
Tinnitus bimodal stimulation entered mainstream medicine in March 2023, when the FDA approved the first device of its kind. Around the same time, a growing body of evidence was confirming what audiologists had long suspected: cognitive behavioral therapy (CBT) works for tinnitus too — just not in the way most people think. Here is what both treatments actually do, and what the latest trials say about using them together.
What Is Tinnitus, and Why Is It So Hard to Treat?
Tinnitus is not a disease. It is a symptom — specifically, the brain’s response to a disrupted auditory signal. When the cochlea is damaged by noise, aging, or medication, it sends fewer signals to the brain. Rather than going quiet, the brain fills in the gap by generating its own activity. That self-generated noise is what patients hear as tinnitus.
This is why tinnitus is notoriously resistant to treatment: the sound does not come from the ear. Eardrops, antihistamines, and vasodilators target the wrong organ. Effective treatments need to address the brain itself — specifically, the hyperactive neural circuits that generate the phantom sound.
What Is Bimodal Stimulation? The Neuroscience, Explained Simply
The Brain Station Where the Problem Starts: the Dorsal Cochlear Nucleus
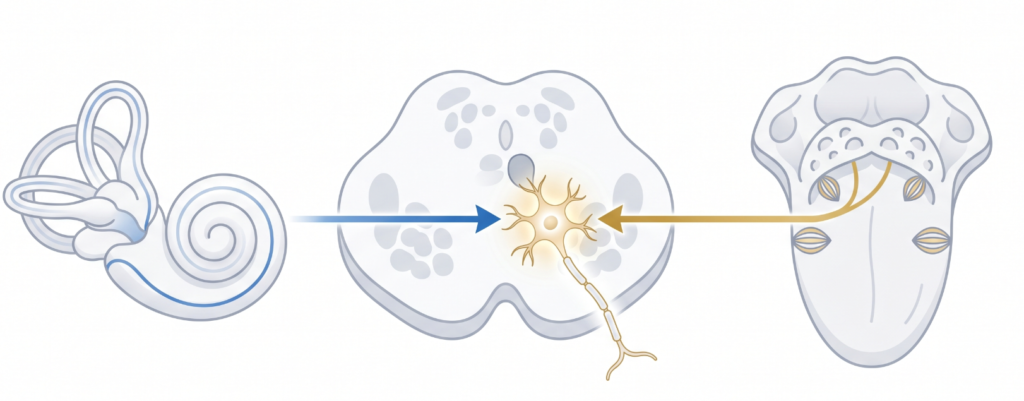
To understand why bimodal stimulation works, you need to know about one small but critical brain region: the dorsal cochlear nucleus (DCN). The DCN sits at the brainstem level and is the first place in the entire auditory pathway where sound signals from the ear and touch/movement signals from the body converge onto the same neurons — the so-called fusiform cells.
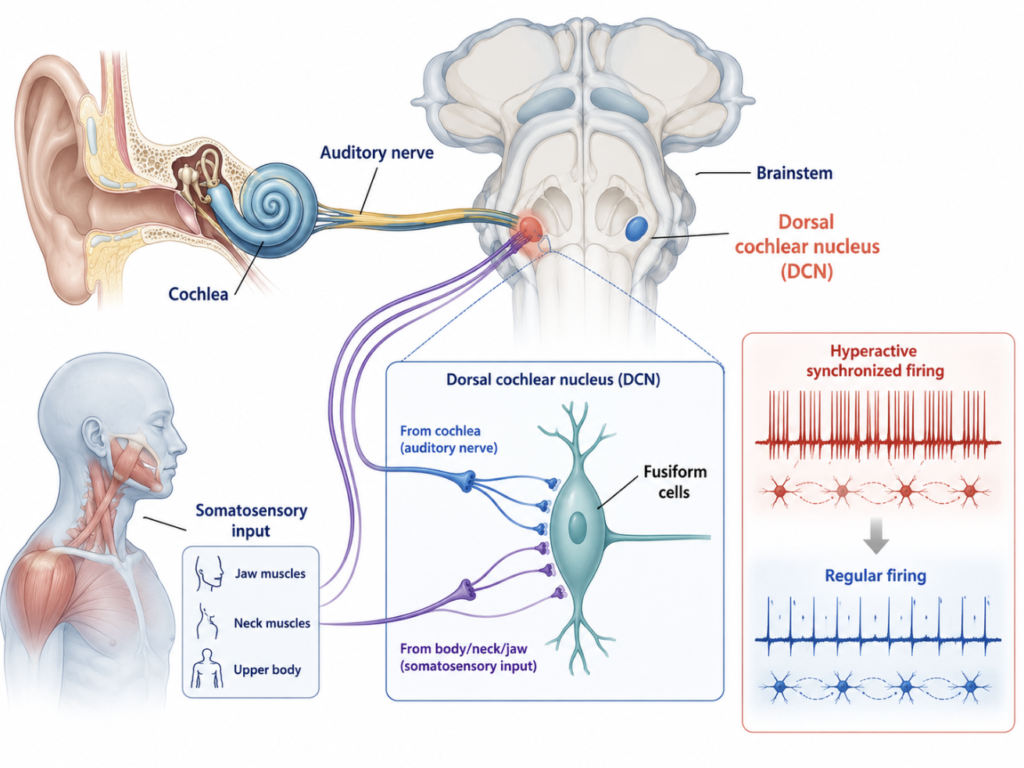
Under normal conditions, this convergence is well-regulated. But after hearing loss, the DCN fusiform cells become hyperactive and fire in an abnormally synchronized, rhythmic pattern. (Peripheral auditory system damage → Reduced auditory signal input → Decreased cortical inhibitory activity → Neural hyperactivity in auditory centers → Hyperactivity in the Dorsal Cochlear Nucleus.) Research in animal models of tinnitus has consistently shown that this synchronized hyperactivity in the DCN corresponds directly to tinnitus perception (Kaltenbach, Progress in Brain Research, 2007; Shore et al., Science Translational Medicine, 2018).
Think of it this way: imagine a choir that normally sings in harmony. After an injury, a section of the choir starts improvising wildly out of turn — loudly, constantly, and out of sync with the rest. That noise is tinnitus. The goal of treatment is to get those rogue singers back in line.
How Bimodal Stimulation Quiets the DCN
Here is the key insight: because the DCN fusiform cells receive both auditory and somatosensory inputs, you can use both to influence their activity. Bimodal stimulation does exactly this — it delivers a precisely timed pair of signals (sound + physical stimulation) to exploit a fundamental property of neurons called spike timing-dependent plasticity (STDP).
