Roughly 80% of adults have some misalignment of the nasal septum, and most never know it. When researchers apply stricter, measurable thresholds, the prevalence of clinically defined deviation drops to between 18% and 65% of the population [Kazimierczak, Correlation Analysis of Nasal Septum Deviation and Results of AI-Driven Automated 3D Cephalometric Analysis, 2023]. The clinical question has never been “is it deviated?” — it is almost always “how much does it matter, and how confident can we be in the measurement?” In 2026, that second question finally has a new tool behind it: deep-learning models that can read the same CT scan an ENT looks at and contribute a more consistent answer.
This article walks through how a deviated septum is actually diagnosed today, where AI fits in, and what a patient should know before agreeing to imaging or surgery.
What a Deviated Septum Actually Is
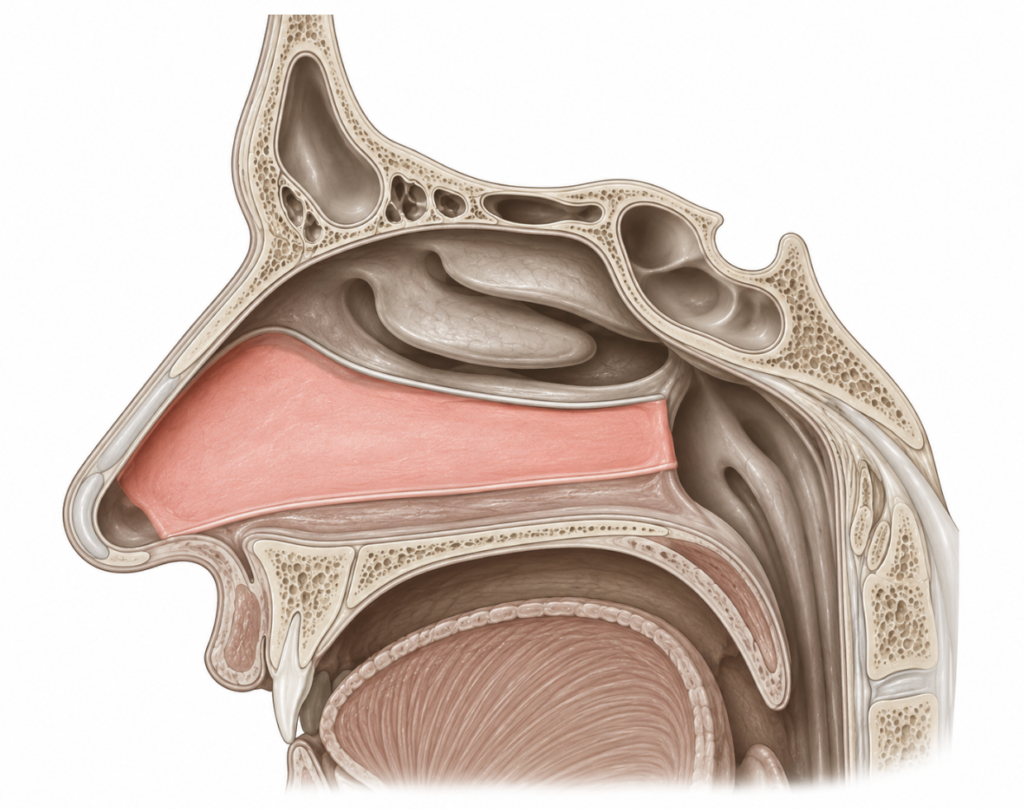
The nasal septum is the wall of cartilage and bone that divides the nasal cavity into a left and a right airway. When it bends, twists, or carries a bony spur, one side becomes narrower than the other. That narrowing can cause nasal obstruction, recurrent sinus infections, nosebleeds, headaches over the spur, and disrupted sleep — but only sometimes. A “deviated septum” on imaging is not, by itself, a diagnosis. It becomes one only when the structural finding lines up with the patient’s symptoms.
That mismatch — anatomy versus symptoms — is the reason diagnosis is more nuanced than it sounds.
How ENT Doctors Diagnose It Today
The pathway has three layers, and most patients only need the first two.
1. History and symptom pattern
The first useful data point is not an image. Unilateral nasal obstruction that does not switch sides, obstruction worse on one side at night, a history of nasal trauma, or chronic mouth breathing all push the probability up. Bilateral congestion that alternates is more often turbinate hypertrophy or rhinitis than a septal problem.
2. Anterior rhinoscopy and nasal endoscopy
A speculum exam shows the anterior septum. An endoscope — a thin rigid or flexible camera — visualizes the entire septum from the nostril to the nasopharynx, including posterior spurs that rhinoscopy misses. For most patients with classic symptoms, endoscopy is enough to confirm the diagnosis and plan treatment.
