Two drugs that share a shelf and a colloquial label, but not a mechanism, a toxicity profile, or a clean answer to the only question that matters at the clinic door: when did the fever really stop being a fever?
Acetaminophen vs NSAIDs (non-steroidal anti-inflammatory drugs) — paracetamol, ibuprofen, naproxen, aceclofenac, and their cousins — are dispensed across pharmacy counters, prescribed in primary care, and stacked in home medicine cabinets as if they were variants of one drug.
These two drug classes occupy different anatomical compartments, accumulate damage in different organs, and lose their effect on different clocks. The popular grammar of “take both, take alternately, take whichever” rests on a fact (the combination is genuinely additive for acute pain) and a fiction (the two drugs are interchangeable). Untangling the fact from the fiction is the only honest way to answer the practical questions: what does combining them buy, what does it cost, and how long must they wear off before a temperature reading at the hospital reflects the patient and not the prescription?
What follows is an evidence-led tour through five questions that clinicians and patients ask repeatedly and answer inconsistently.
Two drugs, two compartments
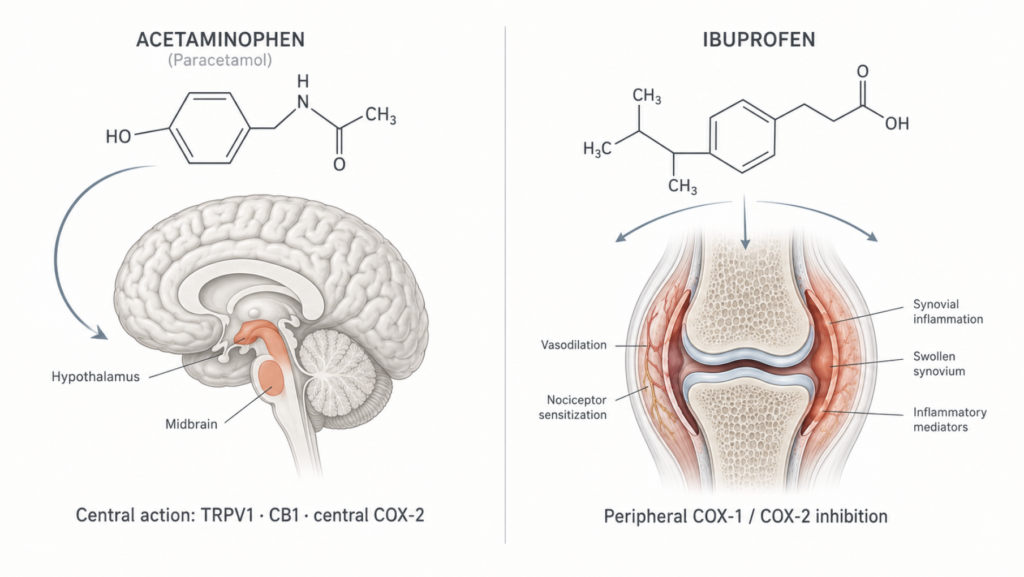
NSAIDs work in the periphery. Their target is cyclooxygenase (COX-1 and COX-2), which converts arachidonic acid into prostaglandins — including prostaglandin E2 (PGE2), the principal mediator of pain and inflammation at injured tissue. Block COX in inflamed tissue and prostaglandin synthesis falls, the sensitised nociceptor calms, and the cardinal signs of inflammation recede [Coxib and Traditional NSAID Trialists’ (CNT) Collaboration, Lancet 2013]. COX-1 also maintains gastric mucosal blood flow and renal afferent arteriolar tone; the same blockade that produces analgesia produces gastric injury and reduced glomerular filtration. This is why NSAIDs are anti-inflammatory and also why they bleed and damage kidneys.
