
The bone you can see isn’t always the one that matters. Up to 96% of nasal bone fractures involve the nasal septum as well [Kucker, Nasal Septal Fracture (StatPearls), 2025] — and the septum, hidden inside the nose, often drives the long-term outcome more than the visible bridge.
Nasal bone fractures are the most common facial fracture, making up 40 to 50 percent of all facial bone injuries [Mondin, Management of Nasal Bone Fractures, 2005]. Yet patients routinely present two or three weeks after the injury, surprised to learn they may have already missed the easiest window for treatment. This guide lays out what actually matters in the first two weeks — including when to fix a broken nose, whether you need a CT, when surgery makes sense, and why children play by different rules than adults.
Is It Actually Broken, or Just Swollen?
Swelling can disguise a non-displaced fracture, and it can also fake one. The most reliable signs of a true fracture are visible deformity from the front or in profile, palpable bony irregularity, persistent epistaxis, and nasal obstruction that doesn’t improve as swelling subsides.
A few findings escalate the situation from clinic visit to emergency room: clear watery discharge from one nostril (possible cerebrospinal fluid leak), vision changes, a bluish bulge on the septum (septal hematoma), or persistent bleeding after 20 minutes of direct pressure. These are not “wait and see” findings.
How Broken Noses Actually Happen
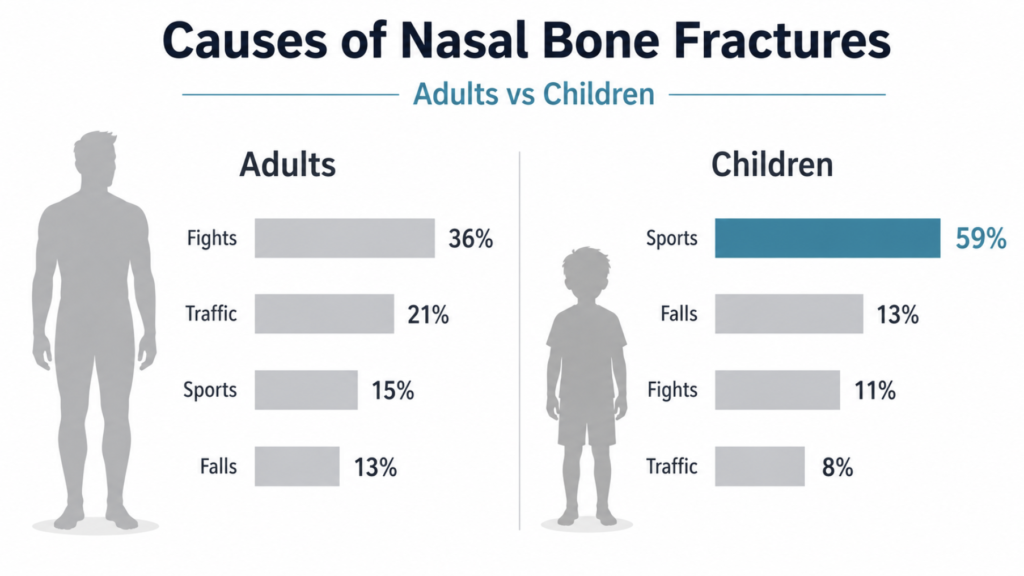
Mechanism predicts pattern, and pattern predicts treatment. In a systematic review of nasal fracture etiologies, the causes differed sharply between adults and children [Hwang, Etiology of Nasal Bone Fractures, 2017]:
| Mechanism | Adults | Children |
|---|---|---|
| Fights and assault | 36.3% | 10.8% |
| Traffic accidents | 20.8% | 8.3% |
| Sports | 15.3% | 59.3% |
| Falls | 13.4% | ~13% |
The direction of the blow matters as much as the force. Lateral impacts typically depress the bone on the struck side and push the contralateral bone outward, while frontal blows tend to splay both nasal bones outward and disrupt the septum at the same time.
Sports-related fractures have a recognizable signature. Contact with another person — often an elbow or a knee to the face — accounts for the majority of sport-related nasal fractures in large series, with team sports (basketball, soccer, football, baseball) carrying the highest incidence. The clinical implication: an elbow to the bridge during a pickup game is a different injury from a frontal fall onto pavement, and the septum is more likely involved in the latter [Erdmann, A Retrospective Analysis of Facial Fracture Etiologies, 2008].
Higher-energy mechanisms — motor vehicle accidents, falls from height, assaults with weapons — demand evaluation of the full midface, not just the nose. An isolated nasal fracture from a high-energy mechanism is unusual.
