
An 82-year-old arrives at a clinic with a canvas bag of pill bottles and a new complaint: dizziness and two falls in a month. The neurological exam is unremarkable, the brain scan clean. The likeliest cause is in the bag. Twelve prescriptions sit there, written by four different clinicians over nine years, and at least three of them can leave an older person unsteady on their feet. No single prescription was a mistake. The trouble is that no one had looked at all twelve together.
This scene is ordinary — the everyday reality of polypharmacy in older adults. Across the world, about four in ten adults over 65 take five or more medicines, and more than one in ten take ten or more [Wang, Prevalence of Polypharmacy Worldwide, 2024; Kim, Global Prevalence of Polypharmacy, 2024]. The word for it — polypharmacy — sounds like a diagnosis, but it is closer to a byproduct. It is what medicine produces when it gets good at finding diseases, managing chronic conditions, and keeping people alive long enough to accumulate more of them.
That is the paradox at the center of this problem. Polypharmacy is not mainly a story of careless prescribing. It is most entrenched in wealthy, aged health systems with the best access to care — and it is spreading fastest to countries aging more quickly than the West ever did, often without the safety machinery to manage it. The problem is not the pills. It is a system that cannot keep track of them.
The paradox of success
Start with the numbers, translated into people. A pooled analysis of millions of older adults put worldwide polypharmacy at roughly two in five, and the heavier burden of ten-or-more medicines at more than one in ten [Wang, Prevalence of Polypharmacy Worldwide, 2024]; an umbrella review of the global literature landed in the same neighborhood [Kim, Global Prevalence of Polypharmacy, 2024]. These are not fringe figures — they describe the median older patient across much of the world.
The distribution is the revealing part. Polypharmacy is generally most common in wealthy, aged regions — Europe and North America — and less common across much of Asia and South America [Wang, Prevalence of Polypharmacy Worldwide, 2024; Kim, Global Prevalence of Polypharmacy, 2024]. Regional estimates vary between reviews, so the exact percentages should be read loosely; the gradient, however, is consistent. More medical wealth tends to mean more medicines.
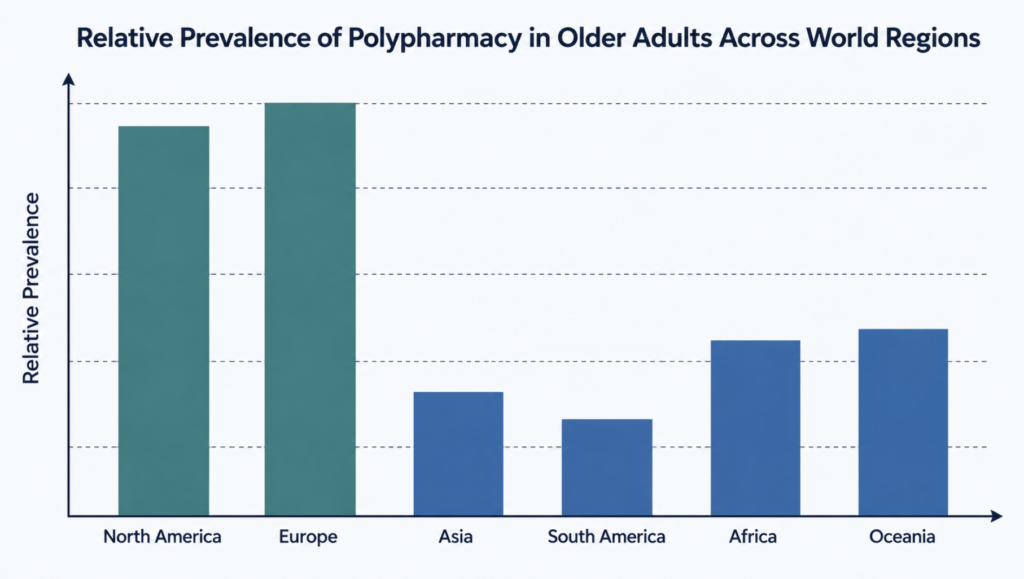
Why would better-resourced medicine produce more drugs per patient? Because access is the engine — a pattern visible even inside a single middle-income country. In national studies of older Brazilians, greater use of health services and private insurance both raised the odds of being on many drugs, and polypharmacy was markedly more common in the wealthier south than the poorer north [Seixas, Polypharmacy among Older Brazilians, 2021; Ramos, Polypharmacy among Older Adults in Brazil, 2022]. The link is associational, not proven cause and effect, but it points one way: the more health care people can reach, the more medicines they collect.
