
Roughly 90% of patients with early-stage Parkinson’s disease — and a similarly high proportion of those with Alzheimer’s disease — show measurable smell loss, often years before their diagnosis [Doty, Olfactory dysfunction in Parkinson disease, 2012]. What makes this clinically interesting is that AI-assisted neuroimaging is now beginning to quantify the underlying structural changes, turning what was once a subjective complaint into an objective, measurable signal.
This article explains what the research shows, how AI fits into the picture, and — critically — what olfactory dysfunction does not mean for an individual patient.
What the Research Actually Shows
Prevalence in Parkinson’s Disease
Olfactory dysfunction is one of the earliest and most consistent nonmotor features of Parkinson’s disease (PD). In a widely cited review, Doty described olfactory impairment as present in approximately 90% of early-stage PD cases, often preceding the onset of motor symptoms by years [Doty, Olfactory dysfunction in Parkinson disease, 2012]. The mechanism appears to involve early Lewy body pathology — abnormal alpha-synuclein deposits — in the olfactory bulb and related structures, consistent with Braak staging, in which the olfactory bulb and dorsal brainstem structures — particularly the dorsal motor nucleus of the vagus — are affected before the substantia nigra.
Importantly, reduced olfactory sensitivity appears to be relatively specific to synucleinopathies. Conditions such as multiple system atrophy (MSA), corticobasal degeneration (CBD), and progressive supranuclear palsy (PSP) generally show lesser or absent olfactory impairment — making olfactory testing one of several tools that can assist in differentiating idiopathic PD from atypical parkinsonian syndromes [Doty, Olfactory dysfunction in Parkinson disease, 2012].
Progression in Alzheimer’s Disease