Simple Fracture vs. Septal Fracture: Why It Changes Everything
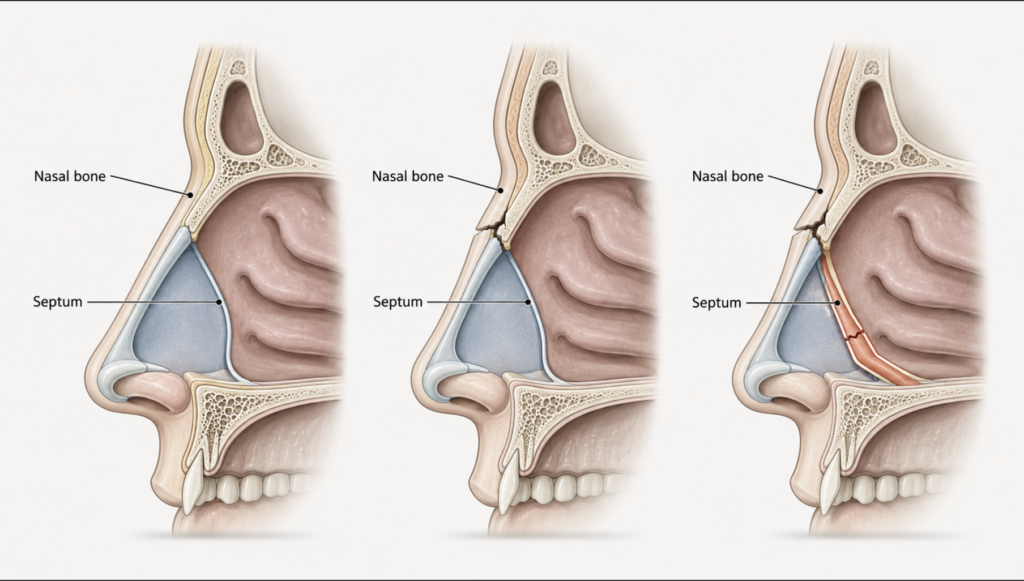
A pure nasal bone fracture without septal involvement is less common than the textbook suggests. Cadaveric and clinical series show septal disruption in the large majority of cases [Kucker, Nasal Septal Fracture (StatPearls), 2025]. This distinction matters because the two scenarios have different treatments and very different prognoses.
Isolated nasal bone fracture. Symptoms are mostly external: deformity, swelling, transient bleeding. Treatment is closed reduction within the treatment window if displaced, or conservative management if non-displaced. Most patients achieve satisfactory functional and cosmetic outcomes when reduction is performed in the optimal window. Cosmetic standards are inherently subjective, however, so a clear preoperative discussion with the surgeon about realistic correction is essential.
Nasal bone fracture with septal involvement. Patients have the external findings plus persistent unilateral nasal obstruction, septal deviation visible on rhinoscopy, and sometimes a saddle nose deformity. Closed reduction can realign the bony pyramid, but a fractured or dislocated septal cartilage tends to spring back to its displaced position. Older literature reported revision rhinoplasty rates of 14 to 50 percent after closed reduction. More recent series, however, suggest the figure is closer to 10 to 20 percent when initial diagnosis carefully evaluates septal involvement — one retrospective analysis of 417 patients found a revision rate of 11.3 percent, with concurrent septal fracture being the strongest predictor of needing later surgery [Besmens, Efficacy of Closed Reduction of Nasal Fractures, 2023]. The practical implication is that accurate assessment of the septum at the time of first diagnosis is the single most important step in avoiding revision.
Septal hematoma is the exception that won’t wait. Blood collecting between the septal mucosa and cartilage cuts off the cartilage’s blood supply. If not drained within 24 to 48 hours, the cartilage dies, and the nose collapses into a saddle deformity that requires major reconstructive surgery to fix. A bluish, boggy septal swelling after trauma is a same-day procedure, not a clinic follow-up.