This matters more each year, because the population in question is growing. According to World Health Organization projections, the number of older adults is climbing steeply, and most of that growth is now occurring in lower- and middle-income countries [Endalifer, Polypharmacy in Northeast Ethiopia, 2025]. The demographic center of gravity of polypharmacy is shifting. What looks like a rich-world problem is becoming a global one.
The reframing is worth stating plainly. Multiple medicines in an older adult are not, by default, bad medicine — they are often the residue of good medicine applied one condition at a time. That makes the problem harder, not easier: there is no villain to remove, only a system to redesign.
The other half of the paradox
If access explains the wealthy world, a different failure explains much of the rest. Developing countries are not spared; in several studied closely, the numbers rival high-income settings. In older Ethiopian patients, polypharmacy has been measured at roughly one in three, with inappropriate medicines in four to five of every ten and drug interactions in nearly half [Bhagavathula, Polypharmacy in a Developing Country, 2021; Endalifer, Polypharmacy in Northeast Ethiopia, 2025]. These figures come from specific countries, not a verdict on every developing system — but they dispel a comfortable assumption: that fewer resources means fewer drugs, and less harm.
The mechanism differs. Where wealthy systems over-supply, many lower-income systems under-monitor. A drug reaction is only useful as a warning if it is recorded, and recording is where these systems thin out. In a survey of Ghanaian health professionals, most had encountered an adverse drug reaction, but only about half had ever reported one, and formal knowledge of how to report was low [Yawson, ADR Reporting in Ghana, 2022].
Across Africa, only a minority of countries have opened adverse-reaction reporting to patients themselves [Adedeji-Adenola, Direct ADR Reporting in Africa, 2020]. Over-the-counter access widens the gap: in India, casual use of non-prescription painkillers is widespread while awareness of their harms and of reporting remains limited [Dash, Pharmacovigilance of NSAIDs in India, 2024].
The blind spot is not confined to poorer countries. Even where reporting systems exist, only a small fraction of drug reactions is ever formally captured, and a culture of blame keeps clinicians from filing what they see [Parracha, Mobile Apps for ADR Reporting, 2022; Afaya, Barriers to Reporting Medication Errors, 2021]. A system that cannot see its own harm cannot correct it.
The two halves of the paradox are best seen side by side.
| Wealthy, aged systems | Many lower-income systems | |
|---|---|---|
| Main driver | Over-supply: high access, more prescribers, more guidelines | Under-monitoring: weak surveillance, limited training |
| How drugs accumulate | Each specialist prescribes correctly for one disease | Prescribing plus easy over-the-counter and informal use |
| Safety net | Reporting systems exist but capture little | Reporting systems often absent or unknown to staff |
| Patient education | Assumed, often thin | Frequently minimal |
| Shared endpoint | Many drugs, few people watching the whole list | Many drugs, few people watching the whole list |
The columns differ; the last row does not. Whether by abundance or by neglect, the patient ends up on a pile of medicines that no one is accountable for as a whole. And the countries inheriting this problem fastest are the ones with the least-developed machinery to contain it.
Clinical Perspective. Treating polypharmacy as a wealthy-world luxury problem is a clinical error. In a lower-resource setting the same drug count often carries more danger, not less, because the systems that would catch an interaction or a reaction are thinner. The number of medicines matters; the number of people watching them matters more.
How the system let it happen
If no single prescriber creates polypharmacy, what does? The honest answer is that several reasonable forces converge, and the harm emerges from their sum.
The first is the structure of medical knowledge itself. Clinical guidelines are written largely one disease at a time, and rarely account for the frail, multimorbid older patient in the room [Krishnaswami, Deprescribing in Cardiovascular Disease, 2019; Liau, Medication Management in Frail Older People, 2021]. Follow the diabetes, hypertension, and osteoporosis guidelines faithfully, and the prescriptions add up — each defensible, the total unexamined.
The second is the prescribing cascade: a side effect of one drug is mistaken for a new illness and treated with a second drug [McCarthy, Appropriateness of Prescribing Cascades, 2019]. A blood-pressure medicine causes ankle swelling; a diuretic is added for the swelling; the diuretic causes its own trouble. Not every cascade is an error — some added drugs are appropriate — but many are invisible extensions of an unrecognized reaction.