In Alzheimer’s disease (AD), olfactory decline follows a different but similarly early trajectory. A meta-analysis by Kotecha et al. found that olfactory identification ability worsens progressively as patients move from mild cognitive impairment (MCI) to confirmed AD, with a large effect size (d = −1.63 for AD vs. healthy controls) [Kotecha et al., Olfactory Dysfunction as a Global Biomarker for Sniffing out Alzheimer’s Disease, 2018]. Notably, olfactory impairment at the MCI stage already shows significant separation from healthy controls (d = −0.81), suggesting that measurable dysfunction precedes the clinical diagnosis of dementia.
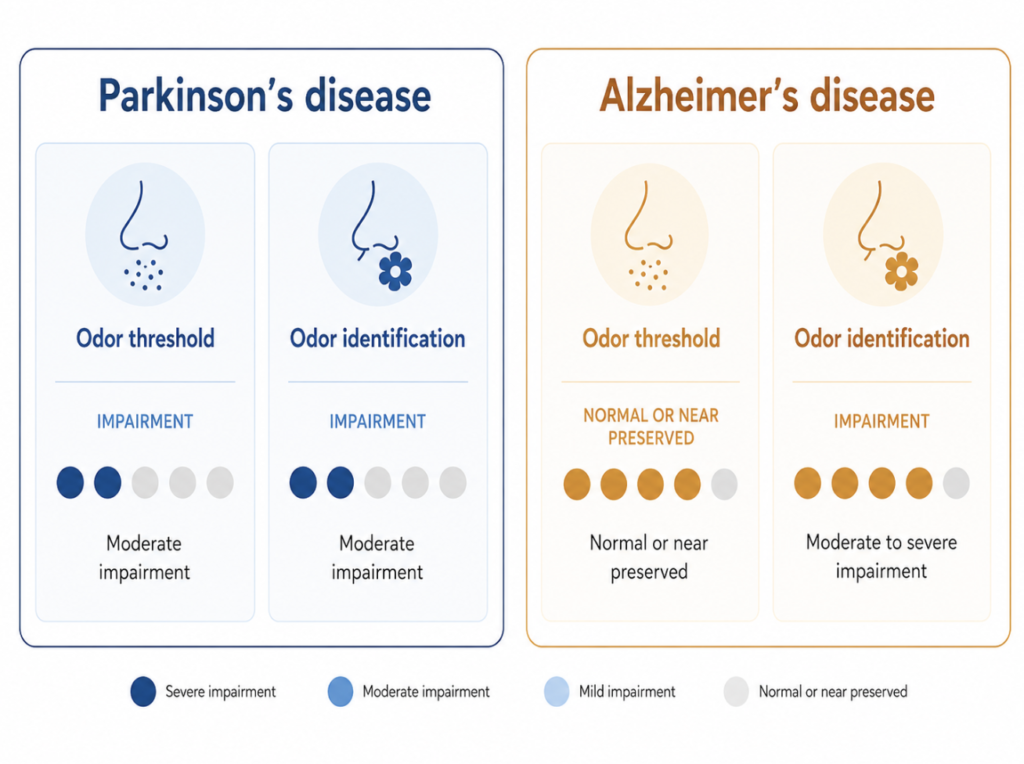
Of the three major olfactory domains — threshold, discrimination, and identification — odor identification appears to be the most consistently affected in the AD spectrum. This distinction matters clinically: patients may not notice gradual threshold shifts, but difficulty recognizing familiar smells (coffee, roses, leather) is more likely to surface as a reportable symptom.
PD vs. AD: Not the Same Deficit
The pattern of olfactory loss differs between the two diseases, and that difference has potential diagnostic value. In PD, both odor threshold and odor identification are impaired. In AD, the impairment is more pronounced in odor identification — the ability to name and recognize familiar smells — while threshold may be relatively preserved in earlier stages. A narrative review in Frontiers in Neuroscience (2025) summarized these distinctions across neurodegenerative conditions, noting that olfactory profiling could contribute to early differential diagnosis when combined with other biomarkers [De Cleene et al., Olfactory dysfunction as potential biomarker in neurodegenerative diseases, 2025].
The Critical Caveat: Association ≠ Individual Risk
Before going further, one clarification this topic demands.