When to Fix a Broken Nose: 5–10 Days for Adults, 3–7 for Children
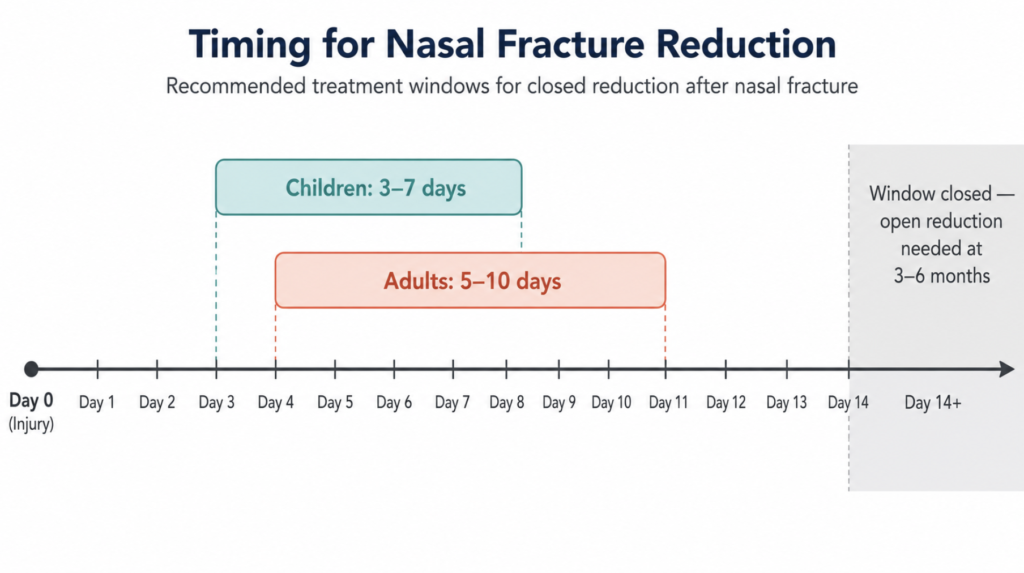
Bone callus begins forming within the first two weeks. Once it does, the fracture is essentially set in its displaced position, and any further correction requires breaking the bone again — an osteotomy rather than a closed reduction.
The practical timeline:
- Days 0–3: Initial swelling peaks. Closed reduction is technically possible but difficult to judge alignment through edema. Most surgeons wait.
- Days 4–10 (adults): Swelling subsides enough to assess shape. This is the sweet spot for closed reduction.
- Days 3–7 (children): Faster healing means earlier intervention.
- After 14 days: Closed reduction success drops sharply. Delayed septorhinoplasty at 3 to 6 months becomes the realistic option.
Waiting past two weeks isn’t a disaster, but it changes the operation from a 15-minute closed reduction under brief anesthesia to a 1- to 2-hour open procedure with longer recovery.
Adults vs. Children: Different Bones, Different Rules
Pediatric nasal fractures are not just smaller versions of adult ones. The bone composition, healing speed, and long-term growth implications all differ.
Children have more elastic bones, more cartilage at the nasal pyramid, and unfused suture lines. Same impact, different fracture pattern: kids more often sustain incomplete or greenstick fractures rather than clean displaced breaks [Hwang, Etiology of Nasal Bone Fractures, 2017]. The visible deformity may be subtler, which is precisely why pediatric nasal fractures are underdiagnosed in emergency departments.
A practical concern unique to children: the nose continues to grow until roughly age 16 in girls and 18 in boys. A displaced fracture in a 7-year-old can disrupt the growth centers and produce a deformity that becomes more obvious as the child grows, not less.
Greenstick Nasal Fractures: The Pediatric Specialty
A greenstick fracture is an incomplete break — one cortex of the bone cracks while the opposite side bends without breaking, like snapping a fresh twig. In nasal bones, this is the dominant pattern in young children because their nasal bones are partly cartilaginous and don’t fracture cleanly.
Greenstick nasal fractures are tricky for several reasons. They often appear normal or equivocal on plain X-ray because there’s no clean fracture line. Even on CT, the fracture segments may be poorly defined. And when surgeons attempt closed reduction, the bent bone tends to spring back toward its displaced position, leaving residual deformity.
The very-young-child question. Parents often ask whether to push for surgery in a 4- or 5-year-old with a clear nasal deformity. The threshold for surgery in young children is generally higher than in adults. General anesthesia carries non-trivial risk in this age group, growth plate disruption is a real consideration, and many minor deformities remodel with growth. For mildly displaced greenstick fractures without functional problems, the preferred approach is active surveillance — regular ENT follow-up to track how the bone settles as the child grows — rather than passive observation. This is a thorough medical decision, not a decision to do nothing: it avoids unnecessary anesthesia risk while protecting the option of definitive correction in adolescence if needed.
Surgery becomes appropriate when there is obvious cosmetic deformity, airway obstruction, septal hematoma, comminution, or persistent bleeding. Outside those scenarios, active surveillance with structured ENT visits is usually the right call.