STDP is the brain’s rule for learning: neurons that fire together, wire together — and neurons that fire in the wrong order, wire apart. More precisely, when two signals arrive at a neuron in a specific sequence and timing window, the synapse is either strengthened (long-term potentiation, LTP) or weakened (long-term depression, LTD).
Bimodal stimulation uses the LTD direction deliberately. By presenting the tongue electrical pulse a few milliseconds before the sound stimulus — in the precise timing window that the DCN fusiform cells respond to — it induces long-term depression at the overactive synapses. Over weeks of repeated sessions, this quiets the hyperactive, hypersynchronized firing pattern. The rogue choir section is brought back to tempo.
A landmark study by Shore et al. (Science Translational Medicine, 2018) demonstrated this mechanism in both guinea pig tinnitus models and humans: 25 days of targeted bimodal stimulation significantly reduced both the physiological and behavioral evidence of tinnitus. The effect was timing-specific — the wrong interval between the two stimuli had no benefit.
The analogy that captures it: think of noise-canceling headphones. They do not turn off the external noise — they generate an anti-signal timed to cancel it. Bimodal stimulation does something similar at the neural level: it delivers an anti-pattern to the overactive circuit, reducing its gain from within.
The Lenire Device: FDA Approved, and How It Works in Practice
What Is Lenire?
Lenire (manufactured by Neuromod Devices, Ireland) is the leading tinnitus bimodal stimulation device on the market and the first to receive FDA clearance. It received FDA De Novo approval in March 2023, following a series of multi-site randomized controlled trials — most notably the TENT-A3 pivotal trial, which showed a 58.6% responder rate with bimodal treatment versus 43.2% with sound therapy alone (Boedts et al., Nature Communications, 2024).
Device Components
- Bluetooth headphones — play personalized sound sequences (not white noise, but specifically designed auditory patterns)
- Tonguetip® — a small, flat mouthpiece with an array of electrodes on its surface, placed on the tip of the tongue
- Handheld controller — allows the patient to start, pause, and adjust intensity
📷Device components (headphones, Tonguetip®, controller): View on Lenire.com — Source: Neuromod Devices
📷 Device in use (patient wearing Lenire during a session): View on Lenire.com — Source: Neuromod Devices
How to Use It: A Typical Session
The protocol is straightforward and designed for home use after an initial clinic setup:
- Place the Tonguetip in the mouth with the electrode array facing downward, resting against the tip of the tongue. The sensation is described as a mild, tingling buzz — similar to a 9-volt battery briefly touched to the tongue, but much gentler.