Acetaminophen works centrally. It is, mechanistically, not an NSAID. Under physiological conditions in inflamed tissue — where peroxide tone is high — acetaminophen is a very weak COX inhibitor and has essentially no peripheral anti-inflammatory activity [Ohashi, Analgesic Effect of Acetaminophen, Front Pharmacol 2020]. Its analgesia is mediated through a metabolite, N-acylphenolamine (AM404), which crosses the blood-brain barrier and acts on TRPV1 and cannabinoid CB1 receptors in the central nervous system. Its antipyresis is mediated by lowering the hypothalamic thermoregulatory setpoint, probably through central COX-2 inhibition that proceeds when peroxide tone is low [Hinz, FASEB J 2008]. Acetaminophen is therefore an analgesic and an antipyretic. It is not an anti-inflammatory.
Clinical Perspective. “Anti-inflammatory” is not a marketing label. It is a mechanism, and acetaminophen does not have it. Patients with acute soft-tissue inflammation, dental inflammation, gout, or musculoskeletal injury who are switched to acetaminophen to “avoid the side effects of NSAIDs” are not receiving a milder version of the same drug. They are receiving a different drug aimed at a different target.
The combination question — additive, not magical
The strongest single data point on combination therapy comes from postoperative acute pain. In the Cochrane review of single-dose oral ibuprofen plus paracetamol in adults, the combination produced the lowest number-needed-to-treat (NNT) across the entire single-dose analgesic database — ibuprofen 200 mg plus paracetamol 500 mg yielded an NNT of 1.6 (95% CI 1.5–1.8) for at least 50% pain relief, and ibuprofen 400 mg plus paracetamol 1000 mg an NNT of 1.5 [Derry, Cochrane 2013; Moore, Cochrane 2015]. Translated into clinical language: about two out of three patients given the combination get meaningful pain relief that they would not have gotten on placebo. Few analgesic interventions in the Cochrane catalogue beat this.
| Regimen (single oral dose) | NNT for ≥50% pain relief (95% CI) | Source |
|---|---|---|
| Paracetamol 1000 mg alone | 3.6 (3.4–4.0) | Toms, Cochrane 2008 (CD004602) |
| Ibuprofen 200 mg alone | 2.7 (2.5–3.0) | Derry, Cochrane 2009 (CD001548) |
| Ibuprofen 400 mg alone | 2.5 (2.4–2.6) | Derry, Cochrane 2009 (CD001548) |
| Ibuprofen 200 mg + Paracetamol 500 mg | 1.6 (1.5–1.8) | Derry, Cochrane 2013 (CD010210) |
| Ibuprofen 400 mg + Paracetamol 1000 mg | 1.5 (1.4–1.7) | Derry, Cochrane 2013 (CD010210) |
Lower NNT = more effective. Values consolidated in Moore RA et al., Cochrane Database Syst Rev 2015 (CD008659.pub3, single dose oral analgesics overview).
The additivity is real but bounded. When two drug-specific effect sizes are summed and compared with the observed combination effect, the assumption that combination analgesia is the sum of individual effects holds across a range of drug pairs, including ibuprofen plus paracetamol [Moore, A conservative method of testing whether combination analgesics produce additive or synergistic effects, Eur J Pain 2012]. The combination is additive; it is not synergistic.
For fever in children — a separate question — the data are more modest. The Cochrane review pooled six trials of 915 children and found that combined paracetamol plus ibuprofen lowered mean temperature by about 0.27 °C at one hour and 0.70 °C at four hours compared with monotherapy (moderate quality evidence), and reduced the number of children remaining febrile at four hours [Wong, Cochrane 2013]. A subsequent updated meta-analysis of nine trials (2,026 children) reported a mean temperature difference of −0.29 °C at one hour, with no statistical difference at four or six hours, but more children reaching apyrexia by six hours with combined therapy [Trippella, Front Pediatr 2019].