3. CT or CBCT imaging — when it is actually needed
Imaging is reserved for cases where surgery is being planned, where chronic sinusitis is suspected, where trauma has reshaped the bony framework, or where an insurer requires objective confirmation. Coronal CT or cone-beam CT (CBCT) shows the full three-dimensional geometry of the septum, the turbinates, and the paranasal sinuses.
Worth noting: imaging is not a great predictor of symptom severity on its own. A 2021 study of 225 patients found that CT morphology and the angle of septal deviation did not predict NOSE symptom scores, and the authors concluded that requesting a CT scan purely to confirm obstruction is not justified [Janovic, Is Computed Tomography Imaging of Deviated Nasal Septum Justified for Obstruction Confirmation?, 2021]. The takeaway: the CT helps the surgeon plan, but it does not tell you whether the patient is actually obstructed. The patient does.
The Septal Deviation Angle: The Number Behind the Diagnosis
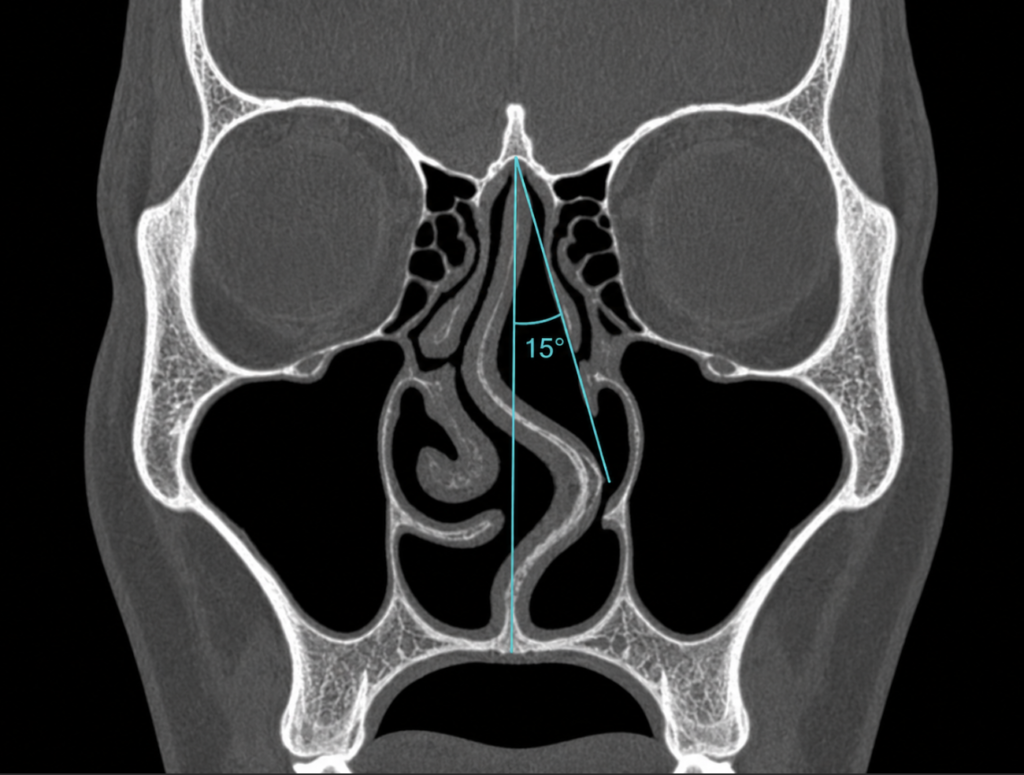
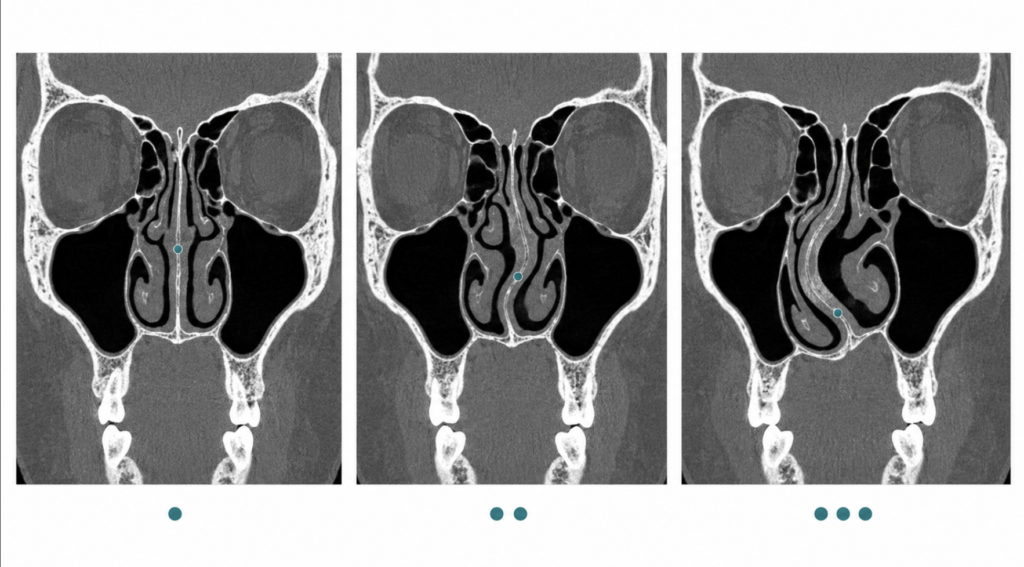
When clinicians or researchers want a single number to describe how crooked a septum is, they use the septal deviation angle (SDA). Measured on a coronal CT slice, it is the angle between a vertical reference line (typically from the crista galli) and the line drawn to the most laterally deviated point of the septum. Researchers commonly group deviations into mild, moderate, and severe categories based on this angle, though the exact cutoffs vary across studies.
