
Picture a scene that plays out often in ENT clinics. An 80-year-old comes in for dizziness that began a few weeks earlier; her hearing test is reasonable, her balance exam is unremarkable, and her brain scan is clean. The likeliest cause is sitting in the bag of pill bottles on the desk: she takes eleven medications, and at least three of them can make a person dizzy. She is one small example of a much larger pattern, because medications that cause dizziness in older adults are common — and they rarely act alone.
This is one of the most under-recognized patterns in the care of older adults — the very symptom that sends someone to an ear, nose, and throat doctor is often a side effect of the medications they already take. A pharmacovigilance analysis of the U.S. Food and Drug Administration’s adverse event database identified roughly 1,300 different drugs reported in connection with hearing impairment alone [Wu, Drug-induced hearing loss: a real-world pharmacovigilance study using the FDA adverse event reporting system database, 2025]. This guide maps the common ENT complaints — dizziness, ringing ears, hearing loss, nosebleeds, cough, dry mouth, taste changes, and more — to the drugs most often behind them, and explains why the risk climbs with every pill added.
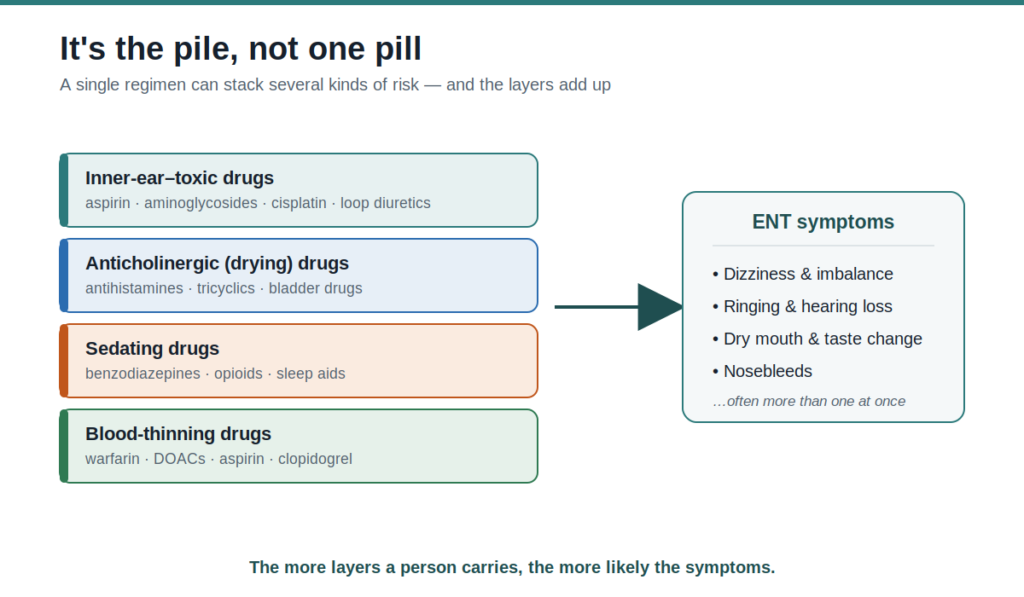
It’s the pile, not one pill
The key idea is not “drug X causes symptom Y.” It is that effects accumulate. A single regimen can carry a layer of drugs that are toxic to the inner ear, a layer that dries out the mouth and nose, a layer that sedates or lowers blood pressure, and a layer that thins the blood — and each layer raises the odds of a different ENT symptom. The problem is rarely one offending pill; it is the combined burden.
Older adults are especially vulnerable because the kidneys and liver clear drugs more slowly with age, so medicines and their active byproducts linger and build up. A dose that was harmless at 50 can reach a higher effective level at 80, even when nothing about the prescription has changed.