Read in plain language: combining the two drugs in a febrile child lowers the temperature roughly a quarter of a degree more than either drug alone, and the child is more likely to be afebrile a few hours later. Whether a quarter of a degree justifies two simultaneous medications is a separate question; major guidelines (NICE, AAP, Italian Pediatric Society) recommend single-agent therapy as the default precisely because the marginal benefit is small.
Clinical Perspective. The combination works for acute pain in a way that monotherapy does not match; the same combination for fever in an otherwise well child buys a fraction of a degree. Treat the pain aggressively. Treat the fever for comfort.
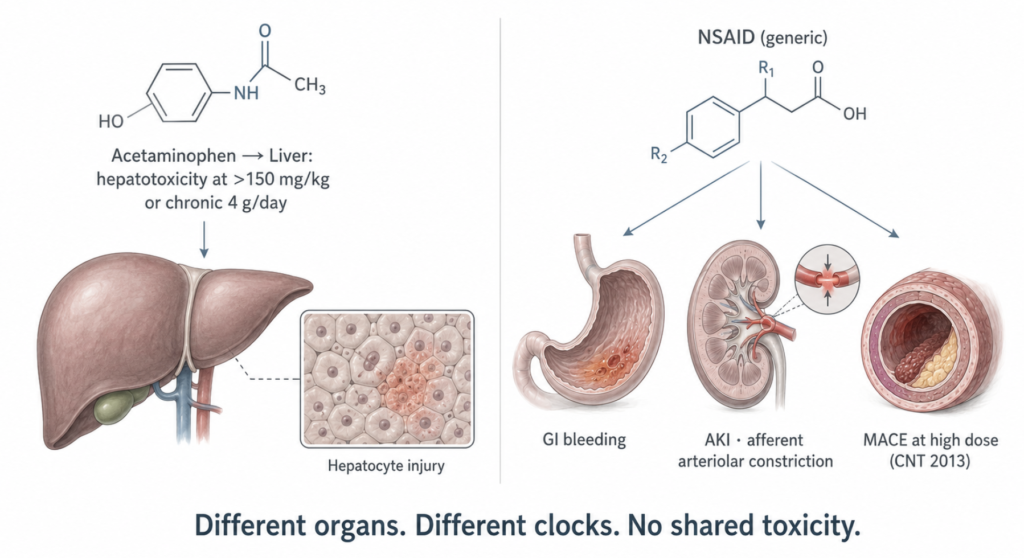
Side-effect profiles do not merge
The toxicities of these two drug classes do not stack into a single risk; they live in different organs and accumulate on different schedules.
Acetaminophen damages the liver. At therapeutic doses (≤4 g/day in healthy adults), the risk is small but not zero. In a randomised controlled trial of 145 healthy adults given 4 g/day of acetaminophen for 14 days, about a third developed transient alanine aminotransferase (ALT) elevations above three times the upper limit of normal, with peaks reaching up to twelvefold; the elevations resolved on continuation or discontinuation [Watkins, JAMA 2006]. Acute hepatotoxicity becomes clinically dangerous at single ingestions above roughly 150 mg/kg, generally >7.5 g in adults, and the risk is amplified by chronic alcohol use, malnutrition, fasting, CYP2E1-inducing drugs, and pre-existing liver disease [LiverTox, Acetaminophen entry]. The FDA has suggested but not mandated a lower daily ceiling of 3–3.25 g; in 2011 McNeil voluntarily lowered the Extra Strength Tylenol label from 4 g/day to 3 g/day, and the FDA separately mandated that prescription combination products contain no more than 325 mg of acetaminophen per dosage unit.
