
Your brain decides whether a stranger’s smile is a genuine Duchenne smile or a rehearsed one in less than half a second, and you are usually right without knowing why. The science behind that judgment is more than party trivia. For an otolaryngologist who treats the facial nerve every week, it is a window into how two different brain circuits write on the same face — and why one of them refuses to lie.
This piece walks through the muscles, the timing, and the neurology that separate a genuine smile from a polite one, with a clinical detour through Bell’s palsy and selective neurectomy where the same anatomy becomes a treatment target.
The Two Muscles That Decide
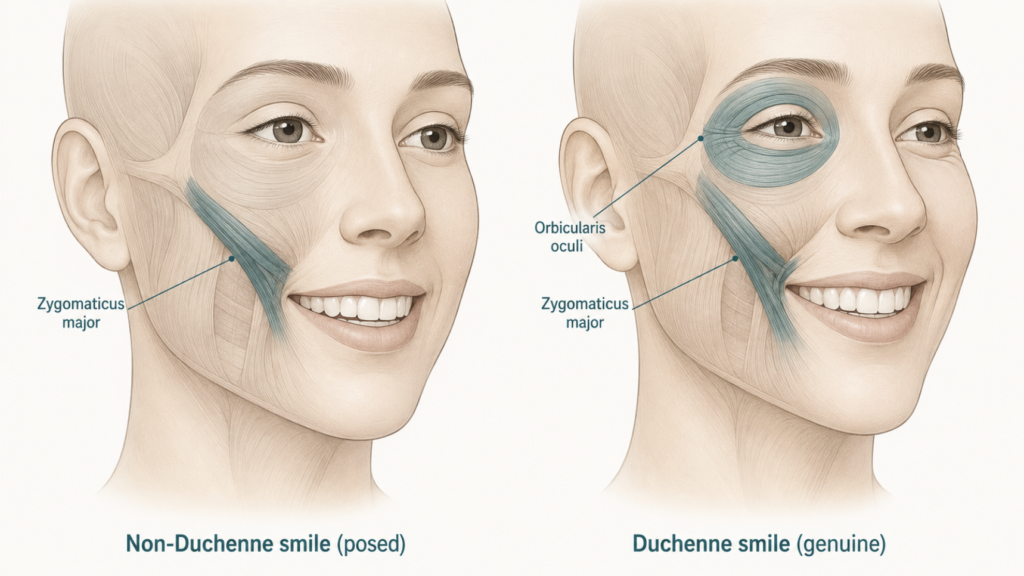
A smile that comes from real enjoyment uses two muscles at once. The zygomaticus major pulls the corners of the lips up and outward. The orbicularis oculi, the ring of muscle that surrounds the eye, contracts at the same time and lifts the cheek, narrows the eye aperture, and creates the small radiating wrinkles at the outer canthus known as crow’s feet. Both muscles are innervated by cranial nerve VII (the facial nerve).
When both fire together during felt joy, the result is what researchers call a Duchenne smile, named after the 19th-century French neurologist Guillaume Duchenne de Boulogne, who isolated this pattern using electrical stimulation in the 1860s. A century later, Ekman, Davidson, and Friesen showed in a controlled study that the Duchenne configuration occurred more often during pleasant film clips than unpleasant ones, tracked left-hemisphere frontal asymmetry on EEG, and matched self-reported positive emotion — while smiles without orbicularis oculi activity did none of these things [Ekman, The Duchenne smile: emotional expression and brain physiology II, 1990].
The catch is the second muscle. Most people can voluntarily contract the zygomaticus major on command — the “say cheese” reflex — but they cannot voluntarily contract the upper portion of the orbicularis oculi (the pars orbitalis) with the same precision. This single asymmetry of motor control is why a posed smile, however wide, often leaves the eyes untouched.
