
In October 2025, the U.S. Food and Drug Administration approved tezepelumab, an antibody that blocks a single epithelial signal called TSLP, for chronic rhinosinusitis with nasal polyps. The same molecule was already a severe-asthma drug. One target, two diseases, two separate approvals years apart. That sequence is the quiet story behind a louder one.
The louder story is about artificial intelligence. A Boston-area company, Generate: Biomedicines, has designed its own anti-TSLP antibody, GB-0895, using machine-learning models rather than conventional antibody engineering, and has moved it into global Phase 3 trials. Those trials are for severe asthma. Nasal polyps are not yet on the list. The obvious question for anyone who treats the upper airway is whether an AI-built antibody aimed at the same target will eventually make the same journey from the lungs to the nose.
The honest answer is that the path is plausible but unfinished. The mechanism connects the two diseases, a real drug has already walked the route, and the molecule is engineered for the kind of durability patients want. None of that is the same as proof. The hurdles ahead are specific and surmountable rather than fatal, which is exactly why the topic is worth taking seriously rather than hyping.
What TSLP Actually Does
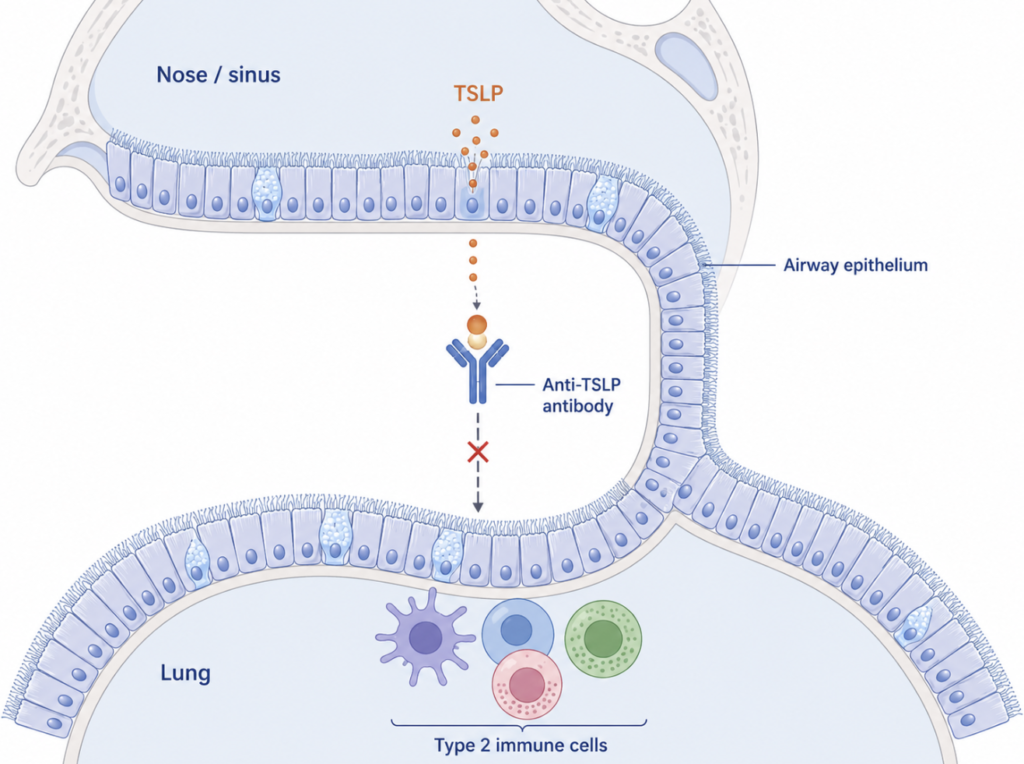
Thymic stromal lymphopoietin, abbreviated TSLP, is a cytokine released by the epithelial cells that line the airway. It is not a downstream foot soldier of inflammation. It sits near the top of the cascade, switching on the immune responses that follow when the airway lining meets allergens, viruses, or airborne irritants. Blocking TSLP, in principle, turns off a master switch rather than mopping up one of its many products.
This upstream position is what makes the target attractive across several diseases at once. TSLP drives the type 2 inflammation familiar from allergy, but it also influences responses that fall outside that classic pattern. A drug that neutralizes it is therefore not narrowly tied to a single inflammatory subtype, which has been one of tezepelumab’s defining features in asthma.
A switch at the top of a cascade is a tempting target. It is also only a target. The existence of an upstream signal says nothing, on its own, about whether silencing it relieves a given disease.