Olfactory dysfunction is statistically associated with neurodegenerative disease at the population level — it is not a diagnostic criterion at the individual level.
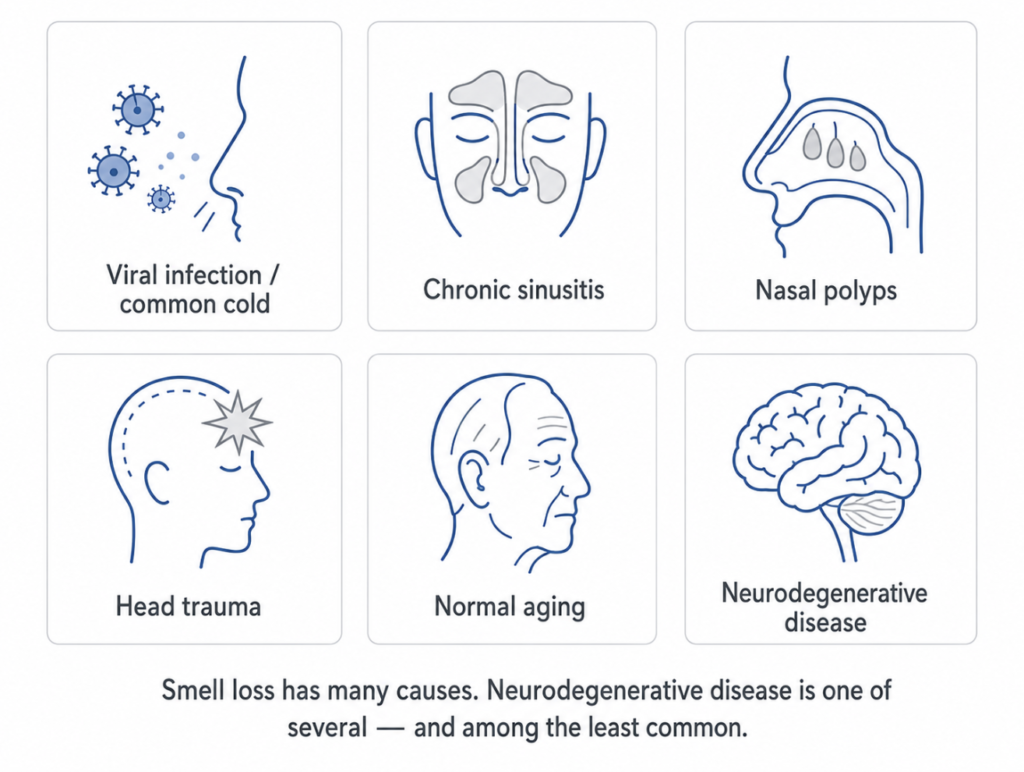
Smell loss is common. It occurs with upper respiratory infections, chronic rhinosinusitis, nasal polyps, head trauma, medication side effects, and normal aging. In people over 65, age-related olfactory decline is nearly universal. The fact that most early-stage PD patients have olfactory dysfunction does not mean that most people with smell loss have PD. The epidemiological framing matters: olfactory testing identifies a subgroup at elevated risk, not a confirmed diagnosis.
This distinction is central to how olfactory biomarkers should be communicated — both in research literature and to patients.
How AI Is Changing the Measurement
Olfactory Bulb Volume on Structural MRI
The olfactory bulb — a small bilateral structure at the base of the frontal lobe that processes incoming olfactory signals — undergoes measurable atrophy in both PD and AD. Traditional MRI morphometry has confirmed volume reduction in these populations, though results have been inconsistent across studies, partly due to the technical difficulty of manually segmenting such a small structure.
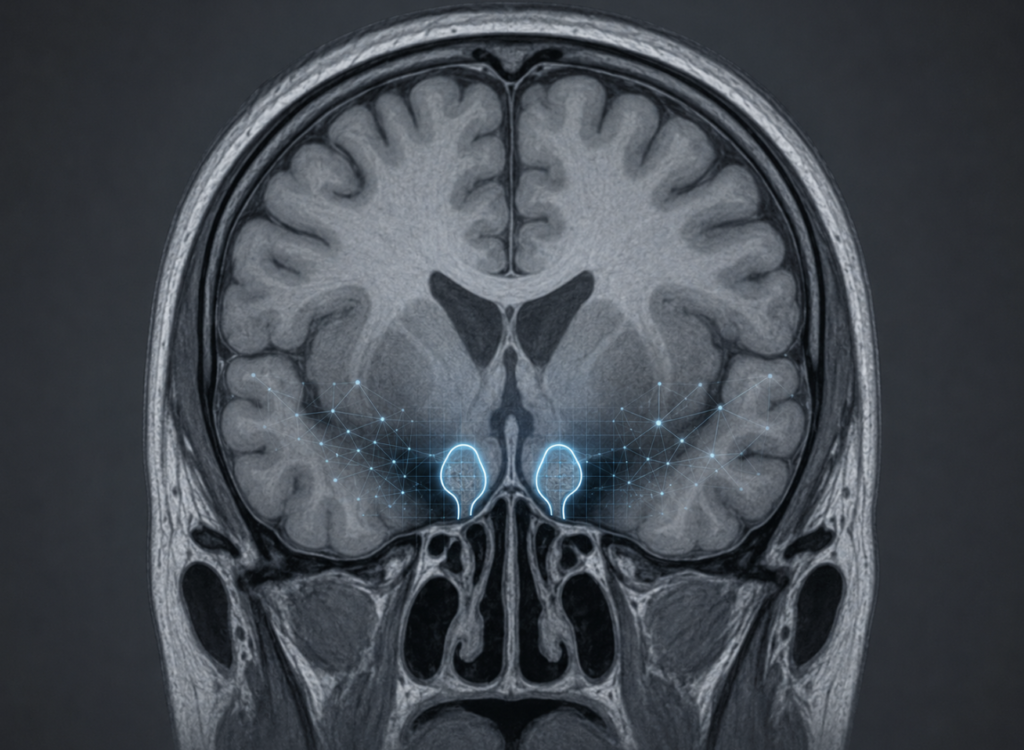
AI-based segmentation is beginning to address this limitation. Deep learning models trained on structural MRI data can now delineate olfactory bulb boundaries with greater reproducibility than manual methods. In one study applying a convolutional neural network (CNN) to olfactory bulb imaging, the model successfully distinguished Parkinson’s disease-related olfactory dysfunction from non-parkinsonian olfactory dysfunction based on morphological features of the bulb and surrounding tissue [Tremblay et al., Olfactory bulb surroundings can help to distinguish Parkinson’s disease from non-parkinsonian olfactory dysfunction, 2020].
