum, parotid duct, facial nerve, and, in the neck, the platysma — and then think cosmesis. A patient forgives a fine-line scar far more readily than a saddle nose, a drooping lip, or a salivary fistula that could have been caught with a thirty-second exam at the first visit.
Key Takeaways
- Nose laceration: rule out a septal hematoma first and drain it — delay can collapse the dorsum.
- Ear laceration: evacuate any subperichondrial hematoma before closing to prevent cauliflower ear.
- Cheek and oral lacerations: examine the facial nerve and the parotid (Stensen) duct before suturing.
- Lip laceration: align the vermilion border with the first stitch.
- Neck laceration: if it penetrates the platysma, do not probe it — image stable patients with CTA and triage by hard versus soft signs.
FAQ
When does a facial laceration need imaging? When it is deep over the frontal sinus, when there is concern for an underlying facial-bone fracture, or when the exam suggests injury to a structure you cannot directly visualize. Most simple facial lacerations need no imaging; palpation and inspection usually suffice.
How do you check for a parotid duct injury? Examine the duct papilla inside the cheek, opposite the second upper molar, for bleeding or clear/salivary leakage, and gently probe or milk the gland if injury is suspected. Deep cheek wounds lateral to a line dropped from the lateral canthus are the high-risk ones, and suspected duct injuries go to operative repair.
Why drain a septal or auricular hematoma immediately? Both sit on cartilage that depends on an overlying blood supply. A trapped hematoma strips that supply, leading to cartilage necrosis — a saddle-nose deformity in the septum, or cauliflower ear in the auricle. Prompt drainage prevents both.
What makes a neck laceration an emergency? Penetration of the platysma plus hard signs — expanding or pulsatile hematoma, active bleeding, bruit or thrill, airway compromise, or hematemesis. These warrant urgent surgical evaluation rather than bedside exploration.
References
- Sabatino F, Moskovitz JB. Facial wound management. Emerg Med Clin North Am. 2013;31(2):529-538.
- Tsao J, Hwang CE. Emergency Facial Injuries in Athletics. Clin Sports Med. 2023;42(3):463-471.
- Yamamoto R, Homma K, Masuzawa Y, et al. Early Complications Following Facial Laceration Repair Performed by Emergency Physicians After One Year of Wound Closure Training. AEM Educ Train. 2018;2(4):259-268.
- Mardani M, Arabion H. Surgical Management of Parotid Duct Injury Using a Feeding Tube. Ann Maxillofac Surg. 2020;10(2):472-474.
- Ibraheem K, Wong S, Smith A, et al. Computed tomography angiography in the “no-zone” approach era for penetrating neck trauma: A systematic review. J Trauma Acute Care Surg. 2020;89(6):1233-1238.
- Petrone P, Velaz-Pardo L, Gendy A, et al. Diagnosis, management and treatment of neck trauma. Cir Esp (Engl Ed). 2019;97(9):489-500.
Joonpyo Hong, MD is a board-certified otolaryngologist practicing in Korea. This article reflects his clinical interpretation of published research and does not constitute individual medical advice.
For more interesting contents:
https://curiousmd.com/when-to-fix-a-broken-nose/
https://curiousmd.com/deviated-septum-diagnosis-ai/
https://curiousmd.com/perilymphatic-fistula-from-weightlifting/
Link out to:
StatPearls — Facial Laceration Repair (NCBI Bookshelf):
https://www.ncbi.nlm.nih.gov/books/NBK570584/
StatPearls — Neck Trauma: zones and management (NCBI Bookshelf):
https://www.ncbi.nlm.nih.gov/books/NBK470422/
StatPearls — Nasal Fracture Reduction: septal hematoma drainage (NCBI Bookshelf):
https://www.ncbi.nlm.nih.gov/books/NBK538299/