
Nasopharyngeal carcinoma AI detection has entered a new era. A nasal endoscopy takes roughly three minutes. In that window, a 3mm lesion tucked into the posterior nasopharynx can look completely unremarkable — or it can be the early-stage cancer that, if missed, won’t be caught again until stage III. Two studies published in Lancet-family journals in 2025 now show that AI, running in real time during the endoscopy itself, can flag that lesion with sensitivity above 91%. Here’s what the research actually says — and what it means for the ENT clinic.
What Is Nasopharyngeal Carcinoma — and Why Is Early Detection So Hard?
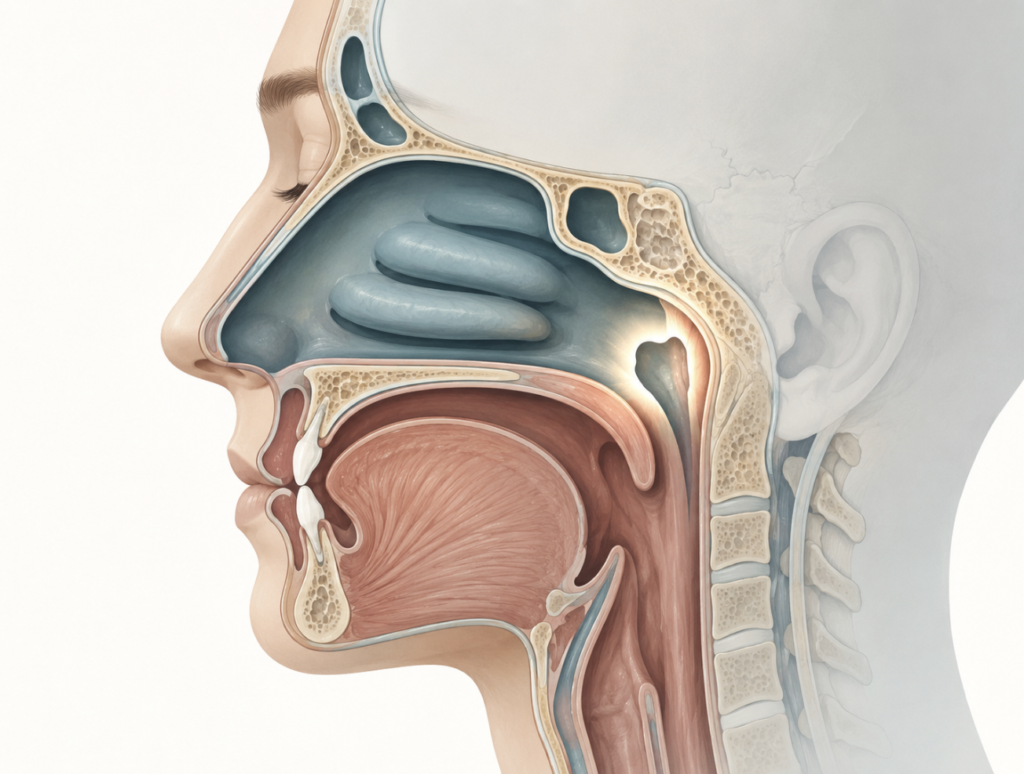
The nasopharynx sits at the very back of the nasal cavity, just above the soft palate — a space the patient cannot feel, cannot see, and cannot easily describe when something is wrong. Nasopharyngeal carcinoma (NPC) arises from the epithelial lining of this region, and it is one of the most geographically skewed cancers in oncology: incidence in southern China and Southeast Asia runs 15–25 times higher than in North America or Northern Europe. (Tang et al., Cancer Lett, 2016) In Korea, NPC accounts for a meaningful proportion of head and neck malignancies, a pattern seen across much of East Asia.
