You lie down after a few too many drinks, and the room starts spinning. You sleep it off, wake up the next morning, and the room is now spinning in the opposite direction. Why the room spins when you’re drunk? That isn’t random. It’s physics — your inner ear doing exactly what it was designed to do, except with the wrong kind of fluid running through it.
Most articles blame “dehydration.” That’s part of it, but it leaves out the mechanism that actually makes the world rotate. The real driver is a temporary density mismatch between two microscopic structures inside your semicircular canal. Understanding it explains why nothing — not water, not coffee, not lying still — makes the spinning stop except time and the right kind of fluid.
How Your Semicircular Canals Normally Work
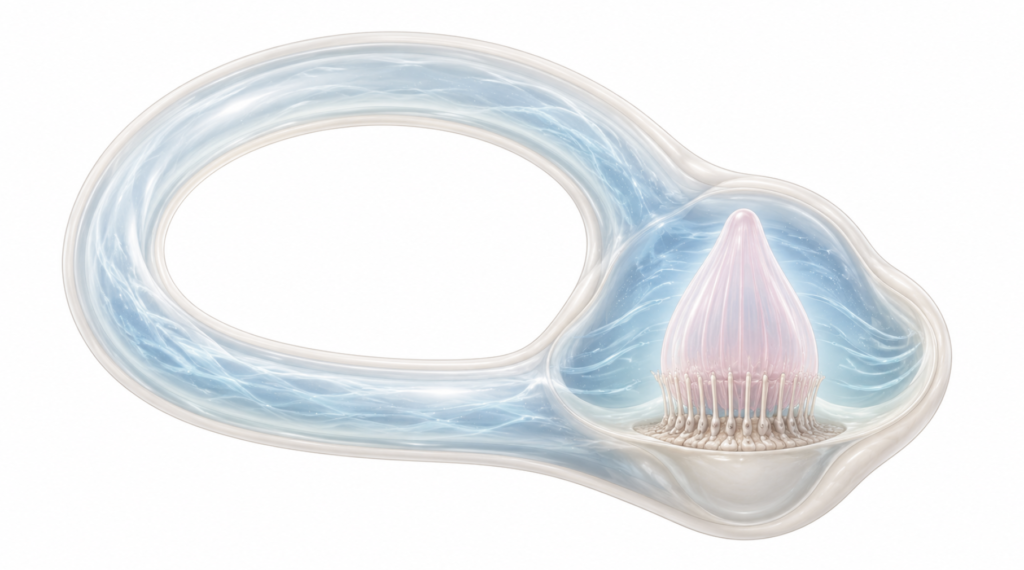
Inside each of your inner ears sit three fluid-filled loops, oriented at right angles so that together they capture rotation in every plane. The fluid is called endolymph. At the base of each loop sits a gelatinous flap called the cupula, with hair cells embedded in it.
Here is the key fact: under normal conditions, the cupula has the same specific gravity (density) as the endolymph. It is neutrally buoyant. Picture a buoy that perfectly matches the density of the water around it — gravity has no preferred direction to push it. This is why your semicircular canals detect rotation only, and ignore gravity and linear movement.
When you actually rotate your head, the endolymph lags behind due to inertia, pushing the cupula sideways, and the hair cells fire. Your brain reads this as rotation. Everything works because cupula and endolymph stay at the same density.
Alcohol breaks that rule.
What Alcohol Actually Does to Your Inner Ear
The phenomenon has a name: positional alcohol nystagmus (PAN). It happens in two phases.