NSAIDs damage the gut, the kidneys, and the arteries. In the largest individual-participant meta-analysis (CNT Collaboration, 754 trials, ~353,000 participants), high-dose diclofenac and high-dose ibuprofen each increased the relative risk of a major vascular event (non-fatal MI, non-fatal stroke, or vascular death) by approximately one-third. For 1,000 high-risk patients treated for a year, this translated into about seven to eight extra major vascular events, of which roughly two would be fatal [CNT Collaboration, Lancet 2013]. High-dose naproxen was notably less cardiotoxic. Upper gastrointestinal complications rose with all non-selective NSAIDs; a recent meta-analysis put ibuprofen’s odds ratio for GI bleeding at 2.28 (the lowest among non-selective agents) and ketorolac’s at 20.67 [Tawfik, Clin Pharmacol Ther 2025]. NSAIDs also acutely reduce renal perfusion via afferent arteriolar constriction and can precipitate acute kidney injury, particularly in dehydrated patients, those on diuretics or ACE inhibitors, and the elderly.
What happens when the two are combined? The Cochrane single-dose review actually found fewer adverse events with ibuprofen plus paracetamol than with placebo across pooled studies, with serious events at roughly 1 per 3,200 participants [Moore, Adverse events after single dose oral analgesics, Cochrane 2015]. Short-term combination does not introduce new toxicities, and it does not multiply existing ones. But the data are largely from single-dose postoperative trials. The longer the combination is used, the more each drug’s individual ceiling — liver for acetaminophen, GI/renal/cardiovascular for NSAIDs — comes back into play independently. There is no shared organ in which they compound.
Clinical Perspective. The two drugs do not share a failure mode. They share a shelf. Patients who take 4 g of acetaminophen daily with full-dose ibuprofen for a week are not running double the same risk; they are running two separate clocks toward two separate organs. The clinical task is to keep both clocks below their alarms, not to imagine them as one.
Duration of effect — what the dosing intervals really mean
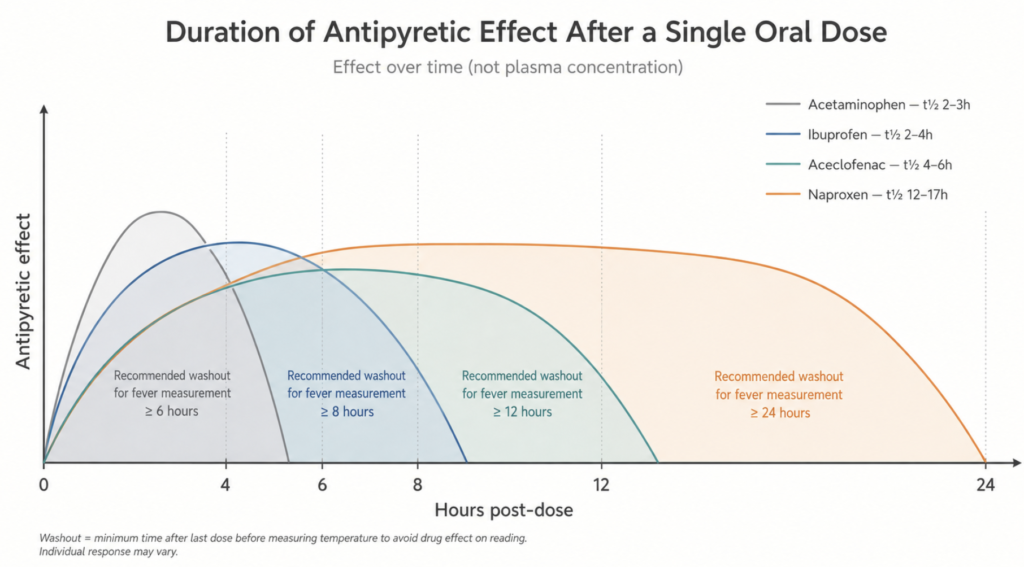
The half-lives are short. Acetaminophen has a plasma half-life of about 2–3 hours in adults; ibuprofen, 1.5–3 hours; naproxen, 12–17 hours; aceclofenac, around 4 hours.
