You are sitting at your desk and suddenly a sharp, deep stab of pain shoots through one ear. Three seconds later it is gone. No fullness, no ringing, no warning — just a single, vivid jab. A week later, it happens again. Then nothing for a month.
This kind of brief, stabbing ear pain is one of the most common ear complaints seen in ENT clinics, and one of the most over-googled. Most online articles lump it together with infections, earwax, and TMJ — none of which fit this pattern. What you are likely experiencing is a benign entity referred to in this article as primary stabbing otalgia. Below is what defines it, how to tell it apart from the conditions it can mimic, and the small set of red flags that actually warrant evaluation.
The Symptom Pattern That Defines It
Primary stabbing otalgia has a remarkably consistent fingerprint. If your pain matches all of the following, you have already done most of the diagnostic work:
- Sudden onset with no warning
- Sharp, stabbing, or “ice-pick” in quality
- Deep inside the ear — not behind it, not in front of it
- Lasts only seconds, rarely longer than ten
- Resolves completely on its own, leaving no residual ache
- Episodes are irregular — days, weeks, or months apart
- No other ear symptoms — no hearing loss, no discharge, no fullness, no dizziness
- No trigger — not provoked by chewing, swallowing, jaw movement, or touch
The most diagnostically powerful feature is the combination of brevity and isolation: seconds long, and accompanied by nothing else. Almost every serious cause of ear pain produces something more — a fever, a ringing, a fullness, a discharge, a duration measured in minutes or hours [Earwood, Ear Pain: Diagnosing Common and Uncommon Causes, 2018].
What Is Primary Stabbing Otalgia?
Primary stabbing otalgia is a benign, idiopathic ear pain syndrome characterized by brief, neuralgia-like jabs of pain in the absence of detectable ear pathology. “Primary” means no underlying disease is found on examination or imaging; “idiopathic” means the precise mechanism remains unknown.
It belongs to the same family as primary stabbing headache — the so-called “ice-pick headache” — a well-recognized condition under the International Classification of Headache Disorders, 3rd edition (ICHD-3). It is worth noting that ICHD-3 formally codifies primary stabbing headache, but does not list a separate ear-localized entity. The term “primary stabbing otalgia” is used in this article — and increasingly in clinical writing — to describe the same pain pattern when it is anatomically restricted to the ear, since it shares its phenomenology, benign course, and presumed mechanism with the cephalic form.
ICHD-3 criteria for primary stabbing headache describe spontaneous, single or serial stabs lasting up to a few seconds, recurring at irregular intervals, without cranial autonomic features. Population-based epidemiology supports that these brief stabbing pains are common: in the Vågå study of headache epidemiology, idiopathic stabbing headache was verified in 35.2% of 1,838 adult parishioners interviewed — meaning roughly one in three people will experience this kind of brief stab at some point in life [Sjaastad, The Vågå study; epidemiology of headache I: the prevalence of ultrashort paroxysms, 2001]. A portion of these stabs localize to the ear rather than the scalp or temple — and clinically, those cases behave identically.
Primary stabbing otalgia is a diagnosis of exclusion. The label is appropriate only after history and examination rule out structural, infectious, or referred causes. When the pattern is textbook and the ear exam is normal, the workup ends quickly [Coulter, Otalgia, 2024].
What It Is NOT: Other Causes of Stabbing Ear Pain
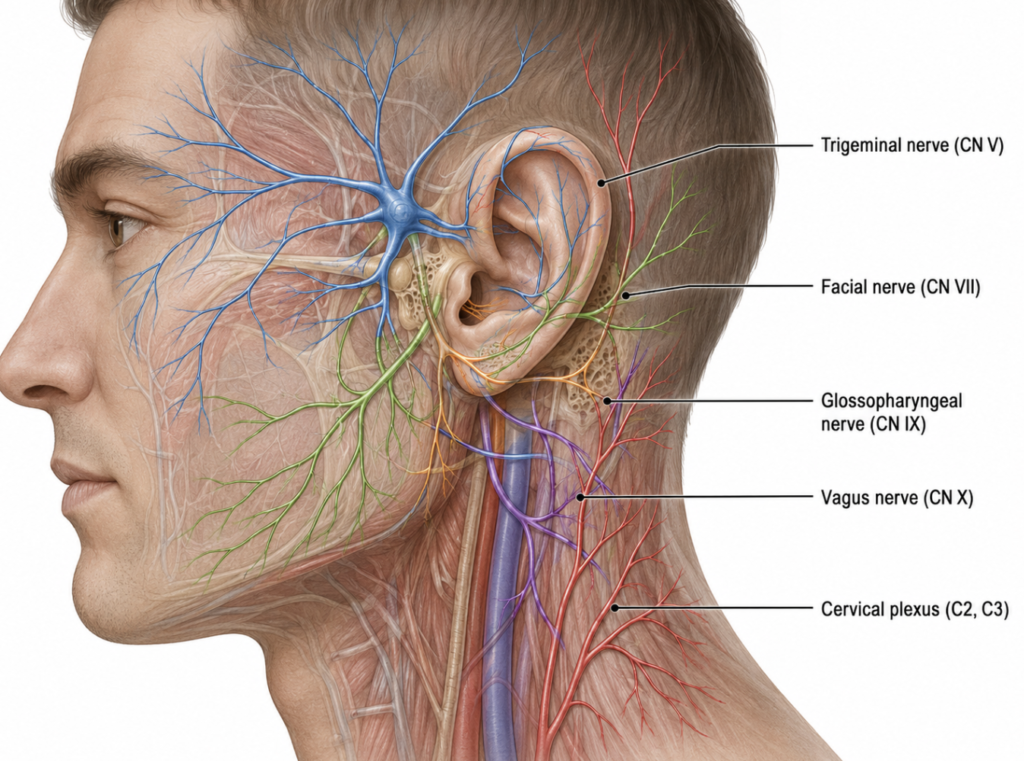
