
A generation ago, only about one in six oropharyngeal cancers in the United States tested positive for HPV; by the early 2000s, it was closer to seven in ten [Chaturvedi, Human papillomavirus and rising oropharyngeal cancer incidence in the United States, 2011]. That shift has turned the HPV vaccine and throat cancer into one of the most pressing questions in adult health — so this guide answers the four that adults ask most, honestly, including where prevention is powerful and where it runs out of road.
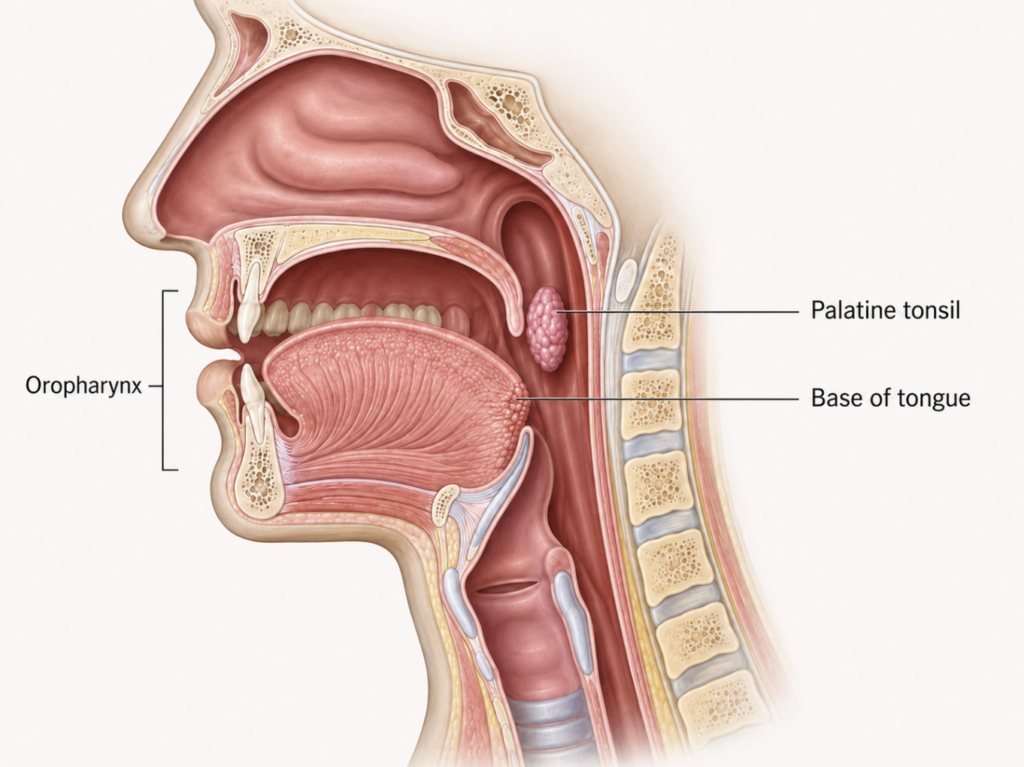
A quick note on names first. What many people call “throat cancer” from HPV is, more precisely, oropharyngeal cancer — cancer of the oropharynx, mainly meaning the tonsils and the base of the tongue. The distinction matters because these tumors behave differently from cancers elsewhere in the throat, so this article uses the term oropharyngeal cancer throughout, even though “throat cancer” is the phrase most people search for.
Why oropharyngeal cancer is rising — and why mostly in men
The change over the past few decades has been steep. HPV prevalence in these tumors rose from 16.3% in the mid-1980s to 71.7% by the early 2000s, and the population-level incidence of HPV-positive oropharyngeal cancer climbed 225% between 1988 and 2004 [Chaturvedi, 2011]. The same analysis projected that annual cases would overtake cervical cancer — and multiple U.S. epidemiologic datasets, including from the American Cancer Society, indicate HPV-positive oropharyngeal cancer has already done so. Korea reflects the same direction: it ranks among the countries where HPV-positive oropharyngeal cancer is both common and rising, and here too the disease falls mostly on younger men [Carlander, A Contemporary Systematic Review on Repartition of HPV-Positivity in Oropharyngeal Cancer Worldwide, 2021].