The antipyretic effect, however, outlasts the plasma curve. Pharmacodynamic studies in febrile children show that ibuprofen’s effect-compartment half-life is about 1.1 hours, but the temperature decrement persists with a peak 1–3 hours after peak plasma concentration and a clinically meaningful effect lasting 6–8 hours [Kelley, Effect of age on ibuprofen pharmacokinetics and antipyretic response, J Pediatr 1992]. Acetaminophen’s antipyretic effect typically lasts 4–6 hours, consistent with its recommended q4–6h dosing. Naproxen’s effect spans roughly 12 hours, justifying twice-daily administration.
Combination dosing extends the apyretic window. In a randomised, double-blind pilot trial of single-dose alternating therapy (ibuprofen followed by acetaminophen four hours later), children in the intervention arm spent 7.4 hours fever-free versus 5.7 hours with ibuprofen monotherapy, with the difference accentuated between the sixth and eighth hours after the first dose [Nabulsi, BMC Med 2006]. The Cochrane review found similarly extended time-without-fever with alternating regimens.
Clinical Perspective. Dosing intervals are pharmacodynamic, not pharmacokinetic. A drug whose plasma half-life is two hours can still suppress fever for six. The interval reflects how long the effect lasts in the relevant tissue compartment, not when the molecule has left the bloodstream.
Washout before a fever workup — the only practical question
This is where pharmacology meets clinical reality. If a patient presents to the emergency department with a fever that has been suppressed by a recent antipyretic, three questions overlap: when is the antipyretic effect gone, when is the drug eliminated, and when does the residual matter clinically?
Pharmacodynamics gives the answer for the first question. The clinical antipyretic effect of acetaminophen wanes at roughly 4–6 hours, ibuprofen at 6–8 hours, and naproxen at 12–24 hours. To measure a temperature uninfluenced by antipyretic action, a reasonable minimum washout is one full pharmacodynamic dosing interval beyond the last dose — approximately 6 hours for acetaminophen, 8 hours for ibuprofen and short-acting NSAIDs, and 24 hours for naproxen and other long-half-life agents (piroxicam, meloxicam) [Wong, Cochrane 2013; Kelley, J Pediatr 1992; PharmGKB summary, ibuprofen pathways, Pharmacogenet Genomics 2015].
| Antipyretic | Plasma t½ | Antipyretic duration | Recommended washout for fever measurement |
|---|---|---|---|
| Acetaminophen | 2–3 h | 4–6 h | ≥6 h |
| Ibuprofen | 1.5–3 h | 6–8 h | ≥8 h |
| Aceclofenac | ~4 h | 8–12 h | ≥12 h |
| Naproxen | 12–17 h | 12–24 h | ≥24 h |
| Piroxicam / Meloxicam | 20–50 h | 24+ h | ≥48 h |
Washout reflects pharmacodynamic effect duration in the relevant tissue compartment, not complete drug elimination (4–5 half-lives). In routine outpatient evaluation, recording the timing of the last dose and interpreting the temperature accordingly is often a more practical approach than enforcing a full washout — especially for long-acting NSAIDs like naproxen.
Pharmacokinetics gives the answer for the second question. Four to five half-lives are required for essentially complete elimination — 10–15 hours for acetaminophen and ibuprofen, 60–85 hours for naproxen.
The third question is the one that actually drives clinical decisions, and the answer depends on the context. In a routine outpatient evaluation of a febrile child or adult, the temperature reading is one data point among many; a recently dosed antipyretic blunts but does not erase the diagnostic picture, especially when combined with heart rate, respiratory rate, mental status, and inflammatory markers. In high-risk contexts the principle inverts. Expert consensus cautions against antipyretic use in neutropenic patients because fever is the principal — sometimes the only — sign of bacteraemia, and masking it delays the empirical antibiotics that the IDSA guideline requires within one hour of febrile presentation [Freifeld, Clin Infect Dis 2011]. The same logic applies to suspected sepsis evaluations, post-operative fever pattern analysis, and any situation in which the temperature curve itself is part of the diagnosis.
