
Your ears tend to hurt more when the plane is landing than when it takes off. That is not your imagination, and it is not random. The same asymmetry shows up underwater, where divers have a saying: descending is optional, but ascending is mandatory. Understanding why one direction is harder than the other is the key to preventing ear and sinus barotrauma — and to knowing which medication actually works, in which form, and when, across flying, hiking, and diving.
What Causes Ear and Sinus Barotrauma
Barotrauma is not caused by pressure itself. It is caused by a pressure difference across a closed space that cannot equalize fast enough.
The middle ear is a small air pocket behind the eardrum. Its only vent is the Eustachian tube, a narrow channel running to the back of the nose. The paranasal sinuses are air-filled cavities that drain through even narrower openings called ostia, with the frontal sinus connected by a particularly long, delicate duct. When outside pressure changes and these channels stay open, air flows in or out and everything stays balanced. When they are swollen shut — by a cold, allergic rhinitis, or sinus inflammation — pressure cannot equalize, the tissue gets pulled or squeezed, and you feel fullness, pain, and sometimes muffled hearing [Mirza, Otic barotrauma from air travel, 2005]. A severe sinus squeeze can also produce a nosebleed. In other words, barotrauma is really a plumbing problem: the trigger is the pressure change, but the cause is a blocked tube.
Why Descent Hurts More Than Ascent
Here is the part most explanations skip. The Eustachian tube behaves like a one-way flutter valve.
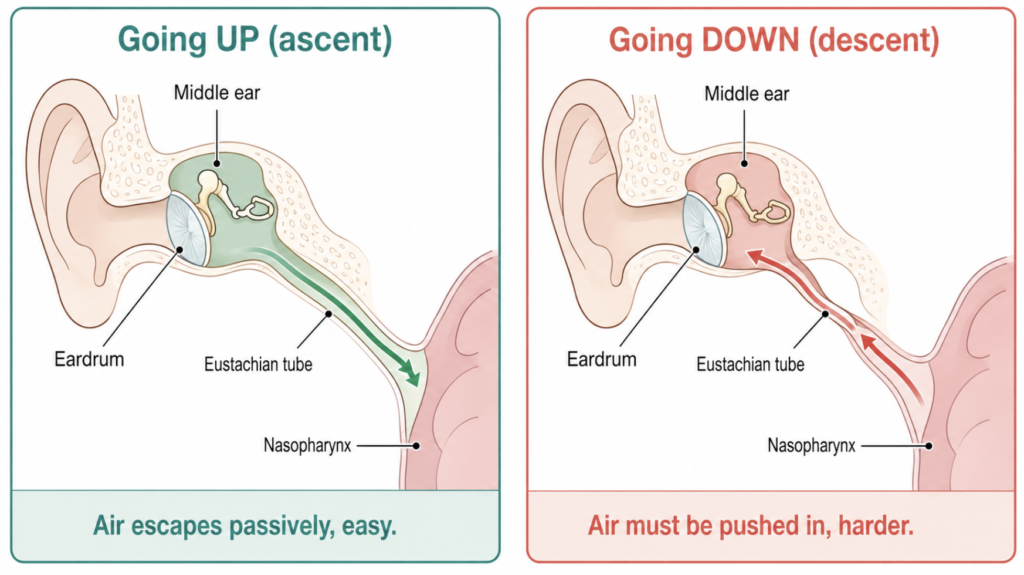
When you go up — a plane climbing, a diver rising toward the surface — the air trapped in your middle ear expands, pushes the valve open from the inside, and escapes on its own. This is mostly passive and rarely painful.
When you go down — a plane descending to land, a diver dropping below the surface — outside pressure rises, the middle ear becomes relatively low-pressure, and the eardrum is pushed inward while the Eustachian tube tends to collapse shut. Now you must actively force air back in against a closing valve, which is much harder [Mirza, Otic barotrauma from air travel, 2005]. That is why airplane ear is worst on landing, and why divers feel the squeeze on the way down.
