
This article compares the current EPOS vs AAO-HNS guidelines on the management of chronic rhinosinusitis.
Two patients walk into the same clinic on the same morning. Both have had nasal blockage, post-nasal drip, and a dulled sense of smell for fourteen weeks. Whether one of them leaves with a steroid spray, the other with a biologic injection schedule, or either ends up in an operating room depends in part on which guideline their surgeon reads most carefully. This article maps where the European Position Paper on Rhinosinusitis and Nasal Polyps (EPOS) 2020 and the brand-new 2025 American Academy of Otolaryngology–Head and Neck Surgery (AAO-HNS) Surgical Management Clinical Practice Guideline actually disagree — and where the modern thinking on phenotype, endotype, and biologics fits between them.

What Each Guideline Actually Says: EPOS vs AAO-HNS
EPOS 2020 — the European framework
EPOS 2020 defines chronic rhinosinusitis (CRS) as two or more cardinal symptoms — nasal obstruction, anterior or posterior nasal discharge, facial pain or pressure, reduction or loss of smell — lasting twelve weeks or longer, with objective confirmation by either nasal endoscopy or computed tomography (CT) [Fokkens, European Position Paper on Rhinosinusitis and Nasal Polyps 2020, 2020]. Its most influential contribution is structural: it separates primary CRS from secondary CRS, then layers in anatomic distribution (localized vs diffuse), endotype dominance (type 2 vs non-type 2), and phenotype examples. EPOS is also explicit about biomarker thresholds for the type 2 endotype: tissue eosinophils ≥10 per high-power field, blood eosinophils ≥250 cells/µL, and total IgE ≥100 IU/mL [Fokkens, European Position Paper on Rhinosinusitis and Nasal Polyps 2020, 2020].
AAO-HNS — 2015 Adult Sinusitis plus 2025 Surgical CPG
The American framework currently sits in two documents. The 2015 Adult Sinusitis CPG anchors the diagnosis: at least two of four cardinal symptoms for twelve weeks, plus objective evidence of inflammation by anterior rhinoscopy, nasal endoscopy, or CT [Rosenfeld, Clinical Practice Guideline (Update): Adult Sinusitis, 2015]. The 2025 Surgical Management CPG, published on May 27, 2025, layers on eleven key action statements specifically for the surgical pathway. It tells surgeons to verify the CRS diagnosis before offering surgery, to obtain a fine-cut CT for planning, and — notably — to not endorse a one-size-fits-all duration of preoperative medical therapy as a prerequisite [Shin, Clinical Practice Guideline: Surgical Management of Chronic Rhinosinusitis, 2025].
Side-by-Side: Where They Disagree
The differences look small on paper and matter a lot at the bedside.
| Domain | EPOS 2020 | AAO-HNS (2015 + 2025) |
|---|---|---|
| Objective confirmation | Endoscopy or CT | Rhinoscopy, endoscopy, or CT |
| Primary classification axis | Endotype-led (type 2 vs non-type 2) | Phenotype-led (CRSwNP vs CRSsNP) |
| Biomarker thresholds | Defined (eos, IgE cutoffs) | Not formally specified |
| Preoperative medical therapy | Structured step-up ladder | No mandated regimen (2025) |
| Biologics positioning | Integrated into the treatment ladder | Acknowledged; surgical vs biologic decision left to clinician |
| Recommendation grading | GRADE methodology | AAO-HNS Aggregate Grade of Evidence (strong / recommendation / option) |
Two practical consequences follow. First, an EPOS-oriented clinician is likelier to send blood eosinophils and total IgE early, because those numbers feed directly into the endotype decision. Second, an AAO-HNS 2025–oriented surgeon is more willing to skip a prolonged “trial of medical therapy” before operating on a patient whose disease is clearly severe — a meaningful change from prior practice [Shin, Clinical Practice Guideline: Surgical Management of Chronic Rhinosinusitis, 2025].
Phenotype vs Endotype: What You See vs What You Test
The older way of organizing CRS was phenotypic: polyps or no polyps, unilateral or bilateral, presence or absence of asthma. That language survives because it maps onto what an endoscope shows. A clinician can see bilateral polyps filling the middle meatus, identify allergic mucin suggestive of allergic fungal rhinosinusitis (AFRS), or note isolated maxillary opacification on imaging — all phenotypic observations made without a single lab test.
The endotype is the immune mechanism underneath. Tomassen and colleagues showed, using cluster analysis of mucosal biomarkers, that CRS partitions into inflammatory endotypes that cross phenotype lines — type 2 patients can have polyps or not, and non-polyp patients can carry a strong type 2 signature [Tomassen, Inflammatory Endotypes of Chronic Rhinosinusitis Based on Cluster Analysis of Biomarkers, 2016]. Determining the endotype requires labs and, in many cases, tissue: blood eosinophils, total IgE, and eosinophils per high-power field on biopsy.