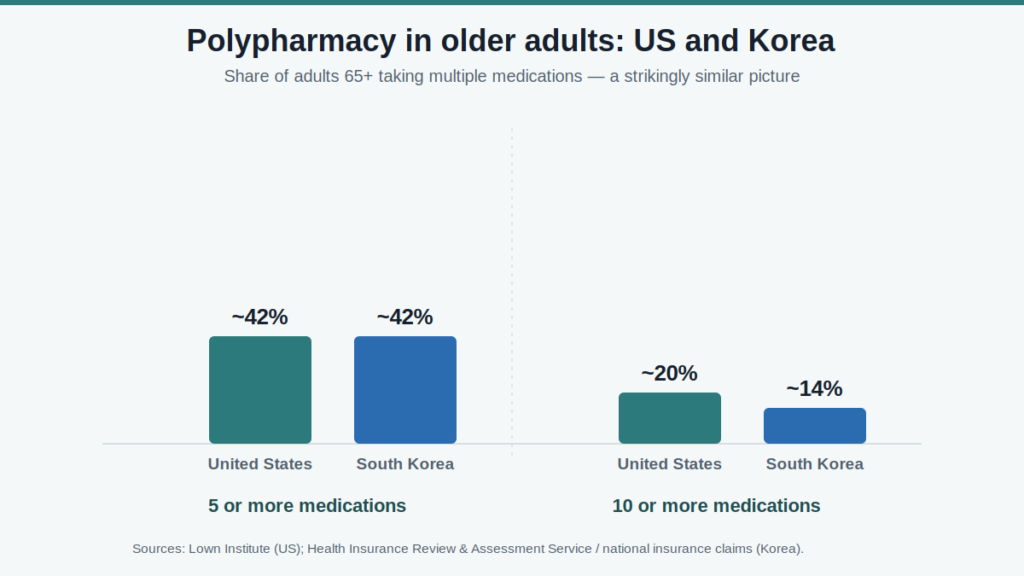
Polypharmacy — commonly defined as taking five or more medications — is common in older adults and is linked to adverse drug events, falls, hospitalizations, and higher mortality [Hung, Deprescribing in older adults with polypharmacy, 2024]. The Lown Institute, a U.S. health-policy think tank, estimates that more than four in ten Americans over 65 take five or more prescription drugs and that nearly one in five take ten or more.
Korea looks much the same: in national health-insurance data, roughly four in ten adults aged 65 and older took five or more medications, while the share taking ten or more climbed to about one in seven over the past decade [Cho, Aging and the Prevalence of Polypharmacy and Hyper-Polypharmacy Among Older Adults in South Korea: A National Retrospective Study During 2010-2019, 2022].
One rule belongs before the table and applies to everything below it: never stop a prescribed medication on your own. The goal of this article is to help you recognize a pattern and raise the right question with your prescriber — not to change a regimen yourself.
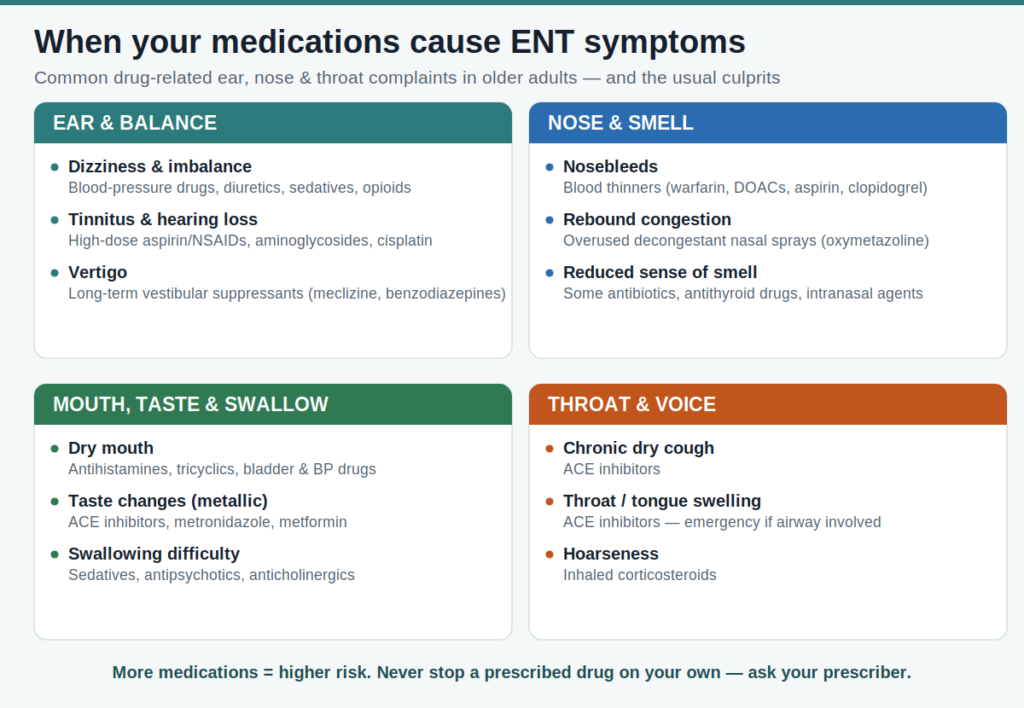
Medications that cause dizziness and other ENT symptoms: The master table
The table below pairs common ear, nose, and throat symptoms with the drug classes most often responsible, the mechanism behind each, and whether the effect typically reverses. It synthesizes the cited literature and standard clinical pharmacology. Reversibility is a general guide, not a promise for any individual.