The ear receives sensory input from four cranial nerves (V, VII, IX, X) and the cervical plexus, which is why ear pain has such a long differential. Most of those causes, however, look nothing like primary stabbing otalgia once compared side by side.
| Cause | Duration | Triggers | Other symptoms |
|---|---|---|---|
| Primary stabbing otalgia | Seconds | None | None |
| TMD (temporomandibular disorder) | Minutes to hours, dull | Chewing, jaw movement | Jaw clicking, locking, facial soreness |
| Glossopharyngeal neuralgia | Seconds | Swallowing, talking, coughing | Throat pain radiation |
| Geniculate (nervus intermedius) neuralgia | Seconds | Touch in the ear canal | Possible trigger zone in canal; sometimes tearing, taste changes |
| Acute otitis media / externa | Hours to days, constant | None | Fever, discharge, hearing loss, fullness |
| Eustachian tube dysfunction | Variable | Altitude, colds | Fullness, popping, muffled hearing |
| Referred otalgia (dental, cervical, pharyngeal) | Variable | Chewing, neck motion, swallowing | Source-specific symptoms |
Two distinctions matter most. TMD (temporomandibular disorder), historically referred to as Costen syndrome, produces a dull, persistent ache linked to jaw function — fundamentally different from a soundless, triggerless, seconds-long jab [Visvanathan, 12 minute consultation: an evidence-based management of referred otalgia, 2010]. Glossopharyngeal and geniculate neuralgia can both cause brief, sharp ear pain, but they are nearly always provoked — by swallowing in the case of glossopharyngeal, by tactile stimulation of the ear canal in the case of geniculate — and they tend to occur in clusters rather than as isolated jabs spread weeks apart [Robblee, A pain in the ear: two case reports of nervus intermedius neuralgia and narrative review, 2021].
Why It Happens (Best Current Understanding)
The leading hypothesis is transient, spontaneous misfiring of sensory nerve fibers in the ear region — the same mechanism proposed for primary stabbing headache. Because four cranial nerves and two cervical roots all send branches to the ear, even a small, brief electrical disturbance in any one of them can register as a deep, focal stab.
Imaging is typically normal. There is no compression, no tumor, no demyelination to find — which is why ENTs and neurologists do not reflexively order MRI for this presentation, reserving it for cases with red flags or atypical features [Fernandez-Vial, A Rare Case of Idiopathic Painful Nervus Intermedius Neuropathy in a 13-Year-Old Female: A Case Report and Discussion in the Context of the Literature, 2022].
Patients commonly identify stress, fatigue, weather shifts, or minor temporomandibular tension as informal triggers, though no single factor has been confirmed.
When You Should See an ENT (Red Flags)
The pattern matters more than the pain itself. Reassessment is appropriate if any of the following appear:
- Episodes lasting longer than a minute
- Pain becoming more frequent or more intense over time
- Hearing loss, tinnitus, or fullness in the same ear
- Dizziness or balance problems
- Facial weakness or numbness
- Discharge or bleeding from the ear
- Night pain that wakes you up
- Unexplained weight loss, neck lumps, or persistent unilateral symptoms
Persistent unilateral ear pain — especially in adults with risk factors such as smoking or significant alcohol use — warrants evaluation for head and neck malignancy even when the otoscopic exam is normal [Earwood, Ear Pain: Diagnosing Common and Uncommon Causes, 2018].
Treatment: Usually None Needed
For most patients, the right “treatment” is reassurance and observation. Episodes tend to remain infrequent, self-limited, and often diminish over months to years.