Two ENTs can look at the same CT and report SDAs that differ by several degrees. That interrater variability is precisely the gap that imaging AI is built to close.
Where AI Is Changing Diagnosis in 2026
Three things are happening in parallel.
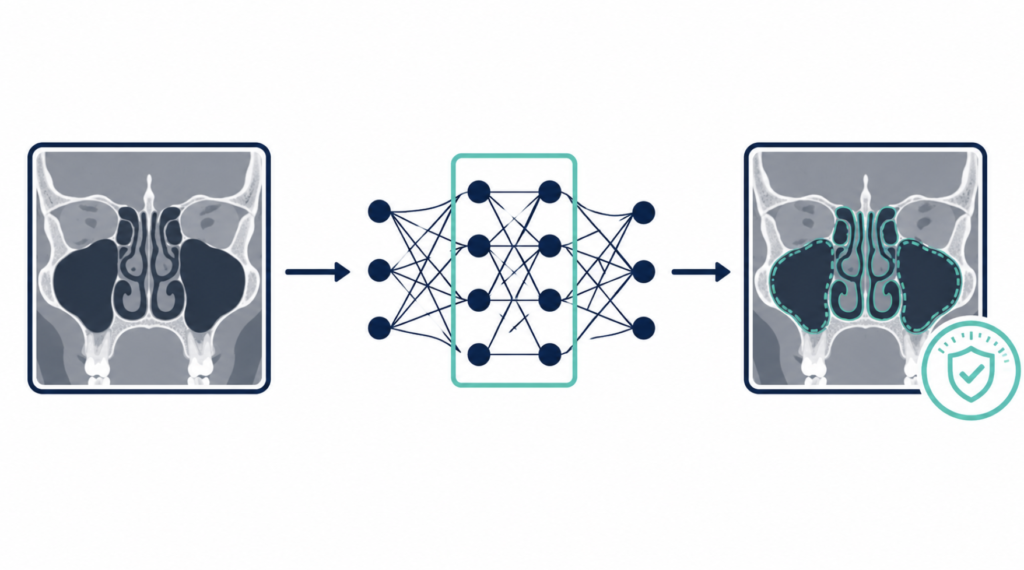
Automated detection on CBCT. A 2024 proof-of-concept study trained Mask R-CNN models — a family of object-detection neural networks — on 204 coronal CBCT images. The best-performing model reached a mean average precision of 0.911 and an area under the curve of 0.921 for detecting whether a nasal septum was deviated [Shetty, The Application of Mask Region-Based Convolutional Neural Networks in the Detection of Nasal Septal Deviation Using Cone Beam Computed Tomography Images, 2024]. In plain language: the AI agreed with two maxillofacial radiologists more than 90% of the time on a binary “deviated or not” call.
Lighter, faster pipelines with measurable clinical impact. A 2026 multicenter study trained a two-stage AI pipeline on 330 CBCT scans: YOLOv11 to locate the nasal septum region within each image, then a lightweight MobileNet classifier to label it as deviated or non-deviated. The classifier itself reached an area under the curve of 0.817 — solid but not extraordinary. The more interesting finding came when orthodontists used the tool on the validation set: diagnostic accuracy improved by roughly 20%, and average diagnosis time fell by about 24 seconds per case, a 54% efficiency gain [Zhai, Automated assessment of nasal septum deviation using cone-beam computed tomography images based on artificial intelligence, 2026]. That is the more useful framing for clinical AI in 2026: not “the model is better than the doctor,” but “the doctor with the model is faster and more consistent than the doctor without it.”