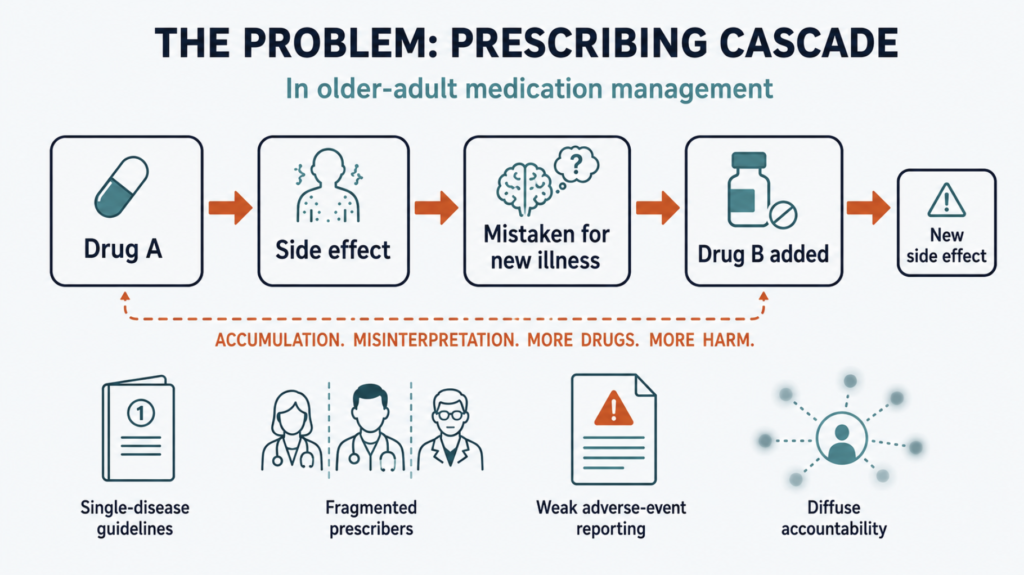
The third is diffuse accountability. Interviews with patients and clinicians suggest cascades persist partly because no one owns the whole medication list; responsibility is spread across specialists, and awareness of what the others have prescribed is patchy [Farrell, Development and Resolution of Prescribing Cascades, 2020]. A list that belongs to everyone belongs to no one.
The fourth is a weak feedback loop: because so few drug reactions are formally reported, the system rarely learns which combinations are hurting people [Parracha, Mobile Apps for ADR Reporting, 2022]. The fifth is the patient’s own trust — qualitative work with the very old finds that many treat their medicines as a settled routine and rarely question a drug themselves [Adamson, Medication Work among Nonagenarians, 2023]. That trust is reasonable, but it means the impulse to review must come from the system, not the patient.
The crux is a distinction lost in the alarm over pill counts. A great deal of polypharmacy is appropriate; some patients genuinely need many drugs. The target is problematic polypharmacy — the drugs that no longer serve the person carrying them [McCarthy, Appropriateness of Prescribing Cascades, 2019]. Not fewer medicines for their own sake, but medicines that still earn their place.
Clinical Perspective. Each mechanism above is individually rational, which is exactly why the problem is durable. There is no single decision to reverse. The clinical task is to make the whole list visible to one accountable person on a regular schedule — because the harm lives not in any one prescription, but in the space between them.
What a better system looks like
The problem is systemic, so the remedies are too. They stack in layers, from global policy down to a single clinic visit.
At the top sits a policy target. In 2017 the World Health Organization launched its third global patient safety challenge, Medication Without Harm, with the stated aim of halving serious, avoidable medication-related harm [Donaldson, Medication Without Harm, 2017; Sheikh, Third Global Patient Safety Challenge, 2017]. The deadline it set has since passed, and the target was not met — but the framing endures: medication harm is a safety problem to be engineered down, not an unavoidable cost of care.
Beneath policy sits the core clinical act — structured medication review and deprescribing, the planned, supervised withdrawal of drugs that no longer help. Here precision matters, because the evidence is genuinely mixed. Deprescribing reliably trims inappropriate medicines and pill counts, and some analyses show fewer adverse drug reactions [Linsky, Deprescribing in Community-Dwelling Older Adults, 2025; Zhou, Deprescribing Interventions for Older Patients, 2023].