Ear and balance
| Symptom | Common culprits (class — example) | Why it happens | Reversibility |
|---|---|---|---|
| Dizziness, lightheadedness, imbalance | Blood-pressure drugs and diuretics (alpha-blockers, furosemide, nitrates); benzodiazepines (lorazepam); opioids; sleep aids (zolpidem); some antidepressants (tricyclics, SSRIs); some antiepileptics | Orthostatic blood-pressure drop; sedation of the brain; combined anticholinergic and sedative burden | Usually reversible after a dose change or switch |
| Vertigo (a spinning sensation) | Aminoglycoside antibiotics (gentamicin); high-dose loop diuretics; long-term vestibular suppressants (paradoxically) | Direct toxicity to the balance organ; suppressants block the brain’s natural compensation | Aminoglycoside damage is often permanent; the suppressant effect reverses, but these should not be used beyond 2–3 weeks |
| Tinnitus (ringing) | High-dose aspirin and other NSAIDs; loop diuretics; aminoglycosides; cisplatin; quinine; some antibiotics | Toxic effects on the cochlea | Aspirin, NSAID, and loop-diuretic effects are usually reversible; aminoglycoside and cisplatin effects are often permanent |
| Hearing loss (sensorineural) | Aminoglycosides; cisplatin and carboplatin; high-dose loop diuretics; high-dose salicylates; macrolide antibiotics | Damage to cochlear hair cells and the stria vascularis | Platinum and aminoglycoside loss is often permanent; salicylate and diuretic effects usually reverse |
Nose and smell
| Symptom | Common culprits (class — example) | Why it happens | Reversibility |
|---|---|---|---|
| Nosebleeds (epistaxis) | Anticoagulants (warfarin, direct oral anticoagulants); antiplatelets (aspirin, clopidogrel); intranasal steroid sprays; overused decongestant sprays | Impaired clotting; thinning and irritation of the nasal lining | Resolves once bleeding is controlled; the blood thinner itself is usually still needed |
| Rebound congestion (rhinitis medicamentosa) | Decongestant nasal sprays (oxymetazoline) used beyond three to five days | Rebound swelling as the medication wears off | Reversible, but only after the spray is stopped |
| Reduced sense of smell | Some antibiotics; antithyroid drugs; intranasal agents | Varied effects on smell receptors and nerves | Variable; some cases reverse after a change |
| Nasal dryness and crusting | Anticholinergics; antihistamines; ipratropium | Reduced nasal secretions | Reversible |
Mouth, taste, and swallowing
| Symptom | Common culprits (class — example) | Why it happens | Reversibility |
|---|---|---|---|
| Dry mouth (xerostomia) | First-generation antihistamines; tricyclic antidepressants; bladder antimuscarinics; some antipsychotics and blood-pressure drugs; diuretics; opioids | Reduced saliva from anticholinergic action | Usually reversible after a change |
| Taste change (a metallic or blunted taste) | ACE inhibitors (classic); metronidazole; clarithromycin; metformin; antithyroid drugs; some chemotherapy | Altered taste signaling and zinc effects | Often reversible |
| Swallowing difficulty (dysphagia) | Benzodiazepines and other sedatives; antipsychotics (drug-induced movement effects); anticholinergics (through dry mouth); bisphosphonates (irritation of the esophagus) | Sedation, movement effects, dryness, or local injury | Often reversible after a change; needs prompt review because of the aspiration risk |
| Gum overgrowth (gingival hyperplasia) | Calcium channel blockers (amlodipine, nifedipine); phenytoin; cyclosporine | Overgrowth of gum tissue | Partly reversible after a drug change |
| Oral thrush (candidiasis) | Inhaled corticosteroids used without rinsing; broad-spectrum antibiotics; dry mouth | A local shift in immunity and normal flora | Treatable, and largely preventable with inhaler technique |
Throat and voice
| Symptom | Common culprits (class — example) | Why it happens | Reversibility |
|---|---|---|---|
| Chronic dry cough | ACE inhibitors (very common) | Build-up of bradykinin | Reversible after the drug class is changed |
| Throat, tongue, or facial swelling (angioedema) | ACE inhibitors (can begin months or years into treatment); rarely ARBs | Bradykinin-mediated swelling | A medical emergency if the airway is involved; the drug is stopped permanently |
| Hoarseness | Inhaled corticosteroids (deposited on the vocal folds); anticholinergic dryness | Local effect on the larynx and dryness | Reversible with inhaler technique |
A note on evidence. The links above span a wide range of certainty. Some are well-established, mechanism-based effects — ACE inhibitors causing cough through bradykinin, or aminoglycosides damaging the cochlea. Others, such as tinnitus or smell loss attributed to common cardiovascular drugs, appear in adverse-event reporting but are not firmly causal. A drug class listed for a symptom means the association is recognized, not that the drug is the proven cause in any one person.
Practical steps by symptom. A few measures are reasonable for anyone while the cause is sorted out. For dizziness, stand up slowly, especially when rising from lying or sitting. For nosebleeds, pinch the soft part of the nose and lean forward, and keep the nasal lining moist. For inhaler-related thrush or hoarseness, use a spacer and rinse the mouth after each dose. For any of these, note when the symptom started relative to a new drug or dose change, raise it with the prescriber, and never stop a medication without guidance.