The clinical problem is that NPC is biologically aggressive but diagnostically subtle in its early stages. Early lesions can appear as slight mucosal irregularities, subtle color changes, or minimal submucosal fullness — findings that blend into normal nasopharyngeal anatomy, especially under standard white-light endoscopy. In most published series, NPC presents at advanced stage, when treatment becomes far more complex and prognosis worsens substantially. The gap between biology (cancer is present) and diagnosis (cancer is confirmed) is exactly where AI has the most to offer.
Nasopharyngeal Carcinoma AI Detection: How It Works
Every modern nasal endoscope generates a continuous video feed. Deep learning models, trained on tens of thousands of labeled endoscopic frames, can analyze that feed frame-by-frame and output a real-time probability score — or a colored overlay — indicating whether a region of interest looks malignant, benign, or normal.
Two imaging modalities are particularly relevant here. White-light imaging (WLI) is the standard view most ENTs use day-to-day. Narrow-band imaging (NBI) uses specific wavelengths of light to enhance mucosal vascular patterns, making subtle surface irregularities more visible to both human and machine. The best-performing AI systems now integrate both modalities simultaneously — not just processing one frame at a time, but correlating visual signals across multiple wavelengths to produce a more reliable output.

The output itself can take two forms: detection (is there something suspicious here?) and segmentation (exactly where are the tumor margins?). This distinction matters clinically, as we’ll see below.
The 2025 Studies: What They Actually Found
Study 1 — STND System (Lancet Digital Health, 2025)
A team across eight major NPC centers in China developed the Swin Transformer-based Nasopharyngeal Diagnostic (STND) system, training it on 27,362 labeled endoscopic images. The model was then externally validated on 1,885 prospectively acquired images from ten separate hospitals — a robust design that matters precisely because AI systems frequently underperform when moved from their training environment to a new clinical site.
The results held up. In external validation, STND achieved an area under the curve (AUC) of 0.95 for NPC detection, with sensitivity of 91.6% and specificity of 86.1%. Critically, the study also measured what happened when primary care ENT specialists used STND as a real-time assistant: their diagnostic accuracy improved from 83.4% to 91.2% — a 7.9 percentage-point gain from one software overlay. That number is the one that should get ENTs’ attention. (Shi et al., Lancet Digital Health, 2025)
Study 2 — NPC-SDNet (eClinicalMedicine, 2025)
A separate multicenter prospective study — published in eClinicalMedicine, another Lancet-family journal — took the AI challenge one step further. The Nasopharyngeal Carcinoma Segmentation Diagnostic Network (NPC-SDNet) was trained and validated on endoscopic video data from 707 patients across multiple centers, using both WLI and NBI simultaneously.
NPC-SDNet is the first validated AI system designed to perform real-time tumor segmentation alongside detection. Rather than just alerting the endoscopist to a suspicious region, it draws a pixel-level boundary around the lesion — in real time, on the live video feed. Using WLI, the system achieved diagnostic accuracy of 95.0%, sensitivity of 97.2%, and specificity of 93.5%. The clinical value extends beyond detection: tumor margin delineation prior to biopsy planning changes how and where you sample tissue, with downstream implications for surgical planning. (He et al., eClinicalMedicine, 2025)
Nose-Keeper: AI in Your Pocket (npj Digital Medicine, 2024)
The third piece of the 2024–2025 research cluster is different in character. Rather than a hospital-integrated deep learning system, Nose-Keeper is a smartphone application developed across three high-incidence NPC centers and trained on 39,340 nasal endoscopic white-light images. Its target user isn’t the subspecialty ENT — it’s the primary care physician or non-specialist otolaryngologist in a region where NPC is common but subspecialty access is limited.