Why this shift matters historically. Through the 1990s and 2000s, treatment selection was almost entirely phenotypic, and clinicians often saw “identical-looking” polyp patients respond very differently to the same treatment [Grayson, Contemporary Classification of Chronic Rhinosinusitis Beyond Polyps vs No Polyps: A Review, 2020]. The arrival of cytokine-targeting biologics changed the stakes: you cannot choose between an anti–IL-4Rα drug, an anti–IL-5 drug, and an anti-IgE drug from endoscopy alone. The endotype framework is not the only route to treatment, but it becomes particularly valuable when selecting among biologics or when the expected response is uncertain.
Clinical Perspective. An experienced rhinologist may infer a probable type 2 endotype from phenotype clues such as bilateral polyps, smell loss, comorbid asthma, and aspirin sensitivity, but laboratory or tissue data are often needed when treatment choice depends on biologic eligibility [Stevens, Associations Between Inflammatory Endotypes and Clinical Presentations in Chronic Rhinosinusitis, 2019]. That clinical inference is useful but not sufficient when the next step is a high-cost biologic with strict reimbursement criteria. The blood draw and, when feasible, the biopsy earn their place at that decision point.
The Rise of Biologics
Biologics are monoclonal antibodies that neutralize specific cytokines or their receptors. In CRS with nasal polyps (CRSwNP), biologics such as dupilumab, omalizumab, and mepolizumab have become established add-on options in patients with severe, uncontrolled disease [Fokkens, EUFOREA Consensus on Biologics for CRSwNP with or without Asthma, 2019]:
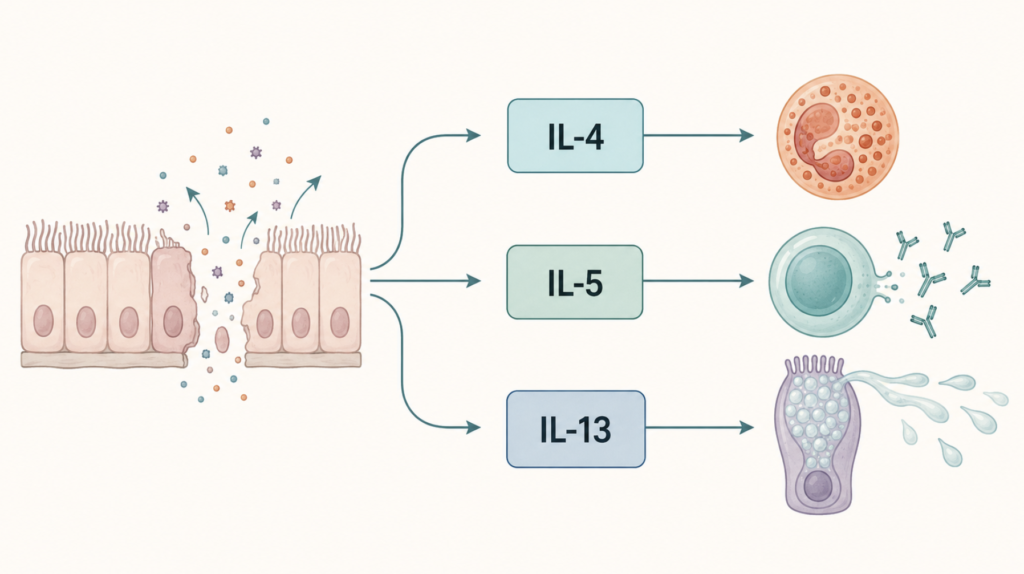
- Dupilumab binds the IL-4 receptor alpha subunit, blocking both IL-4 and IL-13 signaling.
- Omalizumab neutralizes free IgE; its dose is calculated from serum IgE and body weight.
- Mepolizumab binds IL-5 and depletes eosinophils.
Network meta-analyses comparing the three in CRSwNP consistently place dupilumab first for nasal polyp score reduction and improvement in nasal congestion, with omalizumab second [Wu, Which Is the Best Biologic for Nasal Polyps: Dupilumab, Omalizumab, or Mepolizumab? A Network Meta-Analysis, 2022]. Candidacy converges across guidelines: bilateral polyps, evidence of type 2 inflammation, comorbid asthma, prior surgery or surgical ineligibility, and persistent symptoms despite topical corticosteroids and saline irrigation.
The harder question — left largely unanswered by both EPOS and AAO-HNS — is when a biologic should precede revision surgery rather than follow it. Clinical practice appears to be drifting earlier on this axis, particularly in European centers where dupilumab was approved for CRSwNP in late 2019, but the threshold for “biologic before second surgery” remains a judgment call rather than a guideline recommendation.
Key Takeaways
- EPOS 2020 organizes CRS around endotype and biomarker thresholds; AAO-HNS organizes it around phenotype and surgical decision-making.