Spotlight 1 — Dizziness and imbalance
Dizziness is the most common drug-related ENT complaint in older adults, and the two biggest contributors are cardiovascular and central nervous system drugs [Shoair, Medication-related dizziness in the older adult, 2011]. Blood-pressure medicines and diuretics can drop the pressure too far when a person stands; sedatives, opioids, and some antidepressants dull the brain’s balance processing. Add an anticholinergic on top, and the effects compound.
The scale of this is easy to underestimate. In a study of more than 15,000 older adults with dementia, 82 percent were taking at least one medication that lists dizziness as a side effect, and for each additional such drug the risk of emergency hospitalization rose by about four percent [Sondh, Medications associated with dizziness or hypotension and adverse outcomes: an electronic health record study in older adults with dementia, 2025].
The burden also worsens the very condition a patient may be seeking help for: among older people who already had vertigo, dizziness, or balance disorders, a higher anticholinergic and sedative load predicted poorer day-to-day and balance-specific functioning over time [Katzenberger, Exposure to anticholinergic and sedative medication is associated with impaired functioning in older people with vertigo, dizziness and balance disorders—Results from the longitudinal multicenter study MobilE-TRA, 2023].
There is a trap specific to ENT care worth naming. Medications such as meclizine and benzodiazepines quiet acute vertigo, but taken beyond about two to three weeks they block the brain’s natural rebalancing — a process called central compensation — and can turn a short-lived spinning spell into chronic dizziness. For that reason, long-term use of these suppressants is generally avoided.
Standard fall-risk checklists make the problem harder to see, because they often leave medications out: in one analysis of older patients who had fallen, nearly half of the active drug ingredients they were taking qualified as high fall-risk agents, most acting on the nervous or cardiovascular systems [Michalcova, Inclusion of medication-related fall risk in fall risk assessment tool in geriatric care units, 2020].
Spotlight 2 — The ears: ringing and hearing loss
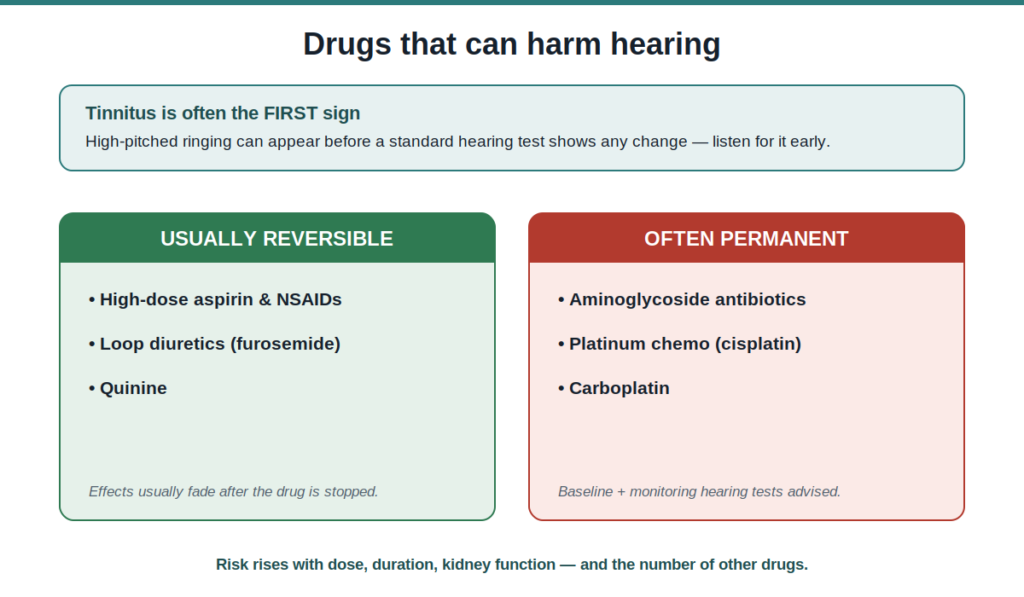
Most people know a few “classic” ototoxic drugs — aminoglycoside antibiotics, the chemotherapy agent cisplatin, high-dose loop diuretics, and high-dose aspirin. The surprise is the long tail. The FDA adverse-event analysis flagged about 1,300 drugs in reports of hearing impairment and found positive risk signals for several hundred of them, including some of the most ordinary medicines in an older adult’s cabinet [Wu, Drug-induced hearing loss: a real-world pharmacovigilance study using the FDA adverse event reporting system database, 2025]. A caution about that data: a drug appearing often in reports partly reflects how commonly it is used, so frequency is not the same as proven cause. Still, the breadth is the point — ototoxicity is not a rare-drug problem.