The burden falls disproportionately on men. A 2025 systematic review found oral HPV infection is consistently more common in males than females, with HPV16 the dominant high-risk type in the mouth and throat [Maltseva, Detection and natural history of HPV infection of oral cavity and tonsils, 2025]. Persistent oral HPV infection is the presumed precursor to these cancers, which is why the questions below matter for otherwise healthy adults [Rettig, The role of sexual behavior in head and neck cancer, 2015].
4 key questions every adult actually asks about HPV vaccine and throat cancer
1. Is there a test to know if I have HPV in my oropharynx?
No — there is no approved screening test. The CDC states plainly that there is no approved HPV test to detect the virus in the mouth or throat (CDC, 2025). This is the single biggest difference between oropharyngeal and cervical cancer, and it surprises most people.
The reason isn’t a lack of technology but a lack of meaning. Some laboratories sell oral-rinse or swab tests, but reviewers note that reliable sampling methods and a defined precursor lesion are still missing, so a result cannot tell you your cancer risk [Maltseva, 2025; Rettig, 2015]. The p16 tissue test people sometimes hear about is used after a tumor is found, to guide staging and treatment — it is a diagnostic tool, not a screening one.
2. If I already have HPV, is the vaccine still worth getting?
It can still help, but it will not treat what you already have. Based on how the vaccine works, prophylactic HPV vaccination is not expected to clear an active infection or reverse existing disease [Reuschenbach, Prophylactic HPV vaccines in patients with HPV-associated diseases and cancer, 2023].
The value that remains is real, though. The 9-valent HPV vaccine covers nine HPV types, and being infected with one does not mean you carry the others — so the vaccine can still protect against the covered types you have not encountered, and may guard against re-infection with a type you cleared naturally [Reuschenbach, 2023]. A useful way to frame it: the vaccine fills the gaps you do not yet have, rather than erasing the risk you already carry.