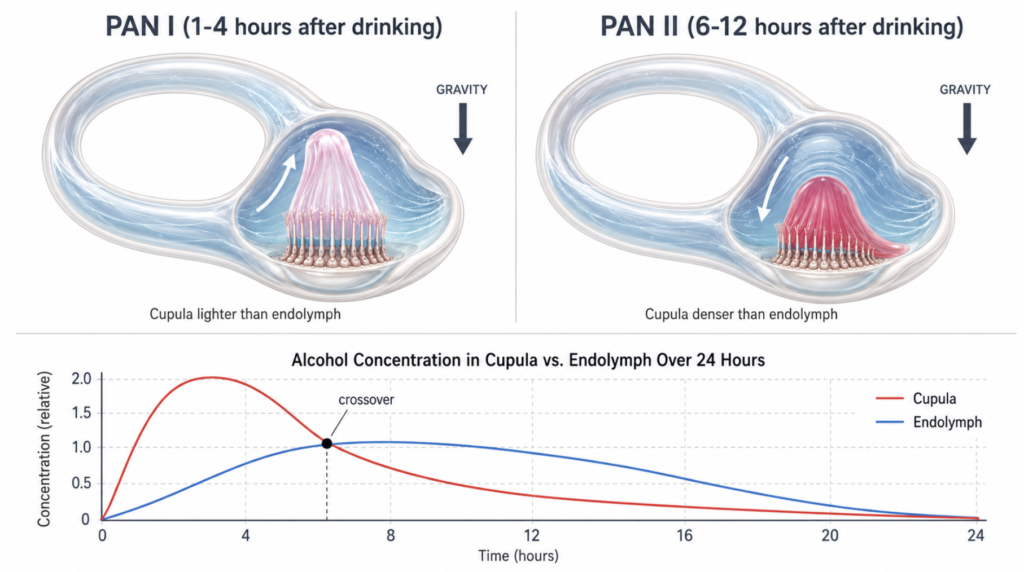
Phase 1 — PAN I (the drinking phase)
Alcohol enters the bloodstream and reaches the cupula faster than the endolymph. For the first several hours after drinking, the cupula becomes lighter than the surrounding endolymph — the classic buoyancy hypothesis, demonstrated and refined over decades of work [Fetter, New Insights into Positional Alcohol Nystagmus, 1999].
The buoy is no longer neutral. It floats. When you tilt your head sideways — lying on a bed, for instance — gravity deflects the cupula upward, and your brain receives a false signal that you are rotating. That is the spinning. Your eyes track the imaginary rotation with rhythmic jerks (nystagmus), which is why fixing your gaze feels impossible.
Phase 2 — PAN II (the hangover phase)
Five to ten hours later, blood alcohol drops. Alcohol now washes out of the cupula faster than out of the endolymph. The cupula is now denser than the fluid around it. The buoy sinks, deflecting in the opposite direction.
This is why morning-after spinning often feels different — sometimes more sway than spin, often reversed in direction. It is PAN I in reverse [Fetter, New Insights into Positional Alcohol Nystagmus, 1999].
A Complementary Modern Insight
In addition to the classical buoyancy hypothesis, a 2020 small-sample study proposed an interesting complementary mechanism [Han, Positional Alcohol Nystagmus and Serum Osmolality, 2020]. The authors examined whether serum osmolality — the concentration of dissolved particles in your blood — might drive a parallel density change in perilymph and endolymph, on top of the direct cupula-diffusion story.
Their data: serum osmolality rose from 286 mOsm/kg before drinking to 303 mOsm/kg at 1 hour (matching the PAN I phase), then dropped to 289 mOsm/kg at 7 hours (matching PAN II). Nine of nine subjects showed corresponding nystagmus shifts.
This is a hypothesis-generating finding in a small cohort, not a replacement for the established buoyancy mechanism. But it adds a plausible whole-body contributor: alcohol’s effect on serum osmolality may be one of several factors shifting inner-ear fluid density. The practical takeaway is that hydration strategy is not just about fluid volume — composition matters too.
Why “The Spins” Get Worse with Eyes Closed
Vision normally helps the brain correct vestibular noise. If your eyes say “the ceiling is still,” the brain dampens the conflicting inner-ear signal. Close your eyes, and that correction disappears. The false rotation signal goes unchecked.
Practical implication: opening your eyes and fixing on a stationary object — a doorframe, a corner of the room — genuinely helps. It is the same principle behind why ballet dancers “spot” a fixed point during pirouettes.