A more recent preprint — not yet peer-reviewed — (bioRxiv, October 2025) investigated the neural underpinnings of olfactory dysfunction across the PD and AD spectra, using large-scale cohort data to link olfactory bulb atrophy with both motor and cognitive decline markers [Preprint: Neural Underpinnings of Olfactory Dysfunction across Parkinson’s and Alzheimer’s Spectra, bioRxiv, 2025]. These findings await peer review but are consistent with the broader structural evidence base.
What AI Adds — and Where It Falls Short
AI-assisted olfactory bulb quantification offers two practical advantages over conventional approaches: objectivity (removing rater variability from manual segmentation) and scalability (applicable to existing MRI datasets without additional scanning protocols). These properties make it potentially useful as a research tool and, in the future, as part of a multimodal screening framework.
However, several limitations remain. Olfactory bulb volume alone has modest specificity for any particular neurodegenerative condition. Atrophy is also seen in post-infectious anosmia (including post-COVID-19), head trauma, and other conditions unrelated to neurodegeneration. Current AI models have been validated primarily in research cohorts and have not been prospectively evaluated as clinical screening tools. At this stage, AI quantification of olfactory structures should be understood as a research-grade technique, not a clinical diagnostic standard.
The ENT Perspective: First Point of Contact
Patients who notice a gradual decline in smell often present first to an otolaryngologist. The initial workup appropriately focuses on structural and inflammatory causes: septal deviation, nasal polyps, chronic rhinosinusitis, or post-viral damage. These are far more common causes of olfactory loss than neurodegeneration, and they are treatable.
When the nasal examination and imaging are unremarkable — no structural obstruction, no inflammatory changes — and olfactory loss is persistent and progressive, particularly in a patient over 60 with no identifiable cause, the differential broadens. Standardized olfactory testing tools such as the University of Pennsylvania Smell Identification Test (UPSIT) or Sniffin’ Sticks provide quantitative baselines that can be documented and tracked over time.
The ENT’s role in this context is not to diagnose neurodegenerative disease, but to rule out treatable causes, quantify the deficit objectively, and facilitate appropriate neurological referral when indicated. That coordination — ENT to neurology — is where early olfactory screening has the most potential clinical impact.
Where the Field Is Heading
Several research trajectories are converging. Longitudinal cohorts such as the Parkinson’s Progression Markers Initiative (PPMI) have incorporated olfactory testing at baseline, enabling researchers to track how early smell loss correlates with subsequent cognitive and motor outcomes. Plasma biomarkers (alpha-synuclein, phospho-tau, neurofilament light chain) are increasingly being studied alongside olfactory measures as part of multimodal early-detection frameworks.
The goal is not to replace neurological assessment with a smell test, but to identify the patients most likely to benefit from closer monitoring — years before symptoms become disabling. Whether AI-enhanced olfactory bulb imaging will find a place in that framework as a validated clinical tool remains an open and actively investigated question.
Key Takeaways
- Olfactory dysfunction is present in approximately 90% of early-stage Parkinson’s disease cases and often precedes motor symptoms by years.