One Airway, Two Doors
The nose and the lungs are often treated as separate territories, divided between otolaryngology and pulmonology. The biology is less tidy. Severe asthma and chronic rhinosinusitis with nasal polyps share enough of their underlying inflammation that researchers describe them together as united airway disease, a single inflamed surface with an upper door and a lower door [De Corso, TSLP in epithelial-driven diseases, 2024].
TSLP is part of what links them. Its levels are elevated in nasal-polyp tissue compared with healthy sinus lining or with chronic rhinosinusitis that lacks polyps, and the epithelial cells of polyps have been shown to ramp up TSLP production under inflammatory signaling [Wang, OSM synergizes with IL-4 to induce TSLP, 2023]. The cytokine that misbehaves in a severe asthmatic’s lungs is measurably overactive in the polyps growing in another patient’s sinuses.
That shared biology is the strongest argument for cross-over. It is also where discipline matters most. A pathway being present and overactive in polyp tissue explains why blocking it might help. It does not establish that blocking it does help. The two statements live one clinical trial apart.
Clinical Perspective. The united-airway framing is genuinely useful at the bedside, because a patient with refractory polyps and poorly controlled asthma is often fighting one disease through two openings. But the clinician’s job is to resist the temptation to treat a convincing mechanism as a finished verdict. Shared inflammation predicts where to look next; it does not tell you what will be found.
How Tezepelumab Crossed Over
Tezepelumab is the proof that the route exists, and the detail of how it earned its second approval is the most instructive part of the whole story.
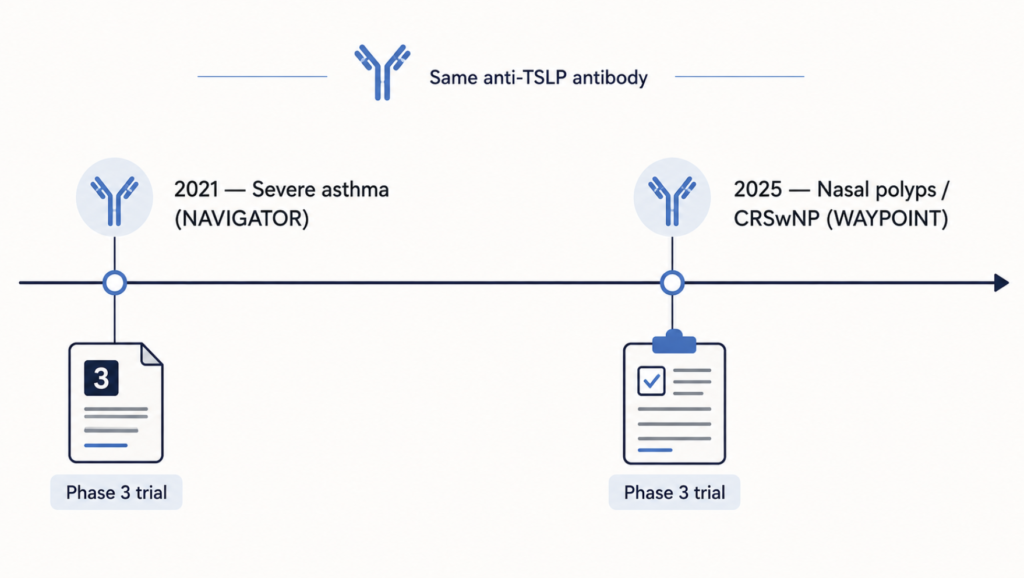
Its first home was severe asthma. In the Phase 3 NAVIGATOR trial, tezepelumab cut the annual rate of asthma attacks by more than half against placebo and improved lung function and symptom control, which carried it to approval as the first anti-TSLP drug [Menzies-Gow, Tezepelumab in severe asthma, 2021]. Many of those asthma patients also had nasal polyps, and their sinus symptoms tended to improve too. It would have been easy to treat that as good enough.
It was not treated as good enough. The efficacy of tezepelumab in nasal polyps as a stand-alone disease was formally unknown until it was tested directly, in the dedicated Phase 3 WAYPOINT trial. There the result was unambiguous: tezepelumab shrank nasal polyps and eased congestion, and the effect on hard outcomes was striking. Surgery for polyps was indicated in fewer than 1 in 200 treated patients, against roughly 1 in 5 on placebo, and systemic steroid use fell sharply as well [Lipworth, Tezepelumab in CRSwNP, 2025]. The October 2025 approval followed.