How to Recover Faster — What’s Actually Defensible

Things with mechanistic backing:
- Electrolyte solutions, not just plain water. If osmolality contributes to PAN, the swing in dissolved-particle concentration is the lever. Plain water can over-correct in one direction. Oral rehydration solutions or sports drinks restore the gradient more cleanly.
- Sleep with your head propped up about 30 degrees. This recommendation has an anatomical reason. The lateral semicircular canal sits roughly 30 degrees above the horizontal plane in normal head posture. Lying flat on your back tilts the canal close to perpendicular to gravity, maximizing the deflection force on a non-neutrally-buoyant cupula. Propping up to roughly 30 degrees aligns the canal closer to horizontal, minimizing that effect. No PAN-specific clinical trial has tested this, but it follows directly from inner-ear anatomy and the same conservative-management logic used for other vestibular disorders.
- Open your eyes; fix on a still object. Multisensory integration is the brain’s built-in noise filter.
- Time. PAN resolves when alcohol equilibrates between both compartments — usually within 12 to 24 hours.
Trade-offs to think about:
- Antihistamines such as meclizine or dimenhydrinate. They suppress the vestibular signal but stack sedation on top of residual alcohol. The trade is rarely worth it for mild PAN.
- Coffee — a nuanced one. Caffeine causes cerebral vasoconstriction, which can genuinely help the vasodilatory headache component of a hangover. But it is also a diuretic, which may theoretically slow inner-ear osmolality recovery and prolong the vertigo. The practical compromise: moderate caffeine for the headache if you need it, but pair it with electrolyte hydration rather than drinking coffee alone.
A Speculative Note — IV Fluids for PAN
Disclaimer: The following represents a pathophysiological deduction based on the osmolality hypothesis. It is a personal clinical opinion, not an evidence-based recommendation, and not an official society treatment guideline. No clinical trial has tested IV fluids specifically for PAN.
If the osmolality hypothesis is correct, then one of the upstream drivers of PAN is the serum osmolality swing — not only alcohol diffusing into the cupula. That changes part of the recovery logic.
Isotonic IV fluids — normal saline, possibly with dextrose — should, in theory, normalize serum osmolality faster than oral hydration alone. By that reasoning, an IV could in principle shorten the PAN II phase specifically.
To be clear about what this reasoning is and isn’t:
- Mechanistically plausible under the leading 2020 hypothesis: yes.
- Consistent with how osmotic disturbances are managed in other clinical contexts: yes.
- Tested in any PAN-specific clinical trial: no.
- A reason to seek out commercial “hangover IV” services as routine care: no.
- A substitute for time and oral hydration in mild cases: no.
If someone is severely dehydrated, vomiting, or unable to keep fluids down, an IV in a proper medical setting addresses the dehydration regardless of the PAN question. Using an IV purely to shorten the spinning is, at this point, an inference — not a prescription.
When It’s Not Alcohol Anymore — A Differential Diagnosis Note
Acute PAN is fully reversible and resolves on its own timeline. The clinically important question is what to do when the spinning does not behave like PAN should.
The diagnostic signature of PAN is direction reversal — PAN I one direction, PAN II the opposite — with full resolution within roughly 24 hours of sobriety. Benign paroxysmal positional vertigo (BPPV), by contrast, has a different signature: brief, intense vertigo triggered specifically by head position changes (rolling over in bed, looking up, lying down), no direction reversal over time, and persistence until the displaced otoliths are repositioned [Bhattacharyya, Clinical Practice Guideline BPPV Update, 2017].
A point worth being precise about: alcohol consumption is not an established cause of BPPV. Large epidemiological reviews of BPPV risk factors do not list alcohol among the recognized contributors (head trauma, age-related otolith degeneration, vestibular neuritis, prolonged bed rest, osteoporosis, vitamin D deficiency, migraine, diabetes). The two conditions can occur in the same person purely by coincidence.