| Activity | When it hurts most | What is happening |
|---|---|---|
| Flying | Landing (descent) | Cabin pressure rises; eardrum pushed inward |
| Scuba diving | Descent (squeeze) and ascent (reverse block) | Down = hard to equalize; up = trapped expanding air |
| Hiking / driving downhill | Descent | Same mechanism as a plane landing |
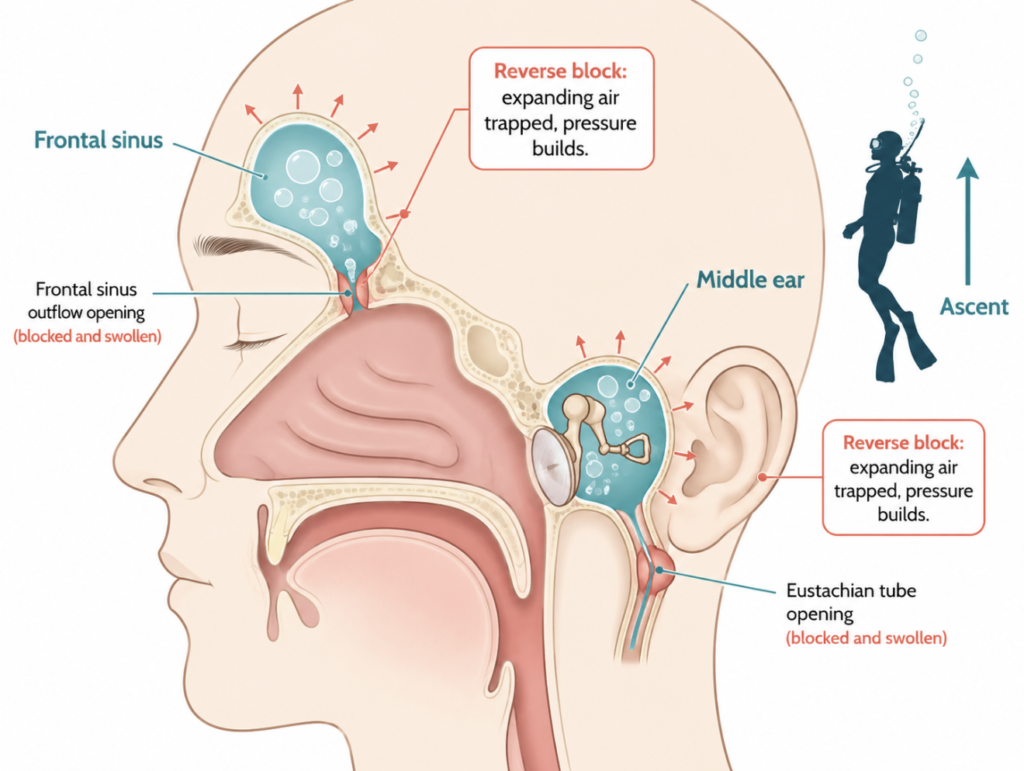
Diving adds a second danger on the way up. If a sinus or ear opening is blocked during ascent, the expanding air has nowhere to go and pressure builds against the sinus walls or the facial and trigeminal nerves — the “reverse block” [Massey, Neurology and diving, 2014]. Because a diver cannot simply stop and stay down, an ascent problem is far more serious than a descent problem.
What To Do — By Situation
The shared first step in every situation is active equalization: swallow, yawn, chew gum, or do a gentle Valsalva (pinch the nose and blow softly). On a plane, this matters most during descent — and it is worth staying awake for landing, since you cannot consciously clear your ears while asleep.
Flying
For flights, the evidence points clearly to an oral decongestant rather than a spray. In a randomized, double-blind trial, adults with a history of ear pain who took 120 mg of oral pseudoephedrine about 30 minutes before departure reported barotrauma 34% of the time, versus 71% in the placebo group — roughly halving the risk. An oxymetazoline nasal spray, by contrast, performed only slightly better than placebo for ear symptoms [Jones, A double-blind comparison between oral pseudoephedrine and topical oxymetazoline in the prevention of barotrauma during air travel, 1998]. A later review reached the same conclusion and noted that oral pseudoephedrine did not help in children [Mirza, Otic barotrauma from air travel, 2005].
If nasal congestion is the main problem, a nasal spray used shortly before takeoff and landing can still help the nose itself — it is simply less reliable for the ear. Oral decongestants are not for everyone: they are generally avoided in people with high blood pressure, heart rhythm disorders, or during pregnancy. This is exactly the kind of decision worth running past a clinician or pharmacist before you fly.
Hiking and Driving in the Mountains
Altitude changes here follow the same physics as a plane landing, but the pressure change is far more gradual. For most people, the equalization techniques above are enough, and routine medication is unnecessary. Pre-treatment is mainly worth considering if you already have a cold or active rhinitis.
Scuba Diving — Where the Rules Change
Diving is where the “just take a decongestant” reflex can backfire, and ENT reviews call the practice genuinely controversial [Mallen, SCUBA Medicine for otolaryngologists: Part I. Diving into SCUBA physiology and injury prevention, 2020]. The problem is timing. A decongestant can open your tubes enough to descend, but if it wears off underwater, congestion rebounds and traps expanding air on ascent — the reverse block. That is not merely painful: it can rupture an eardrum or injure the inner ear, and the panic it triggers at depth is itself a drowning risk. Short-acting sprays are especially prone to this rebound, and oral pseudoephedrine adds CNS stimulation that has no place at depth.