Do You Actually Need a CT Scan?
Probably not, for an isolated nasal injury. The data make a counterintuitive point clearly: better imaging doesn’t change the decision.
CT is the most sensitive modality, detecting roughly 97% of nasal bone fractures, compared to about 80% sensitivity for plain X-ray [Hong, Identification of Nasal Bone Fractures on Conventional Radiography and Facial CT, 2014]. Ultrasound, in experienced hands, reaches close to 90% sensitivity without radiation exposure.
The catch is that surgical decisions are driven by clinical findings — visible deformity, airway obstruction, septal pathology on rhinoscopy — not by imaging detail. Retrospective studies comparing surgical rates between patients diagnosed by CT versus X-ray have found essentially no difference. The fracture you can feel and see, with airway symptoms you can ask about, is the one that determines treatment.
When CT is genuinely needed:
- Suspected involvement of the orbit, maxilla, frontal sinus, or cribriform plate
- Multiple facial fractures
- High-energy mechanism (MVA, severe assault, fall from height)
- Loss of consciousness or neurological signs
- Pre-operative planning for delayed reconstruction
When X-ray plus exam is enough:
- Isolated nasal injury, low-energy mechanism
- No vision changes, no clear fluid drainage, no neurological signs
- An ENT can palpate and visualize the displacement
For children, the radiation calculus tips further toward avoiding CT. Many pediatric ENT centers manage isolated nasal fractures based on clinical exam and X-ray alone, reserving CT for the same high-energy or complex scenarios as in adults.
From ER Triage to ENT Follow-up: Why Both Matter
Emergency physicians are first responders whose primary job in facial trauma is to rule out life-threatening injuries — head injury, cervical spine fracture, ocular emergencies, and concurrent maxillofacial fractures. This triage role is essential and not interchangeable with specialty care. Once those serious threats are excluded, however, certain nasal-specific findings can be subtle and easily overshadowed by the acute setting.
The patterns that benefit most from prompt ENT follow-up include septal hematoma, which can hide under significant external swelling but is a same-day surgical issue; subtle septal deviation that doesn’t show on imaging but will cause long-term airway problems; and greenstick fractures in children that may read as “negative” on plain X-ray. None of these reflects a failure of emergency care — they reflect the natural division of labor between front-line triage and structural-functional specialty assessment.
The practical recommendation is straightforward: even when initial ER imaging is reassuring, any nose injury with visible deformity, airway change, or significant pain warrants ENT evaluation within 72 hours. This isn’t second-guessing the ER; it’s completing the diagnostic workup that the specialty exam is designed for.
Clinical Perspective
The patients who do worst aren’t the ones with the most severe fractures — they’re the ones who waited. When a patient presents at three weeks with a deviated nose and unilateral obstruction, the closed reduction window is gone, the septum is set in its displaced position, and the realistic plan involves a septorhinoplasty several months later.
AI-assisted image interpretation is changing one specific part of the workflow. Recent deep learning models achieve area under the curve values around 0.85 for detecting nasal bone fractures on plain X-ray, comparable to experienced radiologists [Nam, Diagnosis of Nasal Bone Fractures on Plain Radiographs via Convolutional Neural Networks, 2022]. That’s a meaningful capability — AI can reliably flag a subtle cortical break that a busy emergency physician might miss at 2 a.m.
But finding a fracture line is not the same as deciding what to do about it. The surgical decision depends on factors AI cannot evaluate from a single image: whether there is a septal hematoma bulging behind the mucosa, whether the airway is functionally compromised on either side, whether the septum will spring back after reduction, and what the patient’s pretraumatic nose looked like. Detecting structural bone abnormalities is AI’s domain; integrating that finding with intranasal examination, functional assessment, and patient goals to decide on surgery remains the otolaryngologist’s. The most useful framing is collaborative: AI as a screening tool that catches what humans miss on imaging, and the ENT specialist as the clinician who decides what to do next.
One of the most common patient questions is whether a hairline crack can be left alone. The answer depends entirely on the septum and the airway. A truly isolated, non-displaced nasal bone fracture with a midline septum and clear breathing usually heals with ice and time. Anything else deserves a closer look.
Key Takeaways
- Up to 96% of nasal bone fractures involve the nasal septum as well.
- Adults have a 5–10 day window for closed reduction; children have 3–7 days.
- Recent series show revision rhinoplasty rates of about 10–20% after closed reduction, lower than older 14–50% estimates, when septal involvement is carefully assessed at first diagnosis.