The lesson is not that the drug works in both diseases, true as that is. The lesson is the gap between the two approvals. A molecule that already worked in asthma, that already seemed to help the polyps of asthmatic patients, still had to prove itself in nasal polyps through its own trial before it could be used for them. Mechanism opened the door. A separate study was the key.
Clinical Perspective. For the upper-airway specialist, WAYPOINT is reassuring on two counts: it confirms that TSLP blockade meaningfully changes the natural history of polyps, including the need for surgery, and it models the evidentiary standard any successor will be held to. A drug does not inherit a sinus indication from its lung data. It buys one with a trial.
What Makes GB-0895 Different
Against that backdrop, GB-0895 is interesting less because it is new than because of how it was made and how it is meant to be used.
According to the company, GB-0895 is a monoclonal antibody designed with machine-learning models to bind TSLP with very high affinity and an extended half-life, with the explicit goal of dosing roughly twice a year rather than every few weeks (Generate:Biomedicines, 2025). The current approved anti-TSLP option is given by subcutaneous injection every four weeks; an antibody aimed at two injections annually would change the rhythm of treatment, if the durability holds up in late-stage testing. That “if” is doing real work. The dosing target rests on early pharmacokinetic data and a design intention, not on completed Phase 3 results.
The development program is where expectations need their firmest anchor. GB-0895 is in two global Phase 3 asthma trials and an earlier-stage study in chronic obstructive pulmonary disease (Generate:Biomedicines, 2025). There is, at present, no nasal-polyp trial. Early reports from the company also describe reductions in inflammatory markers in a Phase 1 study, but those are preliminary, early-phase findings that have not yet been peer-reviewed and published, and they should be read as a hint of direction rather than evidence of clinical benefit.
The “AI-designed” label deserves the same precision. Machine learning here is a tool for discovering and optimizing the molecule — tuning how tightly it grips its target and how long it lasts in the body. That is a discovery and engineering advantage. It is not a clinical one. An antibody designed by an algorithm and an antibody designed at a bench are judged by the same trials and the same outcomes. The software shapes the candidate; it does not lower the bar the candidate must clear.
| Tezepelumab | GB-0895 | |
|---|---|---|
| Target | TSLP | TSLP |
| Design approach | Conventional antibody engineering | AI / machine-learning design (per company) |
| Dosing | Every 4 weeks (subcutaneous) | ~Twice yearly goal, based on early data |
| Asthma | Approved (Phase 3, NAVIGATOR) | In Phase 3 |
| Nasal polyps (CRSwNP) | Approved (Phase 3, WAYPOINT) | No trial yet |
| COPD | — | Phase 1 |
| Evidence status | Peer-reviewed, regulator-reviewed | Company-reported; pivotal data pending |
The table makes the asymmetry plain. On the target, the two molecules are twins. On evidence, they are a generation apart.
Clinical Perspective. The design story is the part most likely to be oversold and the part that matters least to a patient. What a person with polyps will eventually care about is whether the polyps shrink, whether surgery is avoided, and how often the injection is needed. Affinity figures and design pedigree are interesting; outcomes are decisive.
Can It Reach the Nose?
So can an AI-designed anti-TSLP antibody extend from asthma to nasal polyps? The pieces line up in its favor, and the missing piece is nameable.
In its favor: the target is the same one that works in polyps, the biology connecting asthma and CRSwNP is well described, and a predecessor has already completed the exact crossover in question. A company that has reached Phase 3 against TSLP has both the rationale and the resources to open a polyp program if its asthma data hold. None of that is wishful. It is the ordinary logic of how a successful airway antibody expands its reach.
What is missing is the one thing that converted tezepelumab from promising to approved in the nose: a dedicated trial with polyp outcomes. Until GB-0895 is tested in CRSwNP directly, its case for the upper airway is an inference built on a strong mechanism and a good precedent, not a result. That is a reason for measured optimism rather than doubt — the gap is the normal distance between a sound hypothesis and a proven therapy, and it is a distance the field knows how to close.
Clinical Perspective. The realistic expectation is not whether such a drug could help nasal polyps, but when and whether a company will commit to finding out, and what its durability advantage would be worth in a disease defined by relapse and repeat surgery. A twice-yearly anti-TSLP option for refractory polyps would be a meaningful addition to the upper-airway toolkit. The mechanism has earned that hypothesis a fair test. The next move belongs to the trial, not the press release.