The consequences are not trivial. Hospital-prescribed ototoxic medications are estimated to cause acquired hearing loss in as many as a million people each year across Western Europe and North America, and there is still no approved drug to prevent the permanent damage caused by platinum chemotherapy or aminoglycoside antibiotics [Steyger, Mechanisms of aminoglycoside- and cisplatin-induced ototoxicity, 2021]. Whether the damage reverses depends on the drug: aspirin, NSAID, and loop-diuretic effects usually fade after stopping, while aminoglycoside and cisplatin injury is frequently permanent.
Clinical Perspective. New ringing in the ears deserves attention rather than dismissal. High-pitched tinnitus in particular often appears before any change shows up on a standard hearing test, because ototoxic injury typically begins in the high-frequency base of the cochlea. The precaution that matters most is reserved for the highest-risk treatments: for patients starting platinum-based chemotherapy (cisplatin) or a prolonged course of aminoglycoside antibiotics, a baseline hearing test followed by monitoring can catch a change while it can still be acted on. This is not something that applies to ordinary blood-pressure pills or diuretics.
Spotlight 3 — The cardiovascular drugs: one class, several ENT symptoms
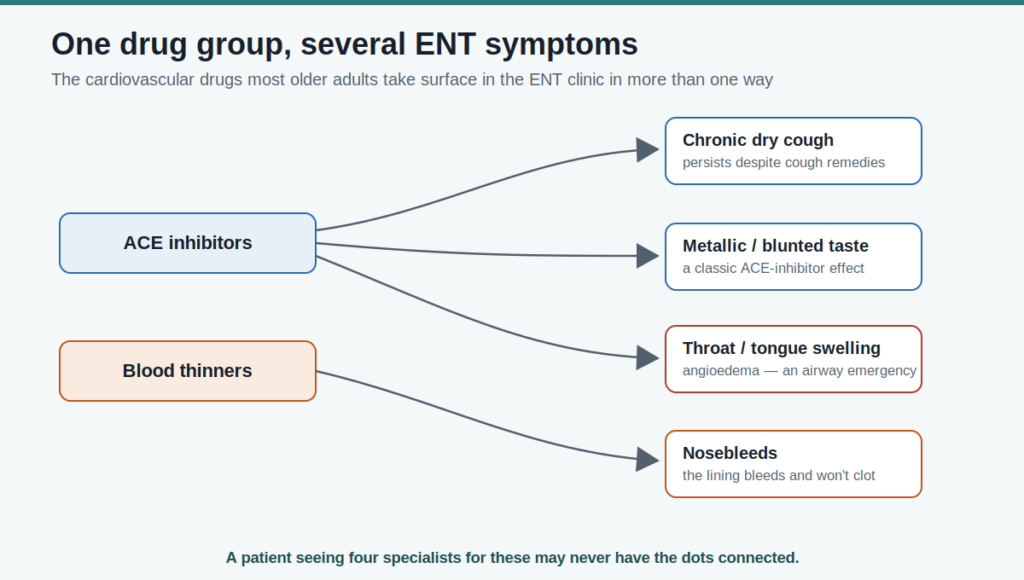
The medicines most older adults are on — blood thinners and blood-pressure drugs — show up in the ENT clinic in more than one way at once, which makes them a good illustration of the cumulative-burden idea.
Anticoagulants and antiplatelet agents are a leading reason for recurrent nosebleeds, because the nasal lining is thin and easily disturbed and these drugs remove the body’s usual ability to stop the bleeding quickly.
ACE inhibitors, among the most prescribed blood-pressure drugs, are a classic cause of a persistent dry cough that often lands in an ENT or pulmonary office after months of fruitless cough remedies; the same class can cause angioedema, a swelling of the lips, tongue, or throat that may begin long after the drug was started and becomes an airway emergency if it involves the throat. ACE inhibitors are also a well-known cause of a metallic or blunted sense of taste. One drug class, four distinct ENT presentations — and a patient seeing four different specialists for them may never have the dots connected.
The anticholinergic burden: dry mouth and what it drags with it
Dry mouth is so common in older adults that it is easy to dismiss as simple aging. It usually is not. The leading cause of dry mouth, in older adults and the general population alike, is medication — mostly through anticholinergic effects — and polypharmacy itself contributes [Hayslett, Management of dry mouth, 2025]. The usual suspects include first-generation antihistamines, tricyclic antidepressants, bladder antimuscarinics, and several heart and blood-pressure drugs.
Dry mouth is not just uncomfortable. Reduced saliva accelerates tooth decay and gum disease, dulls taste, and makes swallowing harder — a meaningful problem when swallowing safety already declines with age. Because so many of these effects surface in the mouth, a medication review belongs in the dental chair, not only the primary care office [Soto, Oral implications of polypharmacy in older adults, 2023] — and, since the same regimens drive ear, nose, and throat symptoms, in the ENT clinic too.