- CT is more sensitive than X-ray (97% vs 80%) but rarely changes surgical decisions for isolated nasal injuries.
- For young children with greenstick fractures, active surveillance with regular ENT follow-up is often preferred over early surgery.
- Sports cause 59% of pediatric nasal fractures but only 15% of adult ones.
- Septal hematoma requires same-day drainage to prevent saddle nose deformity.
Frequently Asked Questions
Does every broken nose involve the septum?
Not every one, but most do — up to 96% in some series. The septum is anatomically tied to the nasal bones, and the same force that displaces the bridge usually disrupts the septum. This is why ENT examination of the septum is essential after any nasal fracture, regardless of how the external nose looks.
Do I need a CT scan for a broken nose?
Usually not, for an isolated nasal injury. CT is more sensitive than X-ray, but studies show similar surgical decision rates regardless of imaging modality. CT is warranted when other facial fractures, orbital injury, or high-energy mechanisms are suspected.
What is a greenstick fracture and why does it matter for my child?
A greenstick fracture is an incomplete break where one side of the bone cracks while the other bends. Children’s flexible bones make this pattern common in pediatric nasal injuries. It matters because greenstick fractures often resist closed reduction and may heal better with observation in young children.
My 5-year-old broke their nose — should we operate or wait?
For most non-displaced or mildly displaced fractures in young children, active surveillance with regular ENT follow-up is the preferred approach — a structured way to monitor how the bone settles as the child grows, not a decision to do nothing. Surgery is reserved for obvious deformity, airway obstruction, septal hematoma, or comminuted fractures. The general anesthesia risk and growth plate considerations in very young children shift the threshold higher than in adults.
What happens if I miss the 10-day window?
Closed reduction becomes progressively less effective as bone callus forms. After 2 weeks, most patients with persistent deformity will need delayed surgical correction — typically a septorhinoplasty performed 3 to 6 months later, when soft tissues have settled.
Is a broken nose more dangerous from sports or from a fight?
Sports-related fractures tend to be more isolated and lower energy, with cleaner reduction outcomes. Assault-related fractures often involve higher force and a greater chance of associated facial fractures, septal disruption, and bilateral involvement. Mechanism matters for both prognosis and the breadth of workup required.
Joonpyo Hong, MD is a board-certified otolaryngologist practicing in Korea. This article reflects his clinical interpretation of published research and does not constitute individual medical advice.
References
- Besmens IS, Shahrdar C, Fontein DBY, Knipper S, Giovanoli P, Lindenblatt N. Efficacy of closed reduction of nasal fractures—a retrospective analysis with focus on factors affecting functional and aesthetic outcomes. J Plast Reconstr Aesthet Surg. 2023;77:371-378.
- Erdmann D, Follmar KE, Debruijn M, et al. A retrospective analysis of facial fracture etiologies. Ann Plast Surg. 2008;60(4):398-403.
- Hong HS, Cha JG, Paik SH, et al. Identification of nasal bone fractures on conventional radiography and facial CT. Iran J Radiol. 2014;11(1).
- Hwang K, Yeom SH, Hwang SH. Etiology of nasal bone fractures. J Craniofac Surg. 2017;28(3):785-788.
- Kucker SC, Patel BC. Nasal septal fracture. In: StatPearls. StatPearls Publishing; 2025.
- Mondin V, Rinaldo A, Ferlito A. Management of nasal bone fractures. Am J Otolaryngol. 2005;26(3):181-185.
- Nam Y, Choi Y, Kang J, Seo M, Heo SJ, Lee MK. Diagnosis of nasal bone fractures on plain radiographs via convolutional neural networks. Sci Rep. 2022;12(1):21510.
For more interesting contents:
https://curiousmd.com/anti-tslp-antibody-nasal-polyps/
https://curiousmd.com/facial-and-neck-lacerations-by-site/
https://curiousmd.com/allergic-vs-nonallergic-rhinitis/
Link out to:
StatPearls – Nasal Septal Fracture (NIH/NCBI):
https://www.ncbi.nlm.nih.gov/books/NBK555912/
AAO-HNS ENThealth – Nasal Fractures:
https://www.enthealth.org/conditions/nasal-fractures/
Mayo Clinic – Broken Nose (Diagnosis & Treatment):
https://www.mayoclinic.org/diseases-conditions/broken-nose/diagnosis-treatment/drc-20370444
PubMed – Nam et al. 2022:
https://pubmed.ncbi.nlm.nih.gov/36513751/