The performance data are striking. Nose-Keeper achieved an overall diagnostic accuracy of 92.27% (95% CI: 90.66–93.61%), with NPC-specific sensitivity of 96.39% and specificity of 99.91%. In a direct comparison, the app outperformed nine experienced otolaryngologists on the same image set. The study also used explainable AI (XAI) to highlight the lesion areas driving the model’s decision — an important feature for clinical trust and safety. (Yue et al., npj Digital Medicine, 2024)
AI vs. Human ENT: Putting the Numbers in Context
| System | Journal (Year) | Sensitivity | Specificity | Impact on Clinicians |
|---|---|---|---|---|
| STND | Lancet Digital Health (2025) | 91.6% | 86.1% | +7.9% accuracy boost for primary ENTs |
| NPC-SDNet | eClinicalMedicine (2025) | 97.2% (WLI) | 93.5% (WLI) | First real-time tumor margin segmentation |
| Nose-Keeper | npj Digital Medicine (2024) | 96.39% | 99.91% | Outperformed 9 experienced ENT specialists |
One honest note on that table: these studies used different patient populations, imaging protocols, and reference standards. Direct cross-study comparison of raw accuracy numbers is statistically inappropriate — the numbers should be read within each study’s context, not ranked against each other. What the table does illustrate is that AI systems across multiple independent research groups are consistently reaching the range of high-performing specialist-level detection.
Clinical Perspective: What This Means in Practice
The following reflects my clinical opinion based on these studies and my experience performing nasal endoscopy in a Korean ENT setting.
Reading this research as someone who performs nasal endoscopy regularly, few findings deserve particular attention.
The +7.9% boost for primary care ENTs is the real story. Expert endoscopists at tertiary centers are already good at spotting NPC. The gap that matters is in the primary care setting — the general ENT clinic where most patients present first, where throughput is high, and where a subtle early lesion may not trigger an immediate biopsy reflex. That’s exactly where STND showed its value. If an AI overlay can consistently nudge diagnostic accuracy from 83% to 91% in community ENT practice, the downstream impact on stage-at-diagnosis could be significant.
AI does not eliminate the biopsy decision — it sharpens it. Every lesion flagged by AI still requires tissue confirmation. NPC diagnosis is histopathological, full stop. What AI changes is which lesions get biopsied and how confidently the clinician proceeds. A high-confidence AI flag on a subtle mucosal irregularity that might otherwise be watched and re-scoped in three months becomes a prompt for same-visit biopsy. That time compression, for an aggressive cancer, matters.
The geographic context is critical. In North America or Northern Europe, NPC is rare enough that routine AI screening during nasal endoscopy may not be cost-effective. In Korea, southern China, and Southeast Asia, the calculus is different. With incidence rates 15–25× higher, the probability that any given suspicious lesion is NPC is meaningfully elevated — which directly improves the positive predictive value of an AI flag. These tools were developed and validated in high-incidence populations, and that’s where they will first demonstrate real-world clinical value.
The smartphone approach (Nose-Keeper) addresses a different problem. Hospital-integrated AI systems require infrastructure, IT integration, and regulatory clearance before they reach a clinic’s endoscopy suite. Nose-Keeper’s smartphone model is designed for the gap between that future state and today’s reality — the regional hospital or primary care clinic that has an endoscope but no AI integration, serving a population with elevated NPC risk. Accuracy that outperforms specialists on a smartphone, in that context, is clinically meaningful.
What’s not yet solved: real-world workflow integration, cost, regulatory pathway (CE marking, FDA clearance, Korean MFDS approval), and clinician training. None of the studies I’m describing are clinical deployment trials. They are validation studies — strong ones, but validation nonetheless. The path from “validated in a multicenter prospective study” to “running in my endoscopy suite on Tuesday” involves procurement, IT, training, and ongoing quality monitoring. That gap is real and worth naming.

Key Takeaways
- AI systems can now detect nasopharyngeal carcinoma in real time during nasal endoscopy, with the STND system (Lancet Digital Health, 2025) achieving 91.6% sensitivity and 86.1% specificity across ten external validation hospitals.
- AI assistance improved primary care ENT diagnostic accuracy by 7.9 percentage points in the STND study — from 83.4% to 91.2% — suggesting the greatest benefit is in non-subspecialty settings.