Why Your Brain Can’t Lie With Its Eyes
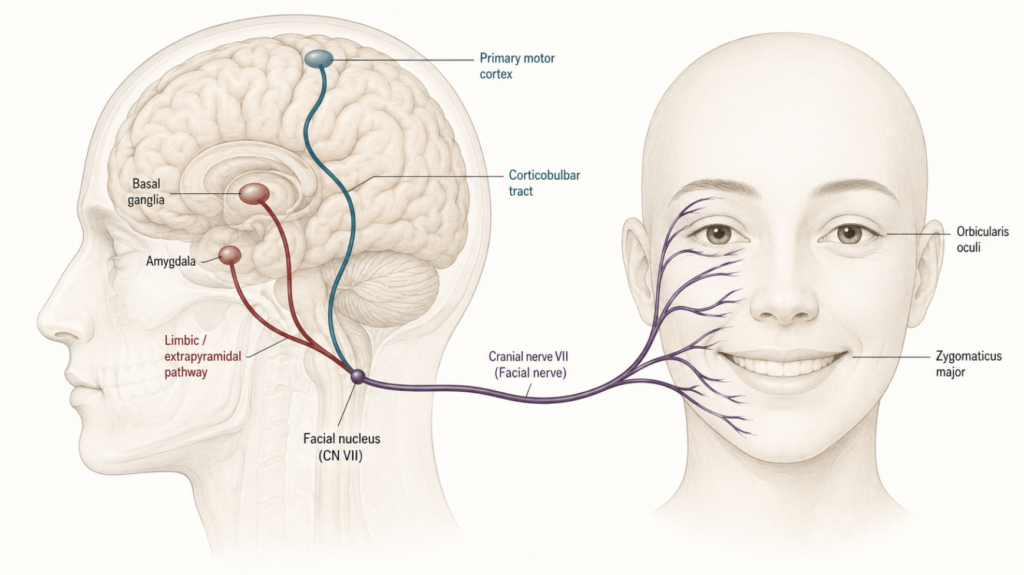
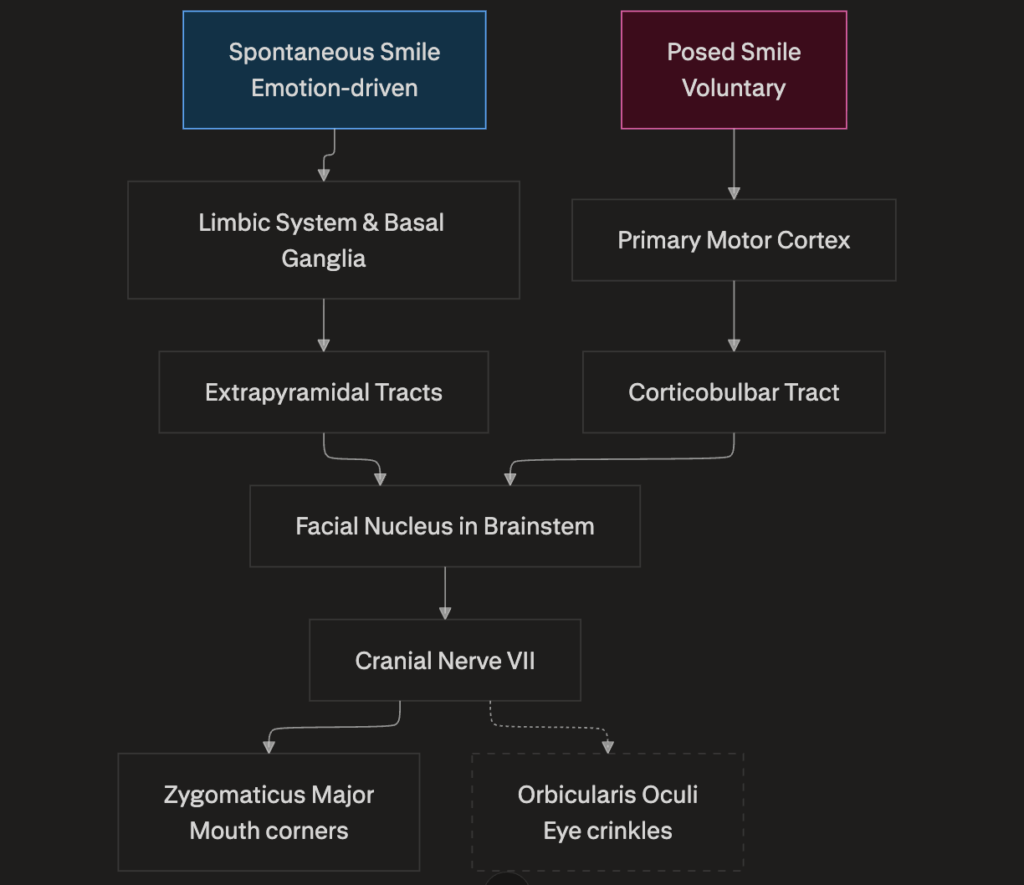
The voluntary–involuntary split is not just convention; it reflects two distinct motor pathways.