- In Alzheimer’s disease, olfactory identification ability worsens progressively from MCI to confirmed dementia, with large effect sizes in meta-analytic data.
- The pattern of olfactory loss differs between PD (threshold + identification) and AD (predominantly identification), which may have differential diagnostic value.
- Smell loss is common and has many causes; olfactory dysfunction is a population-level risk signal, not a diagnosis of neurodegenerative disease in an individual patient.
- AI-assisted segmentation of olfactory bulb volume from structural MRI shows promise as a research tool but remains investigational and is not yet a validated clinical standard.
- Otolaryngologists are typically the first specialists to evaluate olfactory complaints and play a key role in ruling out structural causes and facilitating timely neurological referral.
FAQ
How early can smell loss indicate Parkinson’s disease? Studies show that olfactory dysfunction can precede Parkinson’s motor symptoms by several years in a significant proportion of patients. However, this is a population-level observation — most individuals with smell loss do not have Parkinson’s disease, and smell loss alone is not sufficient to raise clinical suspicion without additional findings.
Can a smell test diagnose Alzheimer’s disease? No. Standardized olfactory tests (UPSIT, Sniffin’ Sticks) can quantify smell function and flag deficits for further evaluation, but they cannot diagnose Alzheimer’s disease. Diagnosis requires comprehensive neurological assessment, neuropsychological testing, and — increasingly — biomarker confirmation.
What is olfactory bulb atrophy? The olfactory bulb is a bilateral brain structure that relays smell signals to cortical areas. In both Parkinson’s and Alzheimer’s disease, this structure undergoes measurable volume reduction. AI-based MRI segmentation can quantify this atrophy with improved consistency compared to manual methods, though clinical applications remain under development.
Should I see an ENT if I lose my sense of smell? Yes, particularly if the loss is persistent and not clearly explained by a recent infection or nasal symptoms. An ENT can evaluate for structural and inflammatory causes, which are far more common than neurodegeneration. If no treatable cause is identified — especially in older adults — further evaluation may be warranted.
Does AI replace clinical assessment in detecting neurodegenerative disease? No. AI tools in this space are research-grade adjuncts. The interpretation of olfactory findings, structural imaging, and biomarker data requires clinical judgment and integration with the patient’s full history.
Joonpyo Hong, MD is a board-certified otolaryngologist practicing in Korea. This article reflects his clinical interpretation of published research and does not constitute individual medical advice.
References
- Doty RL. Olfactory dysfunction in Parkinson disease. Nat Rev Neurol. 2012;8(6):329-39.
- Kotecha AM, Corrêa ADC, Fisher KM, Rushworth JV. Olfactory Dysfunction as a Global Biomarker for Sniffing out Alzheimer’s Disease: A Meta-Analysis. Biosensors (Basel). 2018;8(2):41.
- De Cleene N, Schwarzová K, Labrecque S, Cerejo C, Djamshidian A, Seppi K, Heim B. Olfactory dysfunction as potential biomarker in neurodegenerative diseases: a narrative review. Front Neurosci. 2025;18:1505029.
- Tremblay C, Mei J, Frasnelli J. Olfactory bulb surroundings can help to distinguish Parkinson’s disease from non-parkinsonian olfactory dysfunction. Neuroimage Clin. 2020;28:102457.
- Hwang J, Jung YH, Kang CK, Kim YH. Neural Underpinnings of Olfactory Dysfunction across Parkinson’s and Alzheimer’s Spectra. bioRxiv. 2025. [Preprint]
For more interesting contents:
https://curiousmd.com/olfaction-memory-brain-neurodegenerative-disease/
https://curiousmd.com/role-of-smell-in-flavor/
https://curiousmd.com/ai-electronic-nose/
Link out to:
https://www.ppmi-info.org
https://sensonics.com/product/smell-identification-test/
https://pubmed.ncbi.nlm.nih.gov/22584158/
https://www.mdpi.com/2079-6374/8/2/41