Whether it clearly prevents hospital stays or extends life is not yet settled — the reduction is often small per patient, and only about half of tested programs beat usual care on their main outcome [Linsky, Deprescribing in Community-Dwelling Older Adults, 2025; Hung, Deprescribing in Older Adults with Polypharmacy, 2024]. It is sound practice with an honest ceiling on its proven benefits.
The next layer is tools. Validated checklists — the STOPP/START criteria and the Beers list among them — help clinicians flag risky prescriptions and decide whom to review first [O’Mahony, STOPP/START Criteria Version 3, 2023; Marvin, Targeting Patients for Medication Review, 2018]. They identify problems; they do not, by themselves, guarantee better outcomes, and work best aimed at patients who already have many drugs [Marvin, Targeting Patients for Medication Review, 2018].
Below that sit the operational building blocks expert panels keep returning to: reconciling the full list at every transition of care, pharmacist-led review, and regular checks tied to the patient’s goals [Jokanovic, Managing Polypharmacy in Aged Care, 2017; Liau, Medication Management in Frail Older People, 2021]. And beneath all of it, especially in lower-income settings, is surveillance — making reporting easy (reporting apps now run in a dozen lower-income countries) and replacing blame with a culture that treats a reported reaction as data, not fault [Parracha, Mobile Apps for ADR Reporting, 2022; Afaya, Barriers to Reporting Medication Errors, 2021].
The tension across all these layers is the same. Process improves more reliably than outcomes. It is easier to run a review than to prove the review saved a life. A system that measures its own activity will always look busy; the harder discipline is to judge it by what happens to patients.
Clinical Perspective. The lesson of the deprescribing evidence is not discouragement but calibration. Removing a drug that no longer helps is defensible on its own terms — less burden, less risk, lower cost — even where the survival data are unsettled. What the evidence forbids is the promise that any single intervention will transform outcomes. The gain is real and modest, and modest is not nothing.
The frontier: technology, AI, and a proposal
If no one sees the whole patient, software is an obvious candidate to help. The record so far is instructive — and more sobering than the marketing suggests.
Rule-based electronic tools already exist and have been tested properly. The large European OPERAM trial paired a software-supported medication review with expert oversight for hospitalized older adults; drug-related readmissions fell, but not by a statistically convincing margin [Salari, Cost-Effectiveness of Medication Review (OPERAM), 2022]. A United States tool that flagged inappropriate medicines and reconciliation errors improved communication and record accuracy, yet did not reduce the number of medicines or inappropriate prescriptions — its trial, though, was small [Fried, Tool to Reduce Inappropriate Medications, 2017]. Other systems generating patient-specific deprescribing reports have been trialed in the same vein [Gray, Medication Use Quality and Safety, 2023]. The pattern repeats: these tools reliably improve the process and inconsistently move the outcomes.
The need is real. In the OPERAM population, more than half of older patients carried at least one clinically important drug interaction, and a handful of patterns accounted for most of them, with the heaviest medication users most affected [Zerah, Drug-Drug Interactions in Older People (OPERAM), 2021].
Artificial intelligence is the newest entrant, and it is early. Tested on emergency-department deprescribing, a large language model was good at spotting which prescribing rules might apply — better than trainees — but worse at judging whether a rule fit the specific case, and its confidence did not track its accuracy [Socrates, Identifying Deprescribing Opportunities with LLMs, 2025].
Reviews of the field reach a consistent verdict: the role of these tools is barely established, and they need extensive validation before routine use [Al Meslamani, AI Tools in Deprescribing, 2025; Phutietsile, Rethinking Anticholinergic Burden, 2025]. Connected pill dispensers and remote monitoring are further along for the narrower task of helping people take their medicines, but software that reasons about the whole regimen is still largely outside the clinic [Taher, Polypharmacy in Older Cancer Patients, 2026].
One piece of biology constrains any such system. As the body ages, the kidneys and liver clear drugs more slowly, and sensitivity to many drugs rises [Ngcobo, Ageing and Pharmacokinetics, 2025]. A dose that is safe at fifty can over-expose the same person at eighty, even when nothing about the prescription changes. This is established physiology, not speculation — precisely the individual adjustment today’s blunt interaction checkers ignore.
