
Motion sickness aftereffects — the lingering dizziness once the ride ends — have a precise neurological explanation, even when the body is no longer moving. The research now tells us how long they should last, whether you can train them away, and, crucially, which medications help during the ride and which do not help with the dizziness afterward.
How Motion Sickness Works: The Sensory Conflict Model
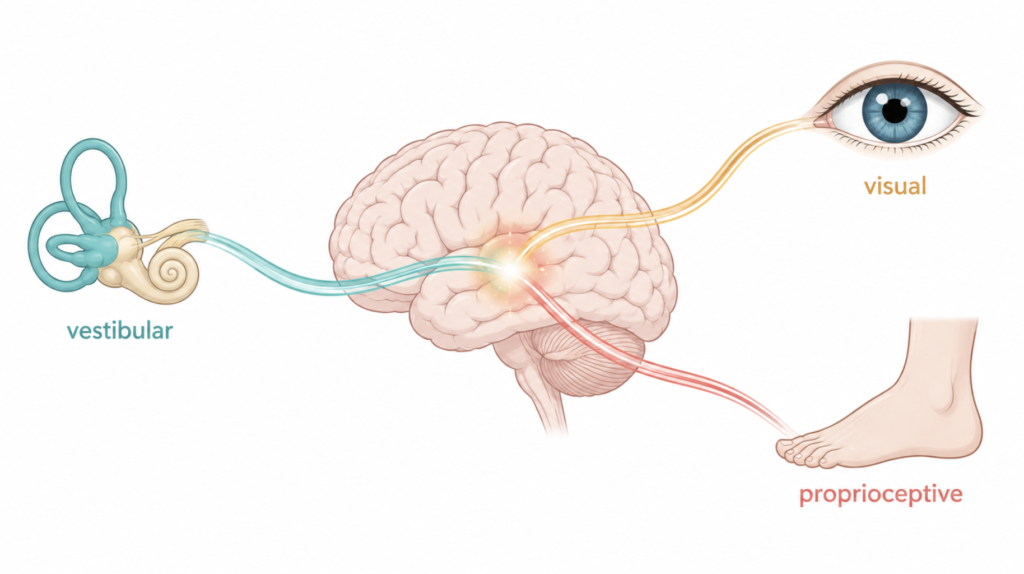
The leading explanation is the sensory conflict hypothesis: your vestibular system (inner ear), vision, and proprioception must agree about how you’re moving. Inside a car, your body is still but your inner ear registers acceleration, braking, and turns. The brain’s internal model of motion can’t reconcile the signals, and the autonomic response — nausea, sweating, dizziness — follows [Golding, Handb Clin Neurol, 2016].
The circuitry involves the vestibular nuclei in the brainstem, the vestibulocerebellum, and autonomic centers. This isn’t a peripheral inner-ear malfunction; it’s a central processing problem, which is why the lingering effects are also central in origin.
Why Motion Sickness Aftereffects Outlast the Ride
The brainstem has a circuit called the velocity storage mechanism — a kind of motion integrator that “remembers” sustained movement to keep your eyes and balance stable. After a long ride, this circuit has been recalibrated to expect motion. When you step out, the recalibration doesn’t reset immediately, so your brain keeps generating a feeling of movement on solid ground [Cha, Ann N Y Acad Sci, 2015].
This produces what clinicians call landsickness — a transient sensation of rocking or swaying after disembarking. Most cases resolve within minutes to a few hours. Anything beyond 48 hours starts moving into a separate diagnostic territory called mal de débarquement syndrome (MdDS) [Van Ombergen, J Neurol, 2016].
| Severity | Duration | What it means |
|---|---|---|
| Normal landsickness | Minutes to hours | Expected; resolves on its own |
| Transient mal de débarquement | Up to 48 hours | Still benign |
| Mal de débarquement syndrome | More than 1 month | Requires specialist evaluation |
Does a Longer Ride Mean Longer Dizziness Afterward?
The intuitive answer is yes — and for ordinary motion sickness, that’s loosely true. Low-frequency oscillations, especially the slow roll of ocean swells, drive stronger and longer vestibular adaptation than high-frequency vibration, which is why sea voyages produce the most prominent aftereffects [Golding, Handb Clin Neurol, 2016].
But the relationship is not linear, and it breaks down for MdDS. The U.S. National Organization for Rare Disorders states explicitly that the duration of motion exposure does not determine the severity or duration of the syndrome. MdDS has been reported after trips of only a few hours and in a person who lived on a boat for a decade [Cha, Ann N Y Acad Sci, 2015].
What seems to matter more than ride length:
- Type of motion — low-frequency, multi-axis motion (boats > cars > planes)
- Individual vestibular sensitivity — measurable and stable across trips
- Comorbid migraine, especially vestibular migraine — a strong risk factor
- Female sex, ages 30–60 — the population with the highest MdDS incidence
Can You Get Used to Motion Sickness? The Habituation Evidence
Yes, and habituation is the single most effective long-term countermeasure — more effective than any drug, with success rates above 85% in military aviation programs [Golding, Handb Clin Neurol, 2016]. But the protocol matters more than most people realize.