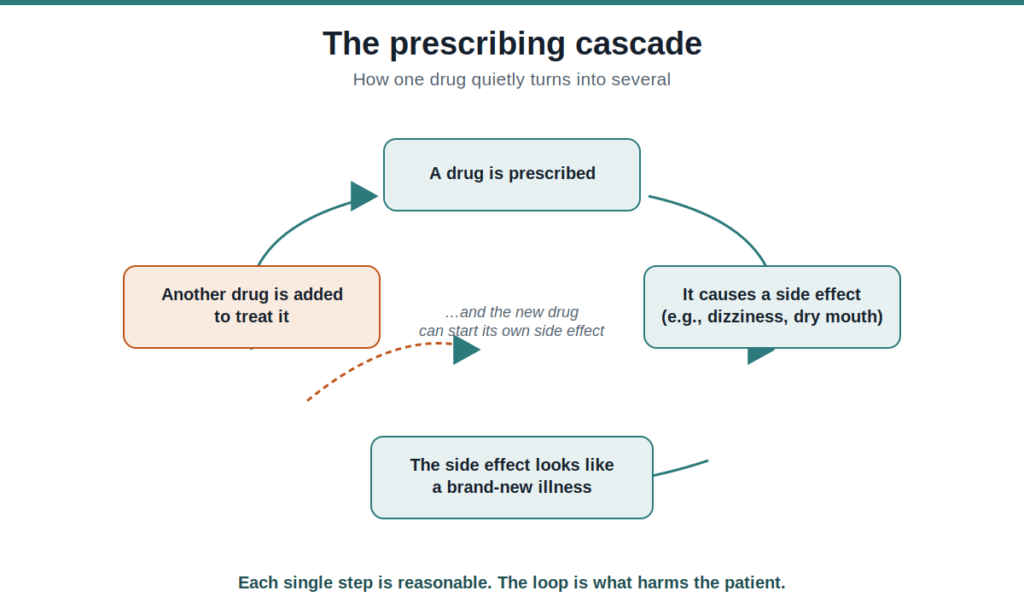
Why more drugs mean more symptoms: the prescribing cascade
Here is the mechanism that ties all of this together. Each specialist prescribes correctly for the organ in front of them — the cardiologist for the heart, the urologist for the bladder, the psychiatrist for mood. No single prescription is wrong. But no one sees the whole list, and a side effect of one drug gets read as a new disease, which earns another drug. This is the prescribing cascade, and it is especially common in older adults, where drug side effects masquerade as new “geriatric syndromes” such as falls, dizziness, and incontinence [O’Mahony, Prescribing cascades: we see only what we look for, we look for only what we know, 2022].
A structural reason this persists is that most medicines taken by multimorbid older patients are started and continued by clinicians without specialist geriatric training, who may not recognize drug-induced harm when it appears [O’Mahony, Prescribing cascades: we see only what we look for, we look for only what we know, 2022]. Modern medicine is built on single-disease guidelines that are good at telling doctors when to start a drug and largely silent on when to stop one. The result is accumulation by default.
ENT’s own prescriptions
It would be incomplete to point only at other specialties. Several drugs that ENT clinicians reach for in older adults carry the same risks discussed above: long-term vestibular suppressants, sedating first-generation antihistamines for allergy or vertigo, and anticholinergic decongestants. Many of these appear on explicit lists of potentially inappropriate medications for older adults, such as the STOPP criteria, which were expanded in their latest version to nearly 200 prescribing rules [O’Mahony, STOPP/START criteria for potentially inappropriate prescribing in older people: version 3, 2023]. The honest framing is that ENT is both a contributor to the burden and the natural place to catch it.
Clinical Perspective. A new ear, nose, or throat symptom in an older adult deserves a medication review as part of the workup, not only an organ-specific test. The most practical tool costs nothing: ask the patient to bring every pill, including over-the-counter products and supplements, and check whether the symptom began within days or weeks of a new prescription or a dose change. That single timeline question resolves a surprising number of cases.
What’s being done — and what you can do
The medical response to this problem has a name: deprescribing, the planned reduction or stopping of drugs that are no longer doing more good than harm. The evidence is encouraging but honest about its limits. Pooled trials show deprescribing reliably reduces inappropriate medications, prescribing omissions, and adverse drug reactions, and improves how consistently patients take what remains [Zhou, Deprescribing interventions for older patients: a systematic review and meta-analysis, 2023].
The average reduction per person can be modest [Linsky, Deprescribing in community-dwelling older adults: a systematic review and meta-analysis, 2025], and clear gains in hard outcomes such as hospitalization and survival have not been consistently demonstrated [Hung, Deprescribing in older adults with polypharmacy, 2024]. Deprescribing is real and worthwhile, but it is not yet a solved problem, and it works only when done deliberately with the prescriber.
For an older adult or a caregiver, a few habits make the biggest difference.