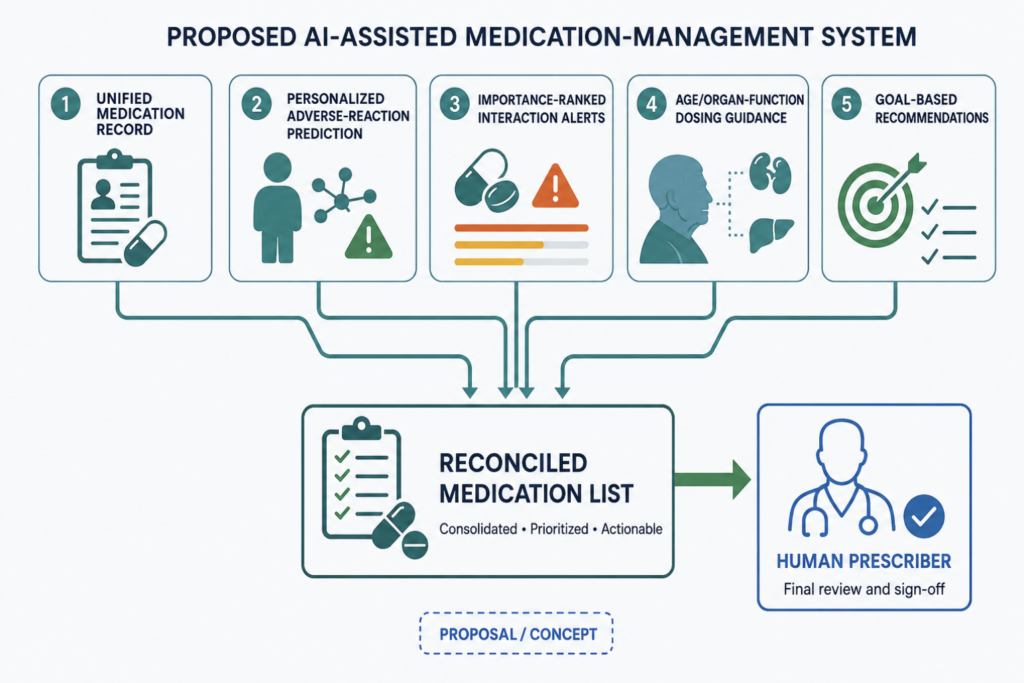
What follows is a proposal, not a finding — one physician’s sketch of what a system worth building would do, offered as informed opinion rather than evidence. No such system has been shown to improve patient outcomes, and none should be trusted until it has. With that caution stated plainly, five functions would separate a useful tool from the underwhelming ones already tried.
The first is a single, unified medication record that gathers every prescription across hospitals and pharmacies into one list and reconciles it at each transition — the missing “whole patient” that fragmentation destroys.
The second is personalized reaction prediction: an estimate, tuned to age and conditions, of which drugs are most likely to cause trouble, with a prompt asking whether a new symptom might be a drug effect rather than a new disease — the cascade, interrupted.
The third is interaction alerting ranked by clinical importance rather than listed exhaustively, so the few dangerous combinations surface instead of drowning in trivial ones.
The fourth is dosing guidance personalized to age and organ function, so declining clearance triggers a warning the standard checker never issues.
The fifth, non-negotiable, is that every recommendation ends at a human prescriber — because this generation of tools is confident precisely where it is least reliable.
Done right, such a system would do what no individual clinician reliably can: hold the entire regimen in view and reason about it as one. Done wrong — deployed without the full list, unvalidated against outcomes, or trusted to decide on its own — it would be one more expensive layer that improves the paperwork, not the patient.
Clinical Perspective. The tool that finally helps with polypharmacy will not be the one that prescribes. It will be the one that lets a single accountable person see the whole patient at once, and then gets out of the way of the decision. Technology can close the visibility gap that fragmentation opened; it cannot supply the judgment or the accountability, and should not be asked to. Polypharmacy is a problem medicine’s success created, and only a redesigned system — with better tools inside it, not in place of it — will resolve it.
Key Takeaways
- Polypharmacy in older adults is less a failure of prescribing than a byproduct of medical success: better access, longer lives, and one-disease-at-a-time care.
- It is most common in wealthy, aged systems yet shifting fastest to lower-income countries that age quickly and monitor weakly — over-supply and under-surveillance converging on one endpoint: a medication list no one owns as a whole.
- Deprescribing dependably reduces inappropriate drugs and pill counts; its effect on hospital stays and survival is real but unsettled, and should not be oversold.
- The fix is a system, not a slogan: one accountable owner of the full list, structured review, honest surveillance, and validated tools.