3. I have HPV but no cancer — do I just watch and wait?
There is no formal surveillance program, because there is nothing reliable to monitor. Unlike the cervix, where precancerous change is visible and treatable, the oropharynx has no accessible precursor lesion and no approved test to track infection over time [Rettig, 2015].
The reassuring part is that most oral HPV infections resolve on their own; only rare, persistent infection carries onward risk, and the tools to measure that persistence in clinic do not yet exist [Maltseva, 2025]. So “watching” is not really an option — awareness is.
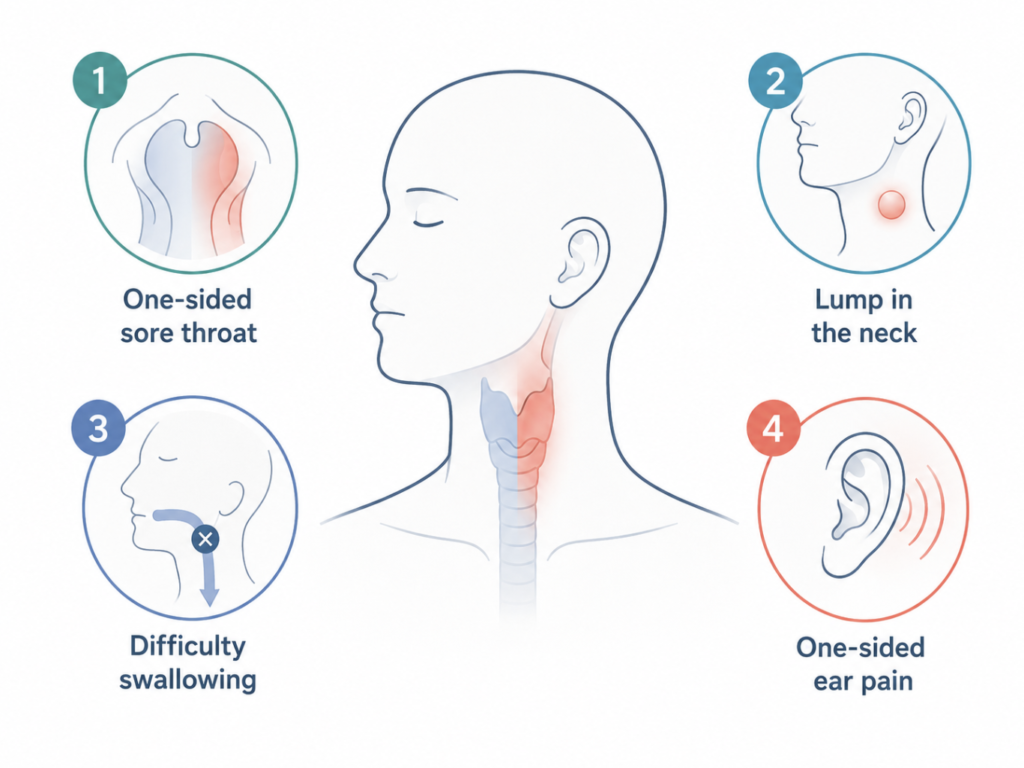
What matters instead is knowing the warning signs. A persistent one-sided sore throat, a painless lump in the neck, pain or difficulty swallowing, or one-sided ear pain lasting more than two to three weeks all warrant an ENT evaluation. Ear pain is easy to dismiss here, but a tumor in the tonsil or base of tongue can refer pain to the ear through shared nerve pathways, so a persistent one-sided earache with no ear infection deserves a look. This is about knowing when to get checked, not about self-diagnosis.
4. I don’t have HPV — is the vaccine worth it as an adult?
Yes — this is exactly who benefits most. Prophylactic vaccines work best before exposure, so an adult who has not encountered the covered types gets the fullest protection against future infection [Reuschenbach, 2023]. Encouragingly, vaccination is already associated with a significant reduction in vaccine-type oral HPV infection in the population [Maltseva, 2025].
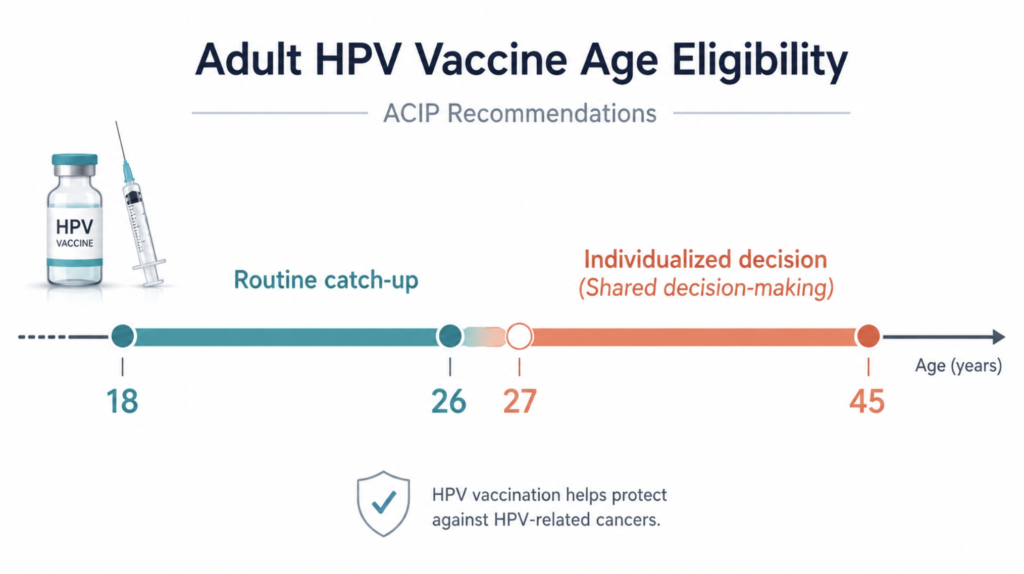
Age shapes the decision. In the United States, catch-up vaccination is recommended through age 26; for adults aged 27 to 45 it becomes an individual “shared clinical decision” with a clinician — most useful for those with ongoing risk of new exposure — and the vaccine is not licensed past age 45 (CDC, 2025).