Spontaneous emotional smiles originate in subcortical structures — the limbic system, including the amygdala and the basal ganglia — and reach the facial nucleus in the brainstem through extrapyramidal projections.
Posed smiles, by contrast, are generated cortically, driven by the primary motor cortex via the corticobulbar tract. Both routes converge on the same cranial nerve VII and the same muscles, but the cortical route has finer access to the lower face than to the upper periocular muscles. Patients with stroke affecting the corticobulbar tract sometimes lose the ability to smile on command but still smile spontaneously when amused — a dissociation known as volitional facial paresis that demonstrates the two systems are anatomically separable.
Once you know the wiring, the everyday observation makes sense. A polite smile is a cortical motor command; a genuine smile is an emotional reflex.
Beyond the Eyes: Four Other Tell-tale Signs
Crow’s feet are not the only marker, and recent research has made clear that fixating on them alone misses real information.
Timing — onset and offset. Schmidt and colleagues used automated facial image analysis to compare deliberate and spontaneous smiles within the same participants. Deliberate smiles had faster onset speed, faster offset speed, and larger amplitude than spontaneous ones — they snapped on and snapped off [Schmidt, Movement Differences between Deliberate and Spontaneous Facial Expressions: Zygomaticus Major Action in Smiling, 2006]. Spontaneous smiles emerge more gradually and fade more gradually. A smile that arrives on cue and leaves on cue reads as performed.
Symmetry, but not perfect symmetry. Older work suggested genuine smiles were strictly symmetrical and false ones were left-side biased. The picture is more nuanced now: a small amount of dynamic asymmetry (one side leading the other by a few frames) is actually rated as more authentic than perfect mirror-image symmetry. A face that is too synchronized starts to look animated rather than felt.
Duration. Genuine smiles last longer at the apex than posed ones; posed smiles tend to be either too brief or held unnaturally fixed.
Congruence across the face. In a real smile, the upper and lower face tell the same story. In a posed one, the brow may stay flat or even tighten, the eyes may stay wide, and the mismatch is what observers register subconsciously.
The Caveat: When Even Experts Are Fooled
The Duchenne marker is a strong signal, not a polygraph. Two important caveats have surfaced in the last decade.
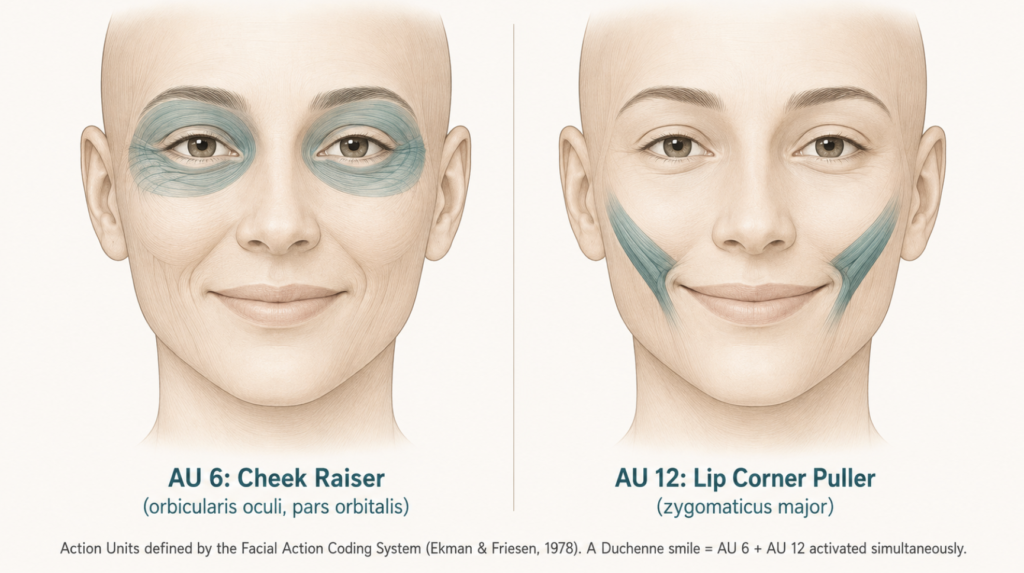
First, the Duchenne smile and a strong smile are confounded: any wide, intense smile recruits more muscle mass, including some orbicularis oculi activity, regardless of whether the underlying emotion is genuine. So orbicularis oculi activation (Facial Action Coding System Action Unit 6) on its own cannot be taken as proof of authenticity.