- Existing decision-support software and early AI improve the process more than the outcomes; a useful system must see the whole regimen and keep a human at the decision.
FAQ
Is taking many medications always bad for older adults?
No. Much polypharmacy is appropriate, and some patients genuinely need several drugs. The concern is problematic polypharmacy — medicines that no longer help the person taking them, which a periodic review of the full list is designed to find [McCarthy, Appropriateness of Prescribing Cascades, 2019].
Should an older adult stop medicines to reduce the count?
No — not on their own. Stopping the wrong drug can be dangerous, and the count itself is not the target. Deprescribing is a planned, supervised process; it reliably trims inappropriate drugs, though its effect on hard outcomes is still being established [Linsky, Deprescribing in Community-Dwelling Older Adults, 2025].
Do developing countries have less of a polypharmacy problem?
Not necessarily. In several studied settings the drug counts approach those of wealthy countries, and interactions are common — while the reporting systems that would catch harm are often weak or absent [Bhagavathula, Polypharmacy in a Developing Country, 2021; Adedeji-Adenola, Direct ADR Reporting in Africa, 2020].
Can AI fix polypharmacy?
Not yet. Early tests show AI can flag which prescribing rules might apply but struggles to judge whether they fit an individual patient, and it can be confidently wrong; the field needs far more validation before such tools are trusted in routine care [Socrates, Identifying Deprescribing Opportunities with LLMs, 2025; Al Meslamani, AI Tools in Deprescribing, 2025].
References
- Wang Z, Liu T, Su Q, et al. Prevalence of polypharmacy in the elderly population worldwide: a systematic review and meta-analysis. Pharmacoepidemiol Drug Saf. 2024;33(8):e5880.
- Kim S, Lee H, Park J, et al. Global and regional prevalence of polypharmacy and related factors: an umbrella review. Arch Gerontol Geriatr. 2024;124:105465.
- Seixas BV, Freitas GR. Polypharmacy among older Brazilians: prevalence, factors associated, and sociodemographic disparities (ELSI-Brazil). Pharm Pract (Granada). 2021;19(1):2168.
- Ramos KA, Boing AC, Bof de Andrade F. Polypharmacy among older adults in Brazil: association with sociodemographic factors and access to health services. Dialogues Health. 2022;1:100078.
- Endalifer BL, Kassa MT, Ejigu YW, Ambaye AS. Polypharmacy, drug-drug interactions, and potentially inappropriate medications among older adults in Northeast Ethiopia: a cross-sectional study. Front Public Health. 2025;13:1525079.
- Bhagavathula AS, Gebreyohannes EA, Fialova D. Prevalence of polypharmacy and risks of potentially inappropriate medication use in the older population in a developing country: a systematic review and meta-analysis. Gerontology. 2021;68(2):136-145.
- Yawson AA, Abekah-Nkrumah G, Okai GA, Ofori CG. Awareness, knowledge, and attitude toward adverse drug reaction reporting among healthcare professionals in Ghana. Ther Adv Drug Saf. 2022;13:20420986221116468.
- Adedeji-Adenola H, Nlooto M. Direct reporting of adverse drug reactions by healthcare consumers in Africa: a narrative review. Int J Clin Pharm. 2021;43(1):11-24.
- Dash S, Singh PA, Bajwa N, Choudhury A, Bisht P, Sharma R. Why pharmacovigilance of non-steroidal anti-inflammatory drugs is important in India? Endocr Metab Immune Disord Drug Targets. 2024;24(7):731-748.
- Parracha ER, Advinha AM, Lopes MJ, Oliveira-Martins S. Mobile apps for quick adverse drug reaction report: a scoping review. Pharmacoepidemiol Drug Saf. 2023;32(1):19-27.
- Afaya A, Konlan KD, Kim Do H. Improving patient safety through identifying barriers to reporting medication administration errors among nurses: an integrative review. BMC Health Serv Res. 2021;21(1):1156.
- Krishnaswami A, Steinman MA, Goyal P, et al. Deprescribing in older adults with cardiovascular disease. J Am Coll Cardiol. 2019;73(20):2584-2595.
- Liau SJ, Lalic S, Sluggett JK, et al. Medication management in frail older people: consensus principles for clinical practice, research, and education. J Am Med Dir Assoc. 2021;22(1):43-49.