The clinical relevance is this: if post-drinking vertigo lasts more than 48 hours, does not reverse direction, or is provoked specifically by positional changes rather than general tilting, the right move is not more hangover remedies — it is an ENT evaluation. A simple repositioning maneuver resolves most BPPV in one or two visits.
There is also a longer-term concern about alcohol itself. Repeated binge drinking has measurable, lasting effects on the vestibulo-ocular reflex [Martellucci, Alcohol Binge-Drinking Damage on the Vestibulo-Oculomotor Reflex, 2021]. The acute episode is reversible. The cumulative pattern is not.
Key Takeaways
- Alcohol-induced spinning is positional alcohol nystagmus (PAN), not “dehydration alone.”
- PAN I (drinking phase): cupula is lighter than endolymph. PAN II (hangover phase): cupula is denser.
- The dominant mechanism is the classical buoyancy hypothesis; serum osmolality changes may contribute as a complementary factor.
- Best mechanistically defensible recovery: electrolyte hydration, head elevation around 30 degrees, visual fixation, and time.
- Vertigo lasting beyond 48 hours, not reversing direction, or provoked by specific head positions needs ENT evaluation for possible BPPV — alcohol does not cause BPPV but the two can coincide.
FAQ
Why does the room spin worse when I lie down?
Lying sideways or supine maximizes the gravitational force acting on a no-longer-neutrally-buoyant cupula, especially because the lateral semicircular canal sits at roughly 30 degrees above horizontal. Sitting upright reduces that effect.
How long does “the spins” last?
Typically until blood alcohol returns to zero AND alcohol clears the endolymph — usually 12 to 24 hours total. PAN II (the morning-after phase) usually fades within 6 to 10 hours after waking.
Why is my morning-after dizziness in a different direction than the night before?
That is PAN II. The cupula has become denser than endolymph as alcohol washes out first, reversing the deflection. Direction-reversing nystagmus is, in fact, one of the diagnostic features of PAN.
Does drinking water cure the spins?
It helps, but plain water can over-correct serum osmolality. Oral electrolyte solutions are more mechanistically sound, especially during the PAN II phase.
Can alcohol damage my inner ear long-term?
Acute PAN is fully reversible. However, chronic binge drinking is associated with measurable vestibulo-ocular reflex impairment [Martellucci, Alcohol Binge-Drinking Damage on the Vestibulo-Oculomotor Reflex, 2021]. It is not only a one-night problem.
References
- Han K, Lee JY, Shin JE, Kim CH. Positional alcohol nystagmus and serum osmolality: new insights into dizziness associated with acute alcohol intoxication. Med Hypotheses. 2020;138:109606.
- Fetter M, Haslwanter T, Bork M, Dichgans J. New insights into positional alcohol nystagmus using three-dimensional eye-movement analysis. Ann Neurol. 1999;45(2):216-223.
- Martellucci S, Ralli M, Attanasio G, Russo FY, Marcelli V, Greco A, et al. Alcohol binge-drinking damage on the vestibulo-oculomotor reflex. Eur Arch Otorhinolaryngol. 2021;278(1):41-48.
- Bhattacharyya N, Gubbels SP, Schwartz SR, Edlow JA, El-Kashlan H, Fife T, et al. Clinical Practice Guideline: Benign Paroxysmal Positional Vertigo (Update). Otolaryngol Head Neck Surg. 2017;156(3 Suppl):S1-S47.
- Brandt T, Daroff RB. The multisensory physiological and pathological vertigo syndromes. Ann Neurol. 1980;7(3):195-203.
- Fregly AR, Bergstedt M, Graybiel A. Relationships between blood alcohol, positional alcohol nystagmus and postural equilibrium. Q J Stud Alcohol. 1967;28(1):11-21.
Joonpyo Hong, MD is a board-certified otolaryngologist practicing in Korea. This article reflects his clinical interpretation of published research and does not constitute individual medical advice.