- Both require ≥12 weeks of symptoms plus objective confirmation, but AAO-HNS accepts anterior rhinoscopy in addition to endoscopy and CT.
- Phenotype is what an endoscope shows; endotype is what blood eosinophils, IgE, and tissue biopsy reveal about the immune driver.
- Three biologics — dupilumab, omalizumab, and mepolizumab — are approved for CRSwNP, with dupilumab leading head-to-head network meta-analyses.
- The 2025 AAO-HNS Surgical CPG removed the requirement for a predefined duration of medical therapy before sinus surgery.
FAQ
Which guideline should I follow if I practice in Asia? In East Asia, EPOS framing is commonly used for endotype discussion, while Japanese practice additionally relies on the JESREC scoring system for classifying eosinophilic CRS [Tokunaga, Novel Scoring System and Algorithm for Classifying Chronic Rhinosinusitis: The JESREC Study, 2015]. Korean practice tends to follow international guidelines without a country-specific scoring routine, often citing EPOS for endotype framing and AAO-HNS for surgical decisions.
Do I need a biopsy before starting a biologic? Usually not. Blood eosinophil count, total IgE, and a careful clinical history (bilateral polyps, asthma, smell loss) are enough to establish candidacy for the approved biologics in most regulatory and insurance contexts. Biopsy becomes valuable when the diagnosis is unclear or non–type 2 disease is suspected.
What changed in the 2025 AAO-HNS guideline that matters most? The most consequential shift is the explicit rejection of a one-size-fits-all preoperative medical therapy regimen. The guideline asks surgeons to base the decision to operate on symptoms, disease characteristics, quality of life, and prior therapy — not on a fixed checklist of trialed medications [Shin, Clinical Practice Guideline: Surgical Management of Chronic Rhinosinusitis, 2025].
References
- Fokkens WJ, Lund VJ, Hopkins C, et al. European Position Paper on Rhinosinusitis and Nasal Polyps 2020. Rhinology. 2020;58(Suppl S29):1-464.
- Shin JJ, Schwartz SR, Gudis DA, et al. Clinical Practice Guideline: Surgical Management of Chronic Rhinosinusitis. Otolaryngol Head Neck Surg. 2025;172(6):1213-1265.
- Rosenfeld RM, Piccirillo JF, Chandrasekhar SS, et al. Clinical practice guideline (update): adult sinusitis. Otolaryngol Head Neck Surg. 2015;152(2 Suppl):S1-S39.
- Tomassen P, Vandeplas G, Van Zele T, et al. Inflammatory endotypes of chronic rhinosinusitis based on cluster analysis of biomarkers. J Allergy Clin Immunol. 2016;137(5):1449-1456.
- Grayson JW, Hopkins C, Mori E, Senior B, Harvey RJ. Contemporary classification of chronic rhinosinusitis beyond polyps vs no polyps: a review. JAMA Otolaryngol Head Neck Surg. 2020;146(9):831-838.
- Stevens WW, Peters AT, Tan BK, et al. Associations between inflammatory endotypes and clinical presentations in chronic rhinosinusitis. J Allergy Clin Immunol Pract. 2019;7(8):2812-2820.e3.
- Fokkens WJ, Lund V, Bachert C, et al. EUFOREA consensus on biologics for CRSwNP with or without asthma. Allergy. 2019;74(12):2312-2319.
- Wu Q, Zhang Y, Kong W, Wang X, Yuan L, Zheng R, et al. Which is the best biologic for nasal polyps: dupilumab, omalizumab, or mepolizumab? A network meta-analysis. Int Arch Allergy Immunol. 2022;183(3):279-288.
- Tokunaga T, Sakashita M, Haruna T, et al. Novel scoring system and algorithm for classifying chronic rhinosinusitis: the JESREC Study. Allergy. 2015;70(8):995-1003.
Joonpyo Hong, MD is a board-certified otolaryngologist practicing in Korea. This article reflects his clinical interpretation of published research and does not constitute individual medical advice.
For more interesting contents:
https://curiousmd.com/anti-tslp-antibody-nasal-polyps/
https://curiousmd.com/smell-loss-parkinsons-alzheimers-ai-biomarker/
https://curiousmd.com/olfaction-memory-brain-neurodegenerative-disease/
Link out to:
European Position Paper on Rhinosinusitis and Nasal Polyps 2020:
https://doi.org/10.4193/Rhin20.600
AAO-HNS Surgical Management of Chronic Rhinosinusitis guideline:
https://www.entnet.org/quality-practice/quality-products/clinical-practice-guidelines/cpg-surgical-management-of-chronic-rhinosinusitis/
cluster analysis of inflammatory endotypes (Tomassen et al., 2016):
https://pubmed.ncbi.nlm.nih.gov/26949058/