- McCarthy LM, Visentin JD, Rochon PA. Assessing the scope and appropriateness of prescribing cascades. J Am Geriatr Soc. 2019;67(5):1023-1026.
- Farrell BJ, Jeffs L, Irving H, McCarthy LM. Patient and provider perspectives on the development and resolution of prescribing cascades: a qualitative study. BMC Geriatr. 2020;20(1):368.
- Adamson J, Hanson H, Todd A, Duncan R, Hanratty B, Robinson L. Medication work among nonagenarians: a qualitative study of the Newcastle 85+ cohort participants. Br J Gen Pract. 2023;73(729):e267-e275.
- Donaldson LJ, Kelley ET, Dhingra-Kumar N, Kieny MP, Sheikh A. Medication without harm: WHO’s third global patient safety challenge. Lancet. 2017;389(10080):1680-1681.
- Sheikh A, Dhingra-Kumar N, Kelley E, Kieny MP, Donaldson LJ. The third global patient safety challenge: tackling medication-related harm. Bull World Health Organ. 2017;95(8):546-546A.
- Linsky AM, Motala A, Booth M, Lawson E, Shekelle PG. Deprescribing in community-dwelling older adults: a systematic review and meta-analysis. JAMA Netw Open. 2025;8(5):e259375.
- Zhou D, Chen Z, Tian F. Deprescribing interventions for older patients: a systematic review and meta-analysis. J Am Med Dir Assoc. 2023;24(11):1718-1725.
- Hung A, Kim YH, Pavon JM. Deprescribing in older adults with polypharmacy. BMJ. 2024;385:e074892.
- O’Mahony D, Cherubini A, Renom Guiteras A, et al. STOPP/START criteria for potentially inappropriate prescribing in older people: version 3. Eur Geriatr Med. 2023;14(4):625-632.
- Marvin V, Ward E, Jubraj B, Bower M, Bovill I. Improving pharmacists’ targeting of patients for medication review and deprescription. Pharmacy (Basel). 2018;6(2):32.
- Jokanovic N, Wang KN, Dooley MJ, et al. Prioritizing interventions to manage polypharmacy in Australian aged care facilities. Res Social Adm Pharm. 2017;13(3):564-574.
- Salari P, O’Mahony C, Henrard S, et al. Cost-effectiveness of a structured medication review approach for multimorbid older adults: within-trial analysis of the OPERAM study. PLoS One. 2022;17(4):e0265507.
- Fried TR, Niehoff KM, Street RL Jr, et al. Effect of the Tool to Reduce Inappropriate Medications on medication communication and deprescribing. J Am Geriatr Soc. 2017;65(10):2265-2271.
- Gray SL, Brandt N, Schmader KE, Hanlon JT. Medication use quality and safety in older adults: 2022 update. J Am Geriatr Soc. 2024;72(5):1329-1337.
- Zerah L, Henrard S, Wilting I, et al. Prevalence of drug-drug interactions in older people before and after hospital admission: analysis from the OPERAM trial. BMC Geriatr. 2021;21(1):571.
- Socrates V, Wright DS, Huang T, et al. Identifying deprescribing opportunities with large language models in older adults: retrospective cohort study. JMIR Aging. 2025;8:e69504.
- Al Meslamani AZ. Management of polypharmacy through deprescribing in older patients: a review of the role of AI tools. Expert Rev Clin Pharmacol. 2025;18(6):333-345.
- Phutietsile GO, Nishtala PS. Rethinking anticholinergic burden in older adults: innovative approaches to detection and management. Expert Rev Clin Pharmacol. 2025;18(8):551-562.
- Taher ASM, Slavova-Boneva V, Battisti NML. Polypharmacy, medicine optimisation, and medication adherence in older cancer patients. Curr Oncol Rep. 2026;28(1).
- Ngcobo NN. Influence of ageing on the pharmacodynamics and pharmacokinetics of chronically administered medicines in geriatric patients: a review. Clin Pharmacokinet. 2025;64(3):335-367.
Joonpyo Hong, MD is a board-certified otolaryngologist practicing in Korea. This article reflects his clinical interpretation of published research and does not constitute individual medical advice.
This article is not intended to advertise or promote any specific company or product.
For more interesting contents:
https://curiousmd.com/medications-that-cause-dizziness-in-older-adults/
https://curiousmd.com/acetaminophen-vs-nsaids-evidence/
https://curiousmd.com/global-aging-and-ai-medicine/