For a patient who calls ahead before a hospital visit, the practical guidance reduces to one line: if the workup depends on a true temperature, the next antipyretic dose can be skipped and at least one full dosing interval allowed to pass — 6 hours for paracetamol, 8 hours for ibuprofen, longer for naproxen. When comfort takes priority, treating it and recording the timing and identity of the last dose for the clinician is the appropriate trade-off.
Clinical Perspective. A temperature reading taken under the cover of a recent antipyretic is not useless; it is annotated. The clinical mistake is not measuring the temperature too soon — it is forgetting to ask when the last dose was given. The drug history is part of the vital sign.
Key Takeaways
- Acetaminophen and NSAIDs act on different compartments — central versus peripheral — and the practical consequence is that acetaminophen treats discomfort and fever, while NSAIDs additionally treat inflammation.
- The combination is genuinely additive for acute pain, with one of the best NNTs in the Cochrane analgesic catalogue; for fever, the marginal benefit over monotherapy is roughly a quarter of a degree.
- The two drugs do not share a toxicity organ — acetaminophen damages the liver, NSAIDs damage the gut, kidneys, and arteries — and short-term combination does not generate new adverse events, but each drug’s individual ceiling still applies.
- Antipyretic effect outlasts plasma half-life: acetaminophen 4–6 hours, ibuprofen 6–8 hours, naproxen 12–24 hours.
- A minimum washout for an uninfluenced temperature reading is one full pharmacodynamic dosing interval — 6 hours for paracetamol, 8 hours for short-acting NSAIDs, 24 hours for naproxen — though in routine evaluations a recent dose blunts rather than erases the diagnostic picture.
FAQ
Is taking acetaminophen and ibuprofen together safer or more dangerous than taking them apart?
Neither, in the short term. Cochrane single-dose data show no increase in adverse events with the combination compared with monotherapy, and serious events occur in roughly 1 in 3,200 participants [Moore, Cochrane 2015]. The two drugs damage different organs, so they do not compound a single risk; each individual ceiling still applies.
Does combining the two drugs work better than either alone?
Yes for acute pain, modestly for fever. The combination gives one of the best NNTs in the Cochrane single-dose analgesic database for postoperative pain (NNT 1.5–1.6) [Derry, Cochrane 2013]. For pediatric fever, the combination lowers mean temperature by about 0.27–0.29 °C more than monotherapy at one hour, and prolongs the time spent afebrile [Wong, Cochrane 2013; Trippella, Front Pediatr 2019].
How long should I wait after a dose of antipyretic before going to the hospital for a fever workup?
At least one full pharmacodynamic dosing interval: approximately 6 hours for acetaminophen, 8 hours for ibuprofen and other short-acting NSAIDs, and 24 hours for naproxen [Kelley, J Pediatr 1992; PharmGKB, Pharmacogenet Genomics 2015]. In routine outpatient settings the timing of the last dose is often more useful than a strict washout, because the diagnostic picture is rarely built on temperature alone. In contexts where fever is itself the diagnosis — neutropenic patients, suspected sepsis — expert consensus is to avoid antipyretics altogether [Freifeld, Clin Infect Dis 2011].
Which drug is “stronger”?
For pediatric fever, ibuprofen lowers temperature slightly faster and slightly more than acetaminophen, but the difference is small and both are recommended as first-line [Wong, Cochrane 2013]. For acute postoperative pain in adults, ibuprofen has a lower NNT than paracetamol at standard doses, and the combination beats either alone [Moore, Cochrane 2015].
References
- Coxib and Traditional NSAID Trialists’ (CNT) Collaboration. Vascular and upper gastrointestinal effects of non-steroidal anti-inflammatory drugs: meta-analyses of individual participant data from randomised trials. Lancet. 2013;382(9894):769-779.