- Put on the headphones and connect via Bluetooth to the controller.
- Press Play and remain in a relaxed, seated position.
- Session duration: 30 minutes, twice daily (morning and evening, or back-to-back). Pausing more than once per session is discouraged to maintain stimulation continuity.
- Treatment course: 12 weeks. The Tonguetip is cleaned with liquid soap before each use.
The experience is non-invasive and generally well-tolerated. In the 2025 real-world study of 220 U.S. patients, no device-related serious adverse events were reported (McMahan and Lim, Communications Medicine, 2025).
Real-World Outcomes (2025–2026)
| Study | Journal | N | Responder Rate | Mean THI Improvement |
|---|---|---|---|---|
| McMahan & Lim (RWE) | Commun Med, 2025 | 220 | 91.5% | 27.8 points ↓ |
| AJA Clinical Practice Study | Am J Audiology, 2026 | — | 81.8% | Clinically significant |
| TENT-A3 Pivotal RCT | Nature Comm, 2024 | 112 | 58.6% | vs. 43.2% (sound only) |
The responder rates in real-world settings (81–91%) exceed those of the controlled trials (58%) — likely because real-world patients are self-selected and motivated, and clinic staff can optimize device fit and settings.
What Is CBT for Tinnitus? Not What Most Doctors Think
The Misconception
When doctors hear “cognitive behavioral therapy,” many picture a psychologist helping a patient talk through their feelings. For tinnitus, CBT is more specific than that — and more mechanical.
What Tinnitus CBT Actually Does
Tinnitus CBT does not try to eliminate the sound. It targets the brain’s alarm response to the sound. In people with bothersome tinnitus, the limbic system treats the tinnitus signal as a threat — triggering anxiety, hypervigilance, and sleep disruption that amplify the perceived loudness and distress, even when the actual signal has not changed.
CBT for tinnitus typically runs 6–12 weeks and includes:
- Psychoeducation — understanding why the brain amplifies tinnitus (reduces fear)
- Cognitive restructuring — identifying and challenging catastrophic thoughts (“this will never stop”)
- Behavioral activation — re-engaging with activities avoided because of tinnitus
- Attention training — systematic practice at redirecting focus away from the tinnitus signal
The result is not a quieter tinnitus — it is a less alarmed brain. Patients often report the tinnitus is “still there, but I don’t care about it as much.” That shift is measurable: CBT shows effect sizes of 0.44–0.70 on validated distress scales, with higher effects in patients who also have anxiety or depression (Bader et al., The Laryngoscope, 2025).
The AAO-HNS Clinical Practice Guideline lists CBT as a recommendation for patients with persistent, bothersome tinnitus — one of very few treatments to receive this designation.
Access Problem and the iCBT Alternative
In Korea and many other countries, tinnitus-specific CBT is scarce. Referral to psychiatry carries stigma, and most audiologists are not trained in CBT protocols. Internet-based CBT (iCBT) apps — such as Timibot, which uses a chatbot interface — are showing comparable efficacy to therapist-delivered CBT for mild-to-moderate tinnitus distress, with faster early improvement when combined with remote counseling.
Combining Both: What the 2025 UNITI Trial Tells Us
The most rigorous answer to “should I do both?” comes from the UNITI (Unification of Treatments and Interventions for Tinnitus Patients) trial, published in Nature Communications in 2025. This international, multicenter RCT randomized patients to 10 treatment arms — single therapies (CBT, hearing aids, counseling, sound therapy) and pairwise combinations of each.
The finding: combination treatments outperformed single treatments, but the benefit was additive, not synergistic. In other words, CBT + sound therapy was better than either alone, but the improvement was roughly the sum of two individual effects — not a multiplied bonus.
Clinical implication: if a patient can access both treatments, combining them is worthwhile. But expecting a dramatic “multiplier effect” is not supported by evidence. The priority should be determined by the patient’s dominant complaint: if distress and anxiety drive the suffering, start with CBT. If the tinnitus perception itself is the central problem in a patient with moderate-to-severe symptoms and no significant psychological comorbidity, bimodal stimulation is a logical first choice — where available.
Clinical Perspective In my experience, the patients who struggle most are those stuck waiting for a “cure.” Both bimodal stimulation and CBT share a counterintuitive premise: they do not silence the tinnitus, they change the relationship between the brain and the sound. Explaining this clearly at the first consultation changes patient expectations — and usually improves outcomes, regardless of which treatment follows.
Key Takeaways
- Tinnitus originates in the brain, not the ear — specifically in hyperactive, hypersynchronized neurons in the dorsal cochlear nucleus (DCN).