What the research says about protocol
Three principles emerge consistently across the desensitization literature:
- Massing of exposures. Sessions must be close together. If intervals exceed roughly one week, long-term habituation largely fails [Bressi, StatPearls, 2023].
- Graded intensity. Start with a stimulus you can tolerate without severe symptoms, then increase. Pushing too hard too fast can trigger sensitization — the opposite of what you want, where the brain becomes more reactive [Golding, Aerosp Med Hum Perform, 2024].
- Specificity. Habituation is stimulus-specific. Getting used to car rides does not protect against seasickness or VR sickness.
Structured vestibular desensitization protocols use repeated graded motion exposures delivered multiple times per week; a pilot study of motion-based equilibrium reprocessing therapy reported substantial reduction in dizziness handicap scores across a multi-session program [Hondebrink, Medicine (Baltimore), 2017]. Military pilot programs run more aggressively: 2–3 weeks of twice-daily graded provocative exposures, followed by graded real flight. Adaptation tends to persist for months — partial retention at one year has been documented in optokinetic studies [Hain, Handb Clin Neurol, 2016].
The practical implication: if you only take long car rides every few weeks, you will keep getting sick. If you ride daily for two weeks, you will likely habituate.
Medications: What Actually Works (and What Doesn’t)
The clinical pharmacology of motion sickness divides cleanly into two questions: preventing sickness during motion, and treating dizziness that lingers afterward. The answers are very different.
For prevention before and during motion
Scopolamine transdermal patch is first-line. A 1.5 mg patch applied behind the ear at least 4 hours before exposure (8 hours is better) provides about three days of protection. Cochrane review data show a roughly 75% reduction in motion-induced nausea and vomiting versus placebo [Spinks, Cochrane Database Syst Rev, 2011]. The mechanism is central anticholinergic — blocking acetylcholine in the vestibular nuclei to dampen the conflict signal. Side effects: dry mouth, blurred vision, drowsiness. Contraindicated in narrow-angle glaucoma and urinary retention.
First-generation antihistamines are the standard alternative: meclizine (typically 12.5–25 mg up to three times daily, though regimens vary by formulation, age, and country — always follow product labeling and clinician guidance), dimenhydrinate, cinnarizine, and promethazine. Depending on the country, dimenhydrinate, cinnarizine, or promethazine may be more commonly prescribed than meclizine. A 2022 Cochrane review found antihistamines prevent motion sickness in about 40% of susceptible individuals versus 25% on placebo (RR 1.81) [Karrim, Cochrane Database Syst Rev, 2022]. Their efficacy comes from central anticholinergic effects, not from H1 blockade. Meclizine causes less drowsiness than dimenhydrinate and lasts longer.
What does not work, despite frequent over-the-counter claims:
- Second-generation antihistamines (cetirizine, fexofenadine, loratadine) — designed not to cross the blood-brain barrier, so they have no effect on the central vestibular centers [Brainard, Am Fam Physician, 2014].
- Ondansetron and other 5-HT3 antagonists — highly effective for chemotherapy-induced nausea but generally not recommended for motion sickness, because the site of action is not the central vestibular pathway.
- Ginger — popular, but recent evidence reviews classify it as not reliably effective for motion sickness prevention.
For the lingering dizziness after the ride
Here is the part most patients (and many clinicians) get wrong: motion sickness medications are designed to prevent the sickness, not to treat the residual dizziness afterward.

For benign landsickness lasting a few hours, no drug is indicated — it resolves on its own. For persistent mal de débarquement syndrome, the data are striking: neither meclizine nor scopolamine has been shown to help [Hain, Handb Clin Neurol, 2016; Van Ombergen, J Neurol, 2016]. Vestibular suppressants don’t reverse a maladapted central model — and in some patients they may slow re-adaptation.
What does have evidence in MdDS:
- Benzodiazepines (clonazepam, diazepam) — most consistently helpful in surveys and small studies, but with addiction risk that limits long-term use [Hain, Arch Otolaryngol Head Neck Surg, 1999].
- SSRIs and SNRIs — modest benefit reported, possibly via central modulation [Mucci, Front Neurol, 2020].
- Tricyclic antidepressants and migraine prophylaxis — useful subsets, especially when vestibular migraine overlaps [Ghavami, Laryngoscope, 2017].
Clinical Perspective
Most lingering post-ride dizziness is benign and resolves within hours without treatment. There are no formally standardized criteria for when post-motion dizziness warrants further evaluation, but clinically relevant red flags include:
- Duration beyond 48 hours
- Rotational vertigo (true spinning, not rocking)
- Hearing changes, severe headache, or any focal neurologic signs
- Recurrent dizziness without any motion trigger
In these cases, the differential expands to vestibular migraine, MdDS, BPPV, orthostatic hypotension, or central causes — conditions that require diagnostic workup rather than continued use of vestibular suppressants.