When attacks become frequent enough to disrupt daily life, low-dose neuropathic agents — carbamazepine, gabapentin, or oxcarbazepine — are sometimes considered, though evidence is limited to related entities such as nervus intermedius neuralgia and primary stabbing headache rather than primary stabbing otalgia itself. What does not help, and is often tried unnecessarily, is antibiotic ear drops, oral decongestants, or earwax removal: none of these address the underlying neural mechanism.
Clinical Perspective
A simple two-question filter is useful in clinic before reaching for any test:
- Does each stabbing episode last only seconds?
- Are there any other ear symptoms at all — hearing change, fullness, ringing, dizziness, discharge?
If the answer to the first is yes and the answer to the second is no, the diagnosis is almost always primary stabbing otalgia. A 60-second otoscopic and tuning-fork exam confirms it. What patients often benefit from most is not a prescription but a clear explanation of the pattern — because once the fingerprint is recognized, the anxiety attached to each new episode tends to fade.
The internet’s failure here is structural. Most patient-facing articles on “sharp ear pain” are written around infection or TMJ, because those are the two diagnoses with marketable treatments. Primary stabbing otalgia gets little coverage precisely because the right answer is usually to do nothing — which is also why patients keep googling it.
Key Takeaways
- Brief stabbing ear pain lasting only seconds, with no other symptoms, is most often primary stabbing otalgia — a benign condition.
- It is a diagnosis of exclusion, but the pattern is highly recognizable: seconds long, no triggers, no associated symptoms.
- ICHD-3 codifies primary stabbing headache; the ear-localized form is not separately classified but is clinically analogous.
- It is not TMD (which is triggered by chewing) or glossopharyngeal neuralgia (which is triggered by swallowing).
- Red flags include episodes lasting more than a minute, hearing changes, dizziness, facial weakness, or any ear discharge.
- Most patients need reassurance, not treatment; medication is reserved for frequent, disabling attacks.
FAQ
Is brief stabbing ear pain dangerous?
In most cases, no. When the pain lasts only a few seconds, resolves spontaneously, and is not accompanied by other ear symptoms, it is almost always benign. Persistent, progressive, or symptomatic ear pain is a different matter and warrants evaluation.
What is primary stabbing otalgia?
Primary stabbing otalgia is a benign, idiopathic ear pain syndrome characterized by brief, sharp jabs of pain — typically lasting seconds — without identifiable underlying disease. It is closely related to primary stabbing headache, the ICHD-3 codified entity sharing the same phenotype but localized to the head rather than the ear.
How common is this kind of pain?
Population studies of primary stabbing headache report a lifetime prevalence of roughly 35%, meaning around one in three adults will experience these brief stabbing pains at some point. The ear-localized subset, while less precisely quantified, is clinically familiar to most ENT clinicians.
How long should I wait before seeing a doctor?
If the pattern stays consistent — seconds long, no other symptoms, irregular intervals — watchful waiting is reasonable. Seek evaluation if duration extends, frequency increases, or new ear symptoms develop.
Can stress or fatigue trigger this kind of ear pain?
Many patients report stress, sleep deprivation, or weather changes around their episodes, although no single trigger has been formally confirmed in the medical literature.
Will primary stabbing otalgia go away on its own?
For most patients, yes. Episodes tend to remain infrequent and often decrease over time. A small subset develops frequent attacks that may respond to neuropathic medications under specialist care.
References
Coulter J, Hohman M, Kwon E. Otalgia. In: StatPearls. Treasure Island (FL): StatPearls Publishing; 2024.
Earwood JS, Rogers TS, Rathjen NA. Ear Pain: Diagnosing Common and Uncommon Causes. Am Fam Physician. 2018;97(1):20-27.
Fernandez-Vial D, Sangalli L, Perez C. A Rare Case of Idiopathic Painful Nervus Intermedius Neuropathy in a 13-Year-Old Female: A Case Report and Discussion in the Context of the Literature. Children (Basel). 2022;9(8):1234.
Robblee J. A pain in the ear: two case reports of nervus intermedius neuralgia and narrative review. Headache. 2021;61(3):414-421.
Sjaastad O, Pettersen H, Bakketeig LS. The Vågå study; epidemiology of headache I: the prevalence of ultrashort paroxysms. Cephalalgia. 2001;21(3):207-215.
Visvanathan V, Kelly G. 12 minute consultation: an evidence-based management of referred otalgia. Clin Otolaryngol. 2010;35(5):409-414.
Joonpyo Hong, MD is a board-certified otolaryngologist practicing in Korea. This article reflects his clinical interpretation of published research and does not constitute individual medical advice.