Second, a minority of people — actors, trained performers, and some children — can voluntarily activate the orbicularis oculi with practice. The muscle is not strictly involuntary; it is just less accessible to volition than the zygomaticus.
A more recent automated analysis using 3D facial landmarks confirmed that the most reliable discrimination between spontaneous and posed smiles came from combining several features at once — Action Unit composition, intensity dynamics, and landmark trajectories — rather than any single cue [Park, Differences in Facial Expressions between Spontaneous and Posed Smiles, 2020]. The takeaway: read the cluster, not the cue.
Deeper Clinical Perspective
From a facial-nerve clinician’s vantage point, the Duchenne smile is not a curiosity — it is a clinical endpoint. Bell’s palsy is a peripheral (lower motor neuron) facial palsy, which means the entire ipsilateral face is affected, including the orbicularis oculi.
That involvement of the upper face is exactly what distinguishes Bell’s palsy from a central (upper motor neuron) palsy, where the forehead and eye are spared by bilateral cortical innervation. During recovery, the return of cheek elevation and a faint crow’s foot can serve as a clinical clue that the upper division of cranial nerve VII is reinnervating — alongside frontalis recovery and eye-closure strength — although crow’s feet return is a clinical observation rather than a standardized item in major facial nerve grading scales such as House-Brackmann or Sunnybrook.
Conversely, when aberrant nerve regeneration produces post-paralytic synkinesis, the orbicularis oculi co-contracts with the zygomaticus, so an attempt to smile triggers an involuntary squint — a configuration that looks Duchenne-like but is uncomfortable for the patient. First-line management is conservative: neuromuscular retraining (facial biofeedback) combined with chemodenervation of the synkinetic orbicularis oculi using botulinum toxin type A [Cooper, Botulinum toxin treatment for facial palsy: A systematic review, 2017].
Surgical options such as selective myectomy or selective neurectomy of the zygomatic branches that innervate the orbicularis oculi are reserved for patients whose synkinesis remains disabling despite first-line treatment [Shikara, Selective neurectomy for treatment of post-facial paralysis synkinesis: a systematic review, 2023]. The same muscle pairing that psychology calls a “marker of genuine emotion” is, in clinical practice, a marker of nerve integrity.
The implication runs in both directions. Botulinum toxin around the periocular region weakens the upper portion of orbicularis oculi, and the same chemodenervation that softens cosmetic crow’s feet is also a workhorse treatment in otolaryngology for post-paralytic synkinesis and facial asymmetry after facial nerve palsy [Cooper, Botulinum toxin treatment for facial palsy: A systematic review, 2017]. In both settings — purely cosmetic and ENT-functional — patients sometimes report that their own smile now “looks fake.” They are not imagining it: the Duchenne marker has been pharmacologically attenuated. In the synkinesis indication this is intentional and beneficial, since it relieves the unwanted eye closure that occurs with smiling; in the cosmetic indication it is an unintended side effect of dosing.