- Derry C, Derry S, Moore RA, McQuay HJ. Single dose oral ibuprofen for acute postoperative pain in adults. Cochrane Database Syst Rev. 2009;(3):CD001548.
- Derry CJ, Derry S, Moore RA. Single dose oral ibuprofen plus paracetamol (acetaminophen) for acute postoperative pain. Cochrane Database Syst Rev. 2013;(6):CD010210.
- Freifeld AG, Bow EJ, Sepkowitz KA, et al. Clinical practice guideline for the use of antimicrobial agents in neutropenic patients with cancer: 2010 update by the Infectious Diseases Society of America. Clin Infect Dis. 2011;52(4):e56-e93.
- Hinz B, Cheremina O, Brune K. Acetaminophen (paracetamol) is a selective cyclooxygenase-2 inhibitor in man. FASEB J. 2008;22(2):383-390.
- Kelley MT, Walson PD, Edge JH, Cox S, Mortensen ME. Pharmacokinetics and pharmacodynamics of ibuprofen isomers and acetaminophen in febrile children. Clin Pharmacol Ther. 1992;52(2):181-189.
- LiverTox: Clinical and Research Information on Drug-Induced Liver Injury. Acetaminophen. Bethesda (MD): National Institute of Diabetes and Digestive and Kidney Diseases; 2012-. Updated 28 January 2016.
- Mazaleuskaya LL, Theken KN, Gong L, et al. PharmGKB summary: ibuprofen pathways. Pharmacogenet Genomics. 2015;25(2):96-106.
- Moore RA, Derry S, Aldington D, Wiffen PJ. Single dose oral analgesics for acute postoperative pain in adults — an overview of Cochrane reviews. Cochrane Database Syst Rev. 2015;(9):CD008659.
- Moore RA, Derry S, McQuay HJ, Wiffen PJ. Adverse events associated with single dose oral analgesics for acute postoperative pain in adults — an overview of Cochrane reviews. Cochrane Database Syst Rev. 2015;(10):CD011407.
- Moore RA, Derry CJ, Derry S, Straube S, McQuay HJ. A conservative method of testing whether combination analgesics produce additive or synergistic effects using evidence from acute pain and migraine. Eur J Pain. 2012;16(4):585-591.
- Nabulsi MM, Tamim H, Mahfoud Z, et al. Alternating ibuprofen and acetaminophen in the treatment of febrile children: a pilot study (ISRCTN30487061). BMC Med. 2006;4:4.
- Ohashi N, Kohno T. Analgesic Effect of Acetaminophen: A Review of Known and Novel Mechanisms of Action. Front Pharmacol. 2020;11:580289.
- Tawfik M, Almousawi N, Yacout M, et al. Nonsteroidal Anti-Inflammatory Drugs and Risk of Gastrointestinal Bleeding: A Systematic Review and Meta-Analysis. Clin Pharmacol Ther. 2025. Online ahead of print.
- Toms L, McQuay HJ, Derry S, Moore RA. Single dose oral paracetamol (acetaminophen) for postoperative pain in adults. Cochrane Database Syst Rev. 2008;(4):CD004602.
- Trippella G, Ciarcià M, de Martino M, Chiappini E. Prescribing Controversies: An Updated Review and Meta-Analysis on Combined/Alternating Use of Ibuprofen and Paracetamol in Febrile Children. Front Pediatr. 2019;7:217.
- Watkins PB, Kaplowitz N, Slattery JT, et al. Aminotransferase elevations in healthy adults receiving 4 grams of acetaminophen daily: a randomized controlled trial. JAMA. 2006;296(1):87-93.
- Wong T, Stang AS, Ganshorn H, et al. Combined and alternating paracetamol and ibuprofen therapy for febrile children. Cochrane Database Syst Rev. 2013;(10):CD009572.
Joonpyo Hong, MD is a board-certified otolaryngologist practicing in Korea. This article reflects his clinical interpretation of published research and does not constitute individual medical advice.