- Tinnitus bimodal stimulation (sound + tongue electrical stimulation) uses spike timing-dependent plasticity to induce long-term depression in overactive DCN circuits — quieting the neural source of tinnitus.
- Lenire, the first FDA-approved bimodal device (cleared March 2023), uses 30-minute twice-daily sessions for 12 weeks; real-world responder rates reach 81–91%.
- CBT for tinnitus does not silence the sound — it reduces the brain’s alarm response to it, with effect sizes of 0.44–0.70 and strong guideline endorsement.
- Combining bimodal stimulation and CBT improves outcomes more than either alone, but the effect is additive, not synergistic (UNITI RCT, Nature Communications, 2025).
- Lenire is not yet available globally; in most cases, domestic guidelines endorse CBT/TRT but have not reached consensus on neuromodulation.
FAQ
Is the Lenire device available in South Korea?
No — Lenire is not currently approved in South Korea. As of 2025, it is available by prescription in the United States, the European Union, and Australia. The Korean Tinnitus Study Group’s 2025 Delphi consensus did not reach agreement on neuromodulation treatments, meaning no domestic guideline or insurance pathway exists yet.
Does CBT require a psychiatrist?
Not necessarily. Tinnitus-specific CBT can be delivered by trained audiologists or through internet-based CBT (iCBT) platforms. Psychiatric referral is recommended when significant anxiety, depression, or sleep disorder accompanies the tinnitus, as these conditions need independent management and tend to amplify tinnitus distress.
What does tongue stimulation actually feel like?
Patients consistently describe the Tonguetip sensation as a mild tingling or buzzing — comparable to lightly touching a 9-volt battery to the tongue for a fraction of a second, but gentler and more diffuse. It is not painful. In the 2025 real-world study of 220 patients, no serious device-related adverse events were reported.
Can I do bimodal stimulation and CBT at the same time?
Yes, and the 2025 UNITI trial supports this approach. The combined benefit exceeds either treatment alone. There is no known interaction or contraindication between the two. The practical constraint is access: CBT availability is limited in many regions, and Lenire requires a clinic prescription and fitting.
References
- Kaltenbach JA. The dorsal cochlear nucleus as a contributor to tinnitus: mechanisms underlying the induction of hyperactivity. Prog Brain Res. 2007;166:89-106.
- Marks KL, Martel DT, Wu C, Basura GJ, Roberts LE, Schvartz-Leyzac KC, Shore SE. Auditory-somatosensory bimodal stimulation desynchronizes brain circuitry to reduce tinnitus in guinea pigs and humans. Sci Transl Med. 2018 Jan 3;10(422):eaal3175.
- Boedts M, et al. Combining sound with tongue stimulation for the treatment of tinnitus: a multi-site single-arm controlled pivotal trial. Nat Commun. 2024;15.
- McMahan EE, Lim HH. Retrospective chart review demonstrating effectiveness of bimodal neuromodulation for tinnitus treatment in a clinical setting. Commun Med (Lond). 2025;5:112.
- Kasper CA, May JM, Crossland NE, Lim HH. Bimodal neuromodulation for tinnitus in a clinical practice setting: clinically significant benefit for patients with moderate or worse symptoms. Am J Audiol. 2026.
- Schoisswohl S, Basso L, Simoes J, et al. Single versus combination treatment in tinnitus: an international, multicentre, parallel-arm, superiority, randomised controlled trial. Nat Commun. 2025;16:10510.
- Bader E, Dinces E, Moskowitz HS, Sturm JJ. Is cognitive behavioral therapy effective for tinnitus? Laryngoscope. 2025;135:2231-2232.
- Jeong J, Lee HY, Choo OS, Kim H, Lee KY, Song JJ, Seo JH, Rah YC, Song JJ, Nam EC, Park SN, Moon IS, Shim HJ. Consensus statements on tinnitus treatment: a Delphi study by the Korean Tinnitus Study Group. J Korean Med Sci. 2025;40(18):e75.
This article is for educational purposes only and does not substitute for medical advice.
For more interesting contents:
https://curiousmd.com/ai-chatbot-for-tinnitus/
https://curiousmd.com/tms-therapy-conditions-tinnitus/
Link out to:
https://www.accessdata.fda.gov/cdrh_docs/pdf21/DEN210033.pdf: FDA De Novo approval (DEN210033)
https://www.entnet.org/quality-practice/quality-products/clinical-practice-guidelines/tinnitus/: AAO-HNS Clinical Practice Guideline for tinnitus