Clinical Perspective
Cervical cancer has a safety net that oropharyngeal cancer simply does not: a screening test, a treatable precancer, and decades of organized follow-up. The oropharynx has none of these, which flips the logic of prevention. When there is no way to catch the disease early and nothing to monitor in between, the value of stopping the infection before it starts rises considerably. For a parent with a child in the eligible age range, or a younger adult who has not completed the series, that argument is straightforward. For adults between 27 and 45, it is a genuine conversation worth having with a clinician rather than an automatic yes — and worth having even for those who already know they carry HPV.
Key Takeaways
- HPV now drives roughly seven in ten U.S. oropharyngeal cancers, which have overtaken cervical cancer and fall mostly on men.
- There is no approved test to screen for HPV in the mouth or throat — the key difference from cervical cancer.
- The HPV vaccine is preventive, not therapeutic: it cannot clear an existing infection but can still protect against covered types you have not caught.
- Most oral HPV infections clear on their own, and there is no watch-and-wait program for the oropharynx — symptom awareness matters instead.
- Adults without prior exposure benefit most; catch-up is recommended through 26, individualized for 27–45, and not licensed past 45.
FAQ
Is there a test for HPV in the throat? No. There is no approved screening test to detect oral or oropharyngeal HPV infection, and a result would not reliably predict cancer risk. HPV testing on tissue happens only after a tumor is found, to guide treatment — not to screen healthy people.
Does the HPV vaccine work if I already have HPV? It will not clear an existing infection or reverse disease, but it can still protect against the other covered HPV types you have not yet encountered, and may help prevent re-infection. Because the 9-valent vaccine covers nine types, partial protection often remains worthwhile.
I’m HPV positive but have no cancer — what should I do? There is no surveillance program to enroll in, because the oropharynx has no monitorable precursor. Reassuringly, most infections clear naturally. Focus on warning signs instead: see an ENT for a persistent one-sided sore throat, neck lump, swallowing difficulty, or one-sided ear pain lasting more than a few weeks.
Is the HPV vaccine worth it for an adult who isn’t infected? Yes — uninfected adults gain the most, since the vaccine prevents future infection with covered types. It is recommended through age 26 and becomes an individual decision with your clinician from 27 to 45, based on your likelihood of new exposure.
References
Carlander AF, Jakobsen KK, Bendtsen SK, et al. A Contemporary Systematic Review on Repartition of HPV-Positivity in Oropharyngeal Cancer Worldwide. Viruses. 2021;13(7):1326.
Chaturvedi AK, Engels EA, Pfeiffer RM, et al. Human papillomavirus and rising oropharyngeal cancer incidence in the United States. J Clin Oncol. 2011;29(32):4294-4301.
Maltseva M, Klasen C, Wuerdemann N, et al. Detection and natural history of HPV infection of oral cavity and tonsils – a systematic literature review. BMC Cancer. 2025;25(1):1405.
Rettig E, Kiess AP, Fakhry C. The role of sexual behavior in head and neck cancer: implications for prevention and therapy. Expert Rev Anticancer Ther. 2015;15(1):35-49.
Reuschenbach M, Doorbar J, Del Pino M, et al. Prophylactic HPV vaccines in patients with HPV-associated diseases and cancer. Vaccine. 2023;41(42):6194-6205.
Joonpyo Hong, MD is a board-certified otolaryngologist practicing in Korea. This article reflects his clinical interpretation of published research and does not constitute individual medical advice.
For more interesting contents:
https://curiousmd.com/hpv-oropharyngeal-cancer/
https://curiousmd.com/cancer-of-unknown-primary-prognosis/
https://curiousmd.com/ai-de-escalation-in-hpv-throat-cancer/
Link out to:
HPV and Oropharyngeal Cancer — CDC:
https://www.cdc.gov/cancer/hpv/oropharyngeal-cancer.html
Oropharyngeal Cancer Treatment (PDQ) — National Cancer Institute:
https://www.cancer.gov/types/head-and-neck/patient/adult/oropharyngeal-treatment-pdq
Causes, Risk Factors, and Prevention — American Cancer Society:
https://www.cancer.org/cancer/types/oral-cavity-and-oropharyngeal-cancer/causes-risks-prevention.html