Integration into orthodontic and craniofacial workflows. AI cephalometric platforms now flag septal deviation as part of broader 3D craniofacial analyses. A 2023 J Clin Med study using the CephX AI platform on 90 post-traumatic patients reported good-to-excellent agreement between repeated AI measurements and manual ones for most cephalometric parameters, with the septal deviation angle showing a weak but statistically significant correlation with the hinge axis angle [Kazimierczak, Correlation Analysis of Nasal Septum Deviation and Results of AI-Driven Automated 3D Cephalometric Analysis, 2023]. The clinical value is less in the correlation itself than in what it shows about AI: software is now reliable enough to add septal measurements to the standard cephalometric report without slowing the radiologist down.
What none of these tools do — and this is the part the headlines tend to skip — is decide whether the patient needs surgery.
Clinical Perspective
Three observations from the clinic.
First, the exam still leads. AI on a CT is most useful when the imaging is already indicated for another reason, such as sinus disease or pre-surgical planning. Ordering a CT just to run AI on it inverts the logic of when imaging is appropriate.
Second, where AI genuinely helps is consistency. Two surgeons measuring the same septum can disagree by five degrees. A validated model gives the same answer every time, which matters when a clinic is tracking outcomes across hundreds of septoplasties or comparing pre- and post-operative anatomy.
Third, patients should be a little skeptical of any consumer app claiming to diagnose a deviated septum from a selfie or a question form. The published models work on cross-sectional imaging — CT or CBCT — not facial photography. The external nose and the septum behind it are two different structures: a tent’s outer fabric can sit perfectly straight while the pole inside leans, and the reverse is just as common.
Can You Self-Diagnose a Deviated Septum?
A reasonable home screen: close one nostril, breathe in, then switch. If one side is consistently and substantially harder to breathe through, and the asymmetry does not flip from morning to evening, a deviated septum is more likely than alternating turbinate swelling. That alone is enough to warrant an ENT visit, but it is not a diagnosis. The structural piece can only be confirmed on endoscopy or imaging.
Key Takeaways
- A deviated septum is diagnosed clinically; imaging confirms severity, not the diagnosis itself.
- CT or CBCT is needed only when surgery, sinusitis, or trauma is in play — not to prove a patient is obstructed.
- AI models published in 2024 detect deviated nasal septum on CBCT with over 90% accuracy and are beginning to automate measurement of the septal deviation angle.
- AI improves consistency of measurement; it does not change the indication for surgery.
- Photo-based or app-based “diagnosis” of a deviated septum is not supported by current evidence.
FAQ
Do I need a CT scan to diagnose a deviated septum? Usually not. Most diagnoses are made with history and nasal endoscopy. CT is added when the surgeon needs to see the bony anatomy before septoplasty, when sinusitis is suspected, or after nasal trauma.
Can ChatGPT or an AI app tell if I have a deviated septum from a photo? No. Published deep-learning models for septal deviation work on coronal CT or cone-beam CT — not on external facial photographs. The visible nose and the septum inside it are different structures, and an asymmetric external nose does not reliably indicate septal deviation.
How accurate is AI at reading nasal CT scans? On 2024 benchmarks, AI models reach roughly 90% accuracy for detecting whether a septum is deviated on CBCT and approach expert-level accuracy for measuring the deviation angle. Accuracy is highest for clear-cut cases and lower for borderline or atypical anatomy.
Will insurance cover a CT for a deviated septum? Coverage depends on the payer and the country, but most insurers require either documented surgical planning, suspected sinus disease, or trauma. Imaging purely to “confirm” symptomatic obstruction is often not reimbursed and is not strongly supported by evidence.
References
- Kazimierczak N, Kazimierczak W, Serafin Z, Nowicki P, Lemanowicz A, Nadolska K, Janiszewska-Olszowska J. Correlation Analysis of Nasal Septum Deviation and Results of AI-Driven Automated 3D Cephalometric Analysis. J Clin Med. 2023 Oct 19;12(20):6621.
- Janovic N, Janovic A, Milicic B, Djuric M. Is Computed Tomography Imaging of Deviated Nasal Septum Justified for Obstruction Confirmation? Ear Nose Throat J. 2021 Feb;100(2):NP100-NP105.
- Shetty S, Mubarak AS, David LR, Al Jouhari MO, Talaat W, Al-Rawi N, AlKawas S, Shetty S, Ozsahin DU. The Application of Mask Region-Based Convolutional Neural Networks in the Detection of Nasal Septal Deviation Using Cone Beam Computed Tomography Images: Proof-of-Concept Study. JMIR Form Res. 2024 Sep 3;8:e57335.
- Zhai Q, Cui M, Fu Y, Huang X, Wang Z, Wu Q, Cong N, Liu C. Automated assessment of nasal septum deviation using cone-beam computed tomography images based on artificial intelligence: Development and multicenter validation. Am J Orthod Dentofacial Orthop. 2026 Jan;169(1):56-66.e2.
Joonpyo Hong, MD is a board-certified otolaryngologist practicing in Korea. This article reflects his clinical interpretation of published research and does not constitute individual medical advice.