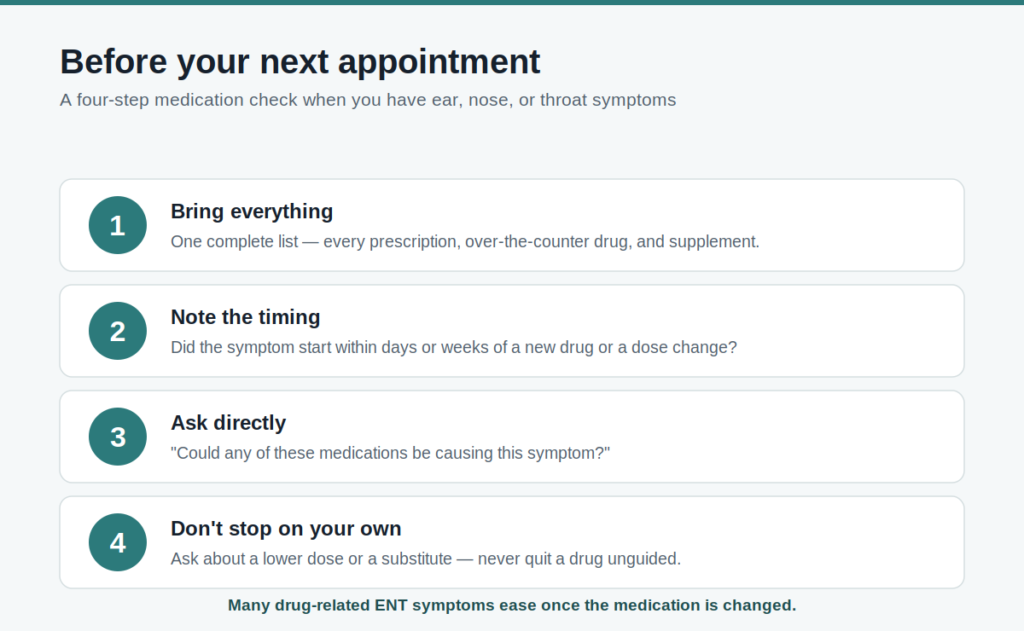
Keep one complete, current list of every medication, including over-the-counter drugs and supplements, and bring it to every appointment. When a new ENT symptom appears, ask directly whether any current drug could be the cause, and note whether the symptom started near a new prescription. Request a medication review from a pharmacist or primary care team, which is often available at no cost. And never stop a medication on your own — ask instead about a lower dose or a different option.
Key Takeaways
- Dizziness, ringing or hearing loss, nosebleeds, cough, and dry mouth are among the most common reasons older adults see an ENT — and all of them can be medication side effects.
- The risk rises with the number and combination of drugs, through a cumulative load of inner-ear-toxic, anticholinergic, sedative, and blood-thinning effects, rather than from one “bad” pill.
- New tinnitus is often the first sign that a medication is affecting the ears, appearing before measurable hearing loss.
- Medication is the leading cause of dry mouth in older adults, which in turn worsens taste, dental health, and swallowing.
- Many drug-induced ENT symptoms reverse when the medication is changed — but a medication should never be stopped without a prescriber’s guidance.
Frequently Asked Questions
Can medications cause dizziness and ringing in the ears at the same time? Yes. Some drugs affect both balance and the inner ear, and an older adult on several medications may be carrying more than one such effect at once. High-dose aspirin and loop diuretics, for example, can produce both tinnitus and unsteadiness, while blood-pressure drugs add lightheadedness from low pressure. Because the effects stack, the combination matters more than any single drug. If both symptoms appeared around the same time as a new prescription, that timing is worth raising with your prescriber.
Can blood thinners cause nosebleeds? Yes, frequently. Anticoagulants such as warfarin and direct oral anticoagulants, and antiplatelet drugs such as aspirin and clopidogrel, remove the body’s ability to stop minor nasal bleeding quickly, so a small irritation in the thin nasal lining can become a recurrent nosebleed. This does not mean the drug should be stopped, since it is usually preventing something more serious. It does mean the bleeding should be managed and the dose reviewed with the prescriber.
Why does my blood-pressure medicine make me cough? A persistent dry cough is a well-known side effect of ACE inhibitors, a common class of blood-pressure drug, caused by a build-up of a signaling molecule called bradykinin. The cough is harmless but can be relentless and often leads people to an ENT office after cough syrups fail. It usually resolves after the prescriber switches to a different class of medication. The cough can begin weeks or months after starting the drug, which is why the connection is often missed.
Which medications most often cause dry mouth in older adults? The most frequent offenders are drugs with anticholinergic effects: first-generation antihistamines, tricyclic antidepressants, bladder-control medications, and several heart and blood-pressure drugs. Taking many medicines together raises the risk further. Dry mouth is worth treating because it accelerates tooth decay and makes swallowing harder. A pharmacist or physician can review the list and look for alternatives with less drying effect.