- The NPC-SDNet system (eClinicalMedicine, 2025) is the first AI to perform real-time pixel-level tumor segmentation during nasal endoscopy, adding margin delineation to the detection capability.
- The Nose-Keeper smartphone app (npj Digital Medicine, 2024) achieved 92.27% overall accuracy and 96.39% NPC sensitivity, outperforming nine experienced otolaryngologists on the same image set.
- These AI tools are most clinically relevant in East and Southeast Asia, where NPC incidence is 15–25× higher than in Western populations — a geographic advantage that directly improves positive predictive value.
FAQ
Can AI detect nasopharyngeal carcinoma in real time during a nasal endoscopy? Yes. The NPC-SDNet system, published in eClinicalMedicine (2025), demonstrated real-time AI detection and pixel-level tumor segmentation during nasal endoscopy using both white-light and narrow-band imaging, validated prospectively across multiple centers in 707 patients. The STND system (Lancet Digital Health, 2025) achieved AUC 0.95 with 91.6% sensitivity in external validation across ten hospitals.
How accurate is AI compared to a doctor in detecting NPC? In the STND study (Lancet Digital Health, 2025), AI achieved 91.6% sensitivity and 86.1% specificity. ENT specialists using AI assistance improved from 83.4% to 91.2% accuracy. The Nose-Keeper app (npj Digital Medicine, 2024) outperformed nine experienced otolaryngologists with 96.39% NPC sensitivity and 99.91% specificity. These figures come from controlled research settings using curated image sets, however — real-world clinical performance may differ, and all numbers warrant cautious interpretation at this stage of validation.
What is the Nose-Keeper app for nasopharyngeal cancer? Nose-Keeper is a smartphone-based deep learning application trained on 39,340 nasal endoscopic images from three high-incidence NPC centers. It classifies nasal endoscopy images as NPC, benign nasal disease, or normal — achieving 92.27% overall accuracy. It is designed for primary care settings in high-incidence regions where subspecialty access is limited.
Does AI replace the ENT specialist in NPC diagnosis? No. All validated AI systems function as real-time decision support, not autonomous diagnostics. The ENT specialist still performs the endoscopy, interprets AI output in clinical context, and makes the biopsy decision. NPC diagnosis is ultimately histopathological — tissue confirmation is always required.
Who is most at risk for nasopharyngeal carcinoma? NPC risk is substantially higher in East and Southeast Asia — particularly southern China, Korea, Vietnam, Malaysia, and the Philippines — where incidence is 15–25 times higher than in North America or Europe. Additional risk factors include Epstein-Barr virus (EBV) infection, family history of NPC, and consumption of salt-preserved foods.
Joonpyo Hong, MD is a board-certified otolaryngologist practicing in Korea. This article reflects his clinical interpretation of published research and does not constitute individual medical advice.
References
- Shi Y, et al. Artificial intelligence-assisted detection of nasopharyngeal carcinoma on endoscopic images: a national, multicentre, model development and validation study. Lancet Digit Health. 2025. PMID: 40544083
- He R, et al. Real-time artificial intelligence-assisted detection and segmentation of nasopharyngeal carcinoma using multimodal endoscopic data: a multi-center, prospective study. eClinicalMedicine. 2025.
- Yue Y, Zeng X, Lin H, et al. A deep learning based smartphone application for early detection of nasopharyngeal carcinoma using endoscopic images. npj Digit Med. 2024;7(1):384.
- Tang LL, Chen WQ, Xue WQ, et al. Global trends in incidence and mortality of nasopharyngeal carcinoma. Cancer Lett. 2016;374(1):22-30.
For more interesting contents:
https://curiousmd.com/deviated-septum-diagnosis-ai/
https://curiousmd.com/role-of-smell-in-flavor/
You can link out to:
https://www.thelancet.com/journals/landig/article/PIIS2589-7500(25)00041-X/fulltext
https://www.thelancet.com/journals/eclinm/article/PIIS2589-5370(25)00052-5/fulltext