So reaching for a decongestant just to get down is strongly discouraged as a self-directed strategy. The rule diving physicians keep coming back to is simpler: if you need a drug to descend, sit the dive out. And never dive with an active cold or sinus infection — the biggest pressure gradients hit in the first few meters, so a tube that will not clear early is a signal to abort, not to medicate [Mallen, SCUBA Medicine for otolaryngologists: Part I. Diving into SCUBA physiology and injury prevention, 2020].
The Long-Term Fix: Treat the Inflammation, Not the Moment
None of the above helps the diver or frequent flyer whose tubes block again and again from ongoing nasal and sinus inflammation. This is where intranasal corticosteroid sprays differ from decongestants in a way that matters underwater: because they calm inflammation instead of constricting vessels, they cause no rebound swelling as they wear off — no reverse-block trap waiting at the end of a dive. The catch is that they work slowly and must be started well in advance, not minutes before descent. In a study of divers with chronic rhinosinusitis and recurrent sinus barotrauma, saline irrigation plus topical mometasone (with a short systemic steroid course) let most return to diving, with surgery reserved for those who did not improve [Skevas, Medical and surgical treatment in divers with chronic rhinosinusitis and paranasal sinus barotrauma, 2012]. For anyone with allergic rhinitis who flies or dives often, this baseline inflammation control — not a last-minute pill — is the safest long-term strategy, worked out with an ENT.
Clinical Perspective
The most common mistake is treating “flying” and “diving” as the same problem with one fix. They are not. On a flight, an oral decongestant taken ahead of time has the best evidence, and a mid-flight rebound is merely uncomfortable. Underwater, that same rebound can be dangerous, so the safest move is often to not dive until the congestion clears. Any episode with hearing loss, lasting vertigo, or an ear that “popped” and stayed wrong deserves an ENT evaluation rather than another dose.
Key Takeaways
- Barotrauma is a blocked-tube problem, not a pressure problem — the Eustachian tube or sinus opening fails to equalize.
- Descent is harder than ascent because air must be actively forced into a closing valve, which is why plane landings and dive descents hurt most.
- For flying, oral pseudoephedrine taken before departure has good trial evidence; an oxymetazoline nasal spray works little better than placebo for the ear.
- For diving, using a decongestant just to get down is strongly discouraged — if a drug is what makes the dive possible, the safer choice is to skip it, and never dive with an active cold.
- For recurrent problems, an intranasal steroid spray controls inflammation without rebound congestion and is the safest long-term option, but it must be started in advance under medical guidance.
FAQ
Does airplane ear hurt more on takeoff or landing? Landing. As the plane descends, cabin pressure rises and pushes the eardrum inward, and the Eustachian tube resists letting air back in. Takeoff is usually easier because expanding middle-ear air escapes on its own.
Should I take a pill or use a nasal spray? For flights, oral decongestants have the stronger evidence for preventing ear pain. Nasal sprays are more useful for nasal congestion itself and for sinus issues, but are less reliable for the ear.
Can I take a decongestant before scuba diving? This is strongly discouraged as a do-it-yourself fix. The drug can wear off underwater and cause a dangerous reverse block on ascent, so if you feel you need one to descend, the safer decision is to postpone the dive — and never dive with an active cold or congested sinuses.
When should I take a decongestant for a flight? If you and your doctor have agreed an oral decongestant is appropriate, research suggests it works best taken about 30 to 60 minutes before departure rather than after symptoms start. But the right drug and timing depend on your health — decongestants can be risky with high blood pressure or heart conditions — so confirm the plan with your doctor or pharmacist before traveling instead of buying one over the counter on your own.
References
- Jones JS, Sheffield W, White LJ, Bloom MA. A double-blind comparison between oral pseudoephedrine and topical oxymetazoline in the prevention of barotrauma during air travel. Am J Emerg Med. 1998;16(3):262-264.
- Mirza S, Richardson H. Otic barotrauma from air travel. J Laryngol Otol. 2005;119(5):366-370.
- Mallen JR, Roberts DS. SCUBA Medicine for otolaryngologists: Part I. Diving into SCUBA physiology and injury prevention. Laryngoscope. 2020;130(1):52-58.
- Massey EW, Moon RE. Neurology and diving. Handb Clin Neurol. 2014;120:959-969.
- Skevas T, Baumann I, Bruckner T, Clifton N, Plinkert PK, Klingmann C. Medical and surgical treatment in divers with chronic rhinosinusitis and paranasal sinus barotrauma. Eur Arch Otorhinolaryngol. 2012;269(3):853-860.
Joonpyo Hong, MD is a board-certified otolaryngologist practicing in Korea. This article reflects his clinical interpretation of published research and does not constitute individual medical advice.