Key Takeaways
- A genuine smile activates two muscles simultaneously — the zygomaticus major and the orbicularis oculi; a posed smile usually activates only the first.
- The orbicularis oculi (the eye-encircling muscle) is largely outside voluntary control in most people, which is why fake smiles fail to reach the eyes.
- Spontaneous and posed smiles travel different brain pathways: subcortical/limbic versus corticobulbar.
- Beyond the muscles, observers also read timing, symmetry, duration, and congruence between the upper and lower face.
- No single feature is foolproof; trained observers and automated systems both perform best when they read multiple cues together.
FAQ
Which facial muscle separates a real smile from a fake one?
The orbicularis oculi — the ring of muscle around the eye. It contracts involuntarily during genuine enjoyment, lifting the cheek and creating crow’s feet at the outer corner. Most people cannot reproduce this contraction on command, so a posed smile leaves the upper face flat.
Can a fake smile ever fool an expert?
Yes. High-intensity posed smiles often recruit orbicularis oculi incidentally because of the muscle mass involved, and a small percentage of people can voluntarily activate the muscle with practice. This is why current research relies on clusters of features — timing, amplitude, symmetry, and Action Unit composition — rather than any single tell.
Why does my smile look different after botulinum toxin around the eyes?
Botulinum toxin used to soften crow’s feet weakens part of the orbicularis oculi. If enough of the muscle is chemoparesized, the Duchenne marker of a felt smile is reduced, which is sometimes perceived by the patient or others as a less authentic expression. The effect is dose-dependent and reversible.
How is the Duchenne smile relevant to facial nerve recovery?
Recovery of orbicularis oculi function after Bell’s palsy or other facial nerve injury restores cheek elevation and crow’s feet on the affected side. The return of this “eye-crinkle” component is a clinical clue that the upper division of cranial nerve VII is reinnervating its target muscles, although it is not a standardized item in formal facial nerve grading scales.
References
Ekman P, Davidson RJ, Friesen WV. The Duchenne smile: emotional expression and brain physiology. II. J Pers Soc Psychol. 1990;58(2):342-353.
Schmidt KL, Ambadar Z, Cohn JF, Reed LI. Movement Differences between Deliberate and Spontaneous Facial Expressions: Zygomaticus Major Action in Smiling. J Nonverbal Behav. 2006;30(1):37-52.
Schmidt KL, Cohn JF, Tian Y. Signal characteristics of spontaneous facial expressions: automatic movement in solitary and social smiles. Biol Psychol. 2003;65(1):49-66.
Park S, Lee K, Lim JA, Ko H, Kim T, Lee JI, Kim H, Han SJ, Kim JS, Park S, Lee JY, Lee EC. Differences in Facial Expressions between Spontaneous and Posed Smiles: Automated Method by Action Units and Three-Dimensional Facial Landmarks. Sensors (Basel). 2020;20(4):1199.
Rychlowska M, Jack RE, Garrod OGB, Schyns PG, Martin JD, Niedenthal PM. Functional Smiles: Tools for Love, Sympathy, and War. Psychol Sci. 2017;28(9):1259-1270.
Cooper L, Lui M, Nduka C. Botulinum toxin treatment for facial palsy: A systematic review. J Plast Reconstr Aesthet Surg. 2017;70(6):833-841.
Shikara M, Bridgham K, Ludeman E, Vakharia K, Justicz N. Selective Neurectomy for Treatment of Post-Facial Paralysis Synkinesis: A Systematic Review. Facial Plast Surg. 2023;39(2):190-200.
Joonpyo Hong, MD is a board-certified otolaryngologist practicing in Korea. This article reflects his clinical interpretation of published research and does not constitute individual medical advice.
For more interesting contents:
https://curiousmd.com/facial-and-neck-lacerations-by-site/
https://curiousmd.com/ramsay-hunt-syndrome-facial-paralysis/
https://curiousmd.com/when-to-fix-a-broken-nose/
Link out to:
https://pubmed.ncbi.nlm.nih.gov/2319446/
https://www.ncbi.nlm.nih.gov/books/NBK482290/
https://pubmed.ncbi.nlm.nih.gov/28389084/