Key Takeaways
- Post-motion dizziness reflects the brain’s velocity storage mechanism still running an outdated motion model.
- Normal landsickness resolves within hours; persistence beyond 48 hours warrants medical evaluation.
- Trip length is a weak, nonlinear predictor of aftereffect duration — motion type and individual sensitivity matter more.
- Habituation works in over 85% of cases when sessions are massed (3× weekly, graded intensity) and stimulus-specific.
- Scopolamine and first-generation antihistamines prevent motion sickness; they do not reliably treat the dizziness that persists afterward.
FAQ
Q: How long does motion sickness last after the car stops? A: For most people, minutes to a few hours. Up to 48 hours is still considered transient landsickness. Beyond that, see a doctor — persistent symptoms can indicate mal de débarquement syndrome or another vestibular condition.
Q: Does the length of the ride determine how long I’ll be dizzy afterward? A: Only loosely. Lower-frequency motion (boats more than cars) and individual vestibular sensitivity matter more than raw ride duration. For mal de débarquement syndrome specifically, research shows trip length does not predict symptom duration.
Q: Can I train myself to stop getting carsick? A: Yes. Repeated, closely-spaced exposures with gradually increasing intensity can produce lasting habituation in most people. The key constraint is timing — if you space exposures more than about a week apart, the adaptation does not consolidate.
Q: What’s the most effective motion sickness medication? A: The scopolamine transdermal patch shows the strongest evidence for prevention, with roughly 75% reduction in nausea and vomiting in clinical trials. First-generation antihistamines like meclizine are the standard alternative when scopolamine is contraindicated.
Q: Will motion sickness pills help the dizziness I feel after the ride? A: Generally no. Standard motion sickness drugs are designed for prevention during motion, and for the lingering dizziness afterward — especially mal de débarquement — meclizine and scopolamine have not been shown to help. If symptoms persist beyond 48 hours, the treatment approach is entirely different and should be guided by a specialist.
References
- Golding JF. Motion sickness. Handb Clin Neurol. 2016.
- Cha YH. Mal de debarquement syndrome: new insights. Ann N Y Acad Sci. 2015.
- Van Ombergen A, Van Rompaey V, Maes LK, Van de Heyning PH, Wuyts FL. Mal de debarquement syndrome: a systematic review. J Neurol. 2016.
- Hain TC, Cherchi M. Mal de débarquement syndrome. Handb Clin Neurol. 2016.
- Hain TC, Hanna PA, Rheinberger MA. Mal de debarquement. Arch Otolaryngol Head Neck Surg. 1999.
- Mucci V, Indovina I, Browne CJ, Blanchini F, Giordano G, Marinelli L, Burlando B. Mal de Debarquement Syndrome: A Matter of Loops? Front Neurol. 2020.
- Hondebrink MS, Mert A, van der Lint R, de Ru JA, van der Wurff P. Motion-based equilibrium reprocessing therapy a novel treatment method for chronic peripheral vestibulopathies: A pilot study. Medicine (Baltimore). 2017.
- Golding JF, Alund D, Gresty MA, Flynn MB. Sensitization of Visually Induced Motion Sickness by Prior Provocative Physical Motion. Aerosp Med Hum Perform. 2024.
- Spinks A, Wasiak J. Scopolamine (hyoscine) for preventing and treating motion sickness. Cochrane Database Syst Rev. 2011.
- Karrim N, Byrne R, Magula N, Saman Y. Antihistamines for motion sickness. Cochrane Database Syst Rev. 2022.
- Ghavami Y, Haidar YM, Ziai KN, Moshtaghi O, Bhatt J, Lin HW, Djalilian HR. Management of mal de debarquement syndrome as vestibular migraines. Laryngoscope. 2017.
- Brainard A, Gresham C. Prevention and treatment of motion sickness. Am Fam Physician. 2014.
- Bressi F, Cricenti L, Bressi M, et al. Motion Sickness. StatPearls. 2023.
Joonpyo Hong, MD is a board-certified otolaryngologist practicing in Korea. This article reflects his clinical interpretation of published research and does not constitute individual medical advice.
For more interesting contents:
https://curiousmd.com/room-spins-when-youre-drunk/
https://curiousmd.com/vestibular-neuritis/
Link out to:
https://rarediseases.org/rare-diseases/mal-de-debarquement/
https://www.cochranelibrary.com/cdsr/doi/10.1002/14651858.CD002851.pub4/full
https://my.clevelandclinic.org/health/diseases/24796-mal-de-debarquement-syndrome-mdds
https://vestibular.org/article/diagnosis-treatment/types-of-vestibular-disorders/mal-de-debarquement/