Key Takeaways
- TSLP is an upstream epithelial switch shared by severe asthma and nasal polyps, which is why a single anti-TSLP drug can plausibly address both.
- Tezepelumab proved the crossover is real — approved for asthma in 2021 and for nasal polyps in 2025 — but each indication required its own Phase 3 trial.
- GB-0895 is an AI-designed anti-TSLP antibody now in Phase 3 for asthma, with no nasal-polyp trial underway as of this writing.
- “AI-designed” is a discovery and engineering advantage, not a clinical shortcut; the molecule faces the same evidentiary bar as any antibody.
- Reported early-phase biomarker effects for GB-0895 are preliminary and unpublished, and should not be read as evidence of benefit in polyps.
- The extension to CRSwNP is mechanistically well-grounded and historically precedented, but remains an inference until a dedicated trial is run.
FAQ
Is GB-0895 approved for nasal polyps? No. GB-0895 is investigational and is currently in Phase 3 testing for severe asthma, with no nasal-polyp trial underway. The only anti-TSLP antibody approved for chronic rhinosinusitis with nasal polyps is tezepelumab [Lipworth, Tezepelumab in CRSwNP, 2025].
Does blocking TSLP help nasal polyps? Yes, for the drug that has been tested. In the Phase 3 WAYPOINT trial, tezepelumab shrank polyps and sharply reduced the need for surgery and systemic steroids [Lipworth, Tezepelumab in CRSwNP, 2025]. Whether another anti-TSLP antibody does the same must be shown in its own trial.
Why would an asthma drug work for a sinus disease? Because they overlap. Severe asthma and CRSwNP share TSLP-driven inflammation and are often described as one united airway disease, so a target relevant in the lungs is frequently relevant in the nose [De Corso, TSLP in epithelial-driven diseases, 2024].
Does “AI-designed” mean it will work better? Not necessarily. Machine learning helps design and optimize the antibody, which can improve properties like binding strength and dosing interval, but clinical benefit is decided by trials, not by how the molecule was created.
References
- Lipworth BJ, Han JK, Desrosiers M, et al. Tezepelumab in adults with severe chronic rhinosinusitis with nasal polyps. N Engl J Med. 2025;392(12):1178-1188.
- Menzies-Gow A, Corren J, Bourdin A, et al. Tezepelumab in adults and adolescents with severe, uncontrolled asthma. N Engl J Med. 2021;384(19):1800-1809.
- De Corso E, Hellings PW, Fokkens WJ, et al. Thymic stromal lymphopoietin (TSLP): evidence in respiratory epithelial-driven diseases including chronic rhinosinusitis with nasal polyps. Curr Allergy Asthma Rep. 2024;25(1):7.
- Wang BF, Cao PP, Norton JE, et al. Evidence that oncostatin M synergizes with IL-4 signaling to induce TSLP expression in chronic rhinosinusitis with nasal polyps. J Allergy Clin Immunol. 2023;151(5):1379-1390.
- Generate:Biomedicines. GB-0895 Phase 3 program announcement. 2025.
AstraZeneca’s official press release announcing the FDA approval for CRSwNP: https://www.astrazeneca.com/media-centre/press-releases/2025/us-fda-approves-tezspire-in-crswnp.html
Amgen’s official press release (including the “About TEZSPIRE” product description):
https://www.amgen.com/newsroom/press-releases/2025/10/fda-approves-tezspire-for-chronic-rhinosinusitis-with-nasal-polyps
The official FDA prescribing information:
https://www.accessdata.fda.gov/drugsatfda_docs/label/2023/761224s003lbl.pdf
The company’s official pipeline page:
https://generatebiomedicines.com/pipeline
The official press release announcing the initiation of the Phase 3 trials (SOLAIRIA-1 and -2):
https://generatebiomedicines.com/media-center/generatebiomedicines-to-initiate-global-phase-3-studies-of-gb-0895-a-long-acting-anti-tslp-antibody-for-severe-asthma-engineered-with-ai
The official page on the ERS 2025 Phase 1 results:
https://generatebiomedicines.com/media-center/ers-2025-gb-0895-a-high-affinity-anti-tslp-mab-demonstrates-prolonged-half-life-and-sustained-pharmacological-activity-supporting-every-6-month-dosing-in-asthma
Joonpyo Hong, MD is a board-certified otolaryngologist practicing in Korea. This article reflects his clinical interpretation of published research and does not constitute individual medical advice. This article is not intended to advertise or promote any specific company or product.