Is dizziness or tinnitus from medication reversible? Often, but it depends on the drug. Dizziness from blood-pressure medicines, sedatives, and similar drugs usually improves after a dose change. Tinnitus from aspirin, other NSAIDs, and loop diuretics typically fades once the drug is stopped. However, damage from aminoglycoside antibiotics and platinum chemotherapy can be permanent, which is why monitoring during those treatments matters. Any change should be made with a prescriber rather than by stopping the drug.
How many medications is “too many”? There is no single magic number, though taking five or more is the common definition of polypharmacy and ten or more clearly raises risk. What matters more than the count is whether each drug still does more good than harm for that person. The right question is not only “how many” but “is this one still needed.” A periodic medication review is the way to answer it.
Should I stop a medication I think is causing my symptoms? No — not on your own. Stopping certain drugs abruptly can be dangerous, and the right move is often a lower dose or a substitute rather than simply quitting. Bring your full medication list to your doctor or pharmacist, describe the symptom and when it started, and ask whether a change is reasonable. The goal is a planned adjustment, not an abrupt stop.
References
Cho HJ, Chae J, Yoon SH, Kim DS. Aging and the prevalence of polypharmacy and hyper-polypharmacy among older adults in South Korea: a national retrospective study during 2010-2019. Front Pharmacol. 2022;13:866318.
Hayslett RL, Marshall LL. Management of dry mouth. Sr Care Pharm. 2025;40(2):55-63.
Hung A, Kim YH, Pavon JM. Deprescribing in older adults with polypharmacy. BMJ. 2024;385:e074892.
Katzenberger B, Koller D, Strobl R, Kisch R, Sanftenberg L, Voigt K, Grill E. Exposure to anticholinergic and sedative medication is associated with impaired functioning in older people with vertigo, dizziness and balance disorders—results from the longitudinal multicenter study MobilE-TRA. Front Pharmacol. 2023;14:1136757.
Linsky AM, Motala A, Booth M, Lawson E, Shekelle PG. Deprescribing in community-dwelling older adults: a systematic review and meta-analysis. JAMA Netw Open. 2025;8(5):e259375.
Michalcova J, Vasut K, Airaksinen M, Bielakova K. Inclusion of medication-related fall risk in fall risk assessment tool in geriatric care units. BMC Geriatr. 2020;20(1):454.
O’Mahony D, Rochon PA. Prescribing cascades: we see only what we look for, we look for only what we know. Age Ageing. 2022;51(7):afac138.
O’Mahony D, Cherubini A, Guiteras AR, Denkinger M, Beuscart JB, Onder G, Gudmundsson A, Cruz-Jentoft AJ, Knol W, Bahat G, van der Velde N, Petrovic M, Curtin D. STOPP/START criteria for potentially inappropriate prescribing in older people: version 3. Eur Geriatr Med. 2023;14(4):625-632.
Shoair OA, Nyandege AN, Slattum PW. Medication-related dizziness in the older adult. Otolaryngol Clin North Am. 2011;44(2):455-471.
Sondh HK, Bishara D, Perera G, Shetty H, Stewart R, Mueller C. Medications associated with dizziness or hypotension and adverse outcomes: an electronic health record study in older adults with dementia. Age Ageing. 2025;54(6):afaf154.
Soto AP, Meyer SL. Oral implications of polypharmacy in older adults. Clin Geriatr Med. 2023;39(2):273-293.
Steyger PS. Mechanisms of aminoglycoside- and cisplatin-induced ototoxicity. Am J Audiol. 2021;30(3S):887-900.
Wu T, Zhao Z, Wang P, Du Q, Shi Y, Zhu B, Dong J, Li D. Drug-induced hearing loss: a real-world pharmacovigilance study using the FDA adverse event reporting system database. Hear Res. 2025;461:109262.
Zhou D, Chen Z, Tian F. Deprescribing interventions for older patients: a systematic review and meta-analysis. J Am Med Dir Assoc. 2023;24(11):1718-1725.
For more interesting contents:
https://curiousmd.com/global-aging-and-ai-medicine/
https://curiousmd.com/acetaminophen-vs-nsaids-evidence/
https://curiousmd.com/cough-that-wont-go-away-after-a-cold/
https://curiousmd.com/future-of-clinical-decision-support/
Link out to:
- What Is Tinnitus? — National Institute on Deafness and Other Communication Disorders (NIDCD) — a clear, authoritative overview of tinnitus and how it relates to hearing and medications.
- Taking Medicines Safely as You Age — National Institute on Aging (NIA) — practical guidance on managing multiple medications and avoiding interactions.
- Medication Overload and Older Americans — Lown Institute — research on the scale and harms of taking too many medications later in life.
Joonpyo Hong, MD is a board-certified otolaryngologist practicing in Korea. This article reflects his clinical interpretation of published research and does not constitute individual medical advice.