
A patient walks in with constant throat clearing, a lump sensation, and morning hoarseness — the classic picture of silent reflux. No heartburn, no acid taste. The laryngoscopy shows mild erythema and some posterior commissure thickening — borderline. The clinical reflex is to start a proton pump inhibitor (PPI) and reassess in eight weeks.
This scenario plays out hundreds of times a day in ENT clinics. It also exposes three uncomfortable truths about laryngopharyngeal reflux disease (LPRD): it is not the same as gastroesophageal reflux disease (GERD), the endoscopic score we rely on is less reliable than textbooks claim, and the medication we routinely prescribe may not work much better than placebo in randomized trials. This article walks through each of those points, with the evidence behind them.
1. LPR and GERD Share a Mechanism, Not a Disease
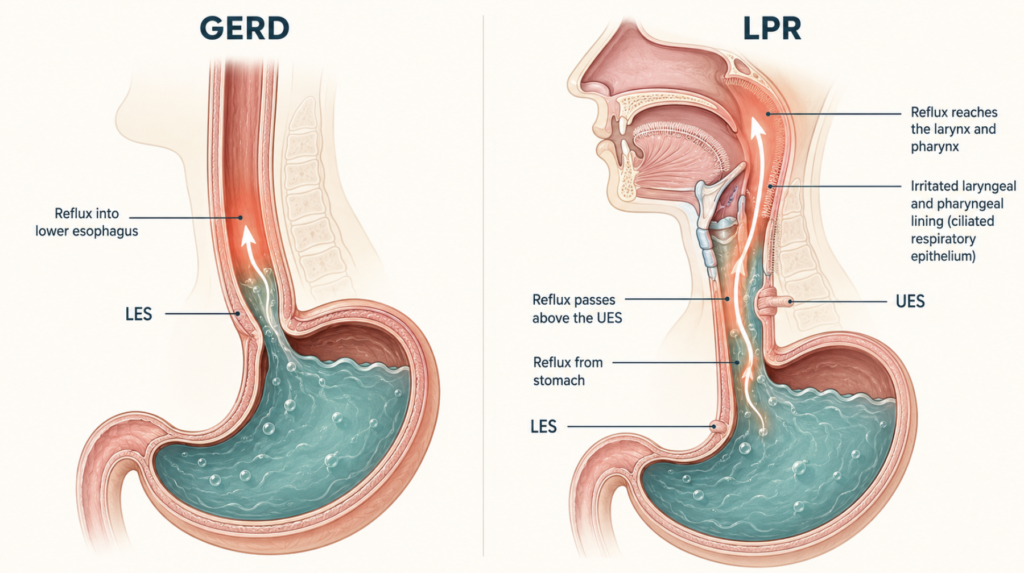
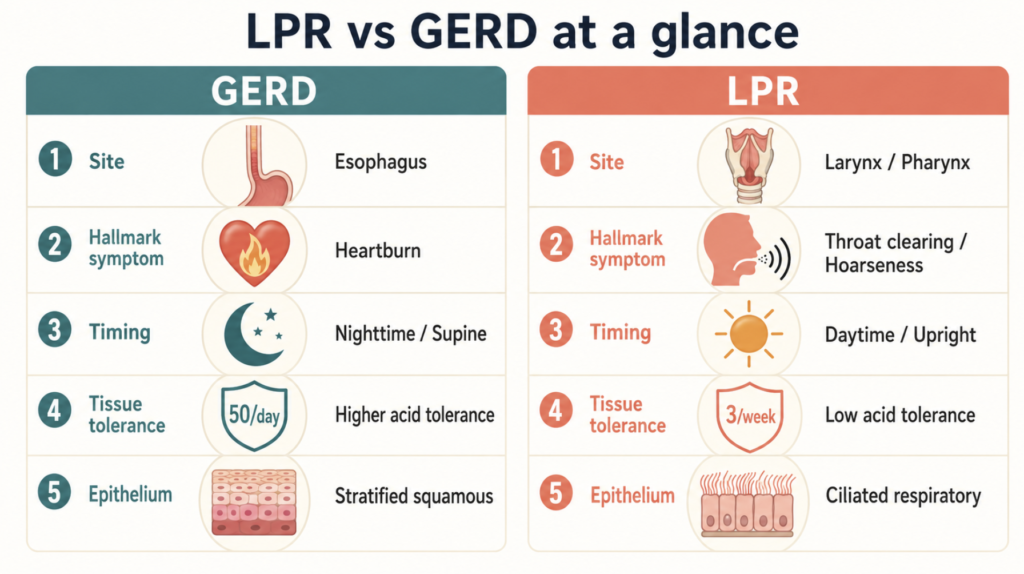
GERD is the reflux of gastric contents past a dysfunctional lower esophageal sphincter (LES) into the esophagus, producing heartburn in more than 80% of patients. LPR is the reflux of gastric contents past the upper esophageal sphincter (UES) into the larynx and pharynx. Heartburn is present in only about 20% of LPR cases, which is why the condition is often called “silent reflux.”
The symptom patterns diverge for a reason. GERD typically occurs supine and at night; LPR occurs upright and during the day. GERD usually leaves visible esophagitis; LPR often shows only subtle laryngeal findings or none at all. Many patients have both, but the Wang et al. synchronous pH-impedance study (Wang L, Otolaryngology–Head and Neck Surgery, 2020) found that 61% of LPR patients had isolated LPR without coexisting GERD, suggesting LPR is not simply “GERD that went higher.”
Why the Larynx Is So Vulnerable
This is the part of the story that most patient-facing articles skip, and it changes how you should think about the disease.
The esophagus is lined with stratified squamous epithelium — abrasion-resistant, with built-in clearance from peristalsis and saliva. The larynx is lined with ciliated respiratory epithelium, far more fragile and without any saliva rinse. The esophagus also expresses defensive proteins like carbonic anhydrase III that buffer acid at the cellular level; these are markedly depleted in the laryngeal epithelium of LPR patients (Johnston N, Pepsin and carbonic anhydrase isoenzyme III as diagnostic markers for laryngopharyngeal reflux disease, 2004).
The clinical consequence of this asymmetry is striking. The esophagus can tolerate up to roughly 50 reflux episodes per day without damage. In the canine model originally published by Koufman, as few as three acid-and-pepsin exposures per week were enough to produce severe laryngeal injury when prior mucosal injury was present (Koufman JA, The otolaryngologic manifestations of gastroesophageal reflux disease (GERD), 1991). This finding was later codified in the American Academy of Otolaryngology–Head and Neck Surgery position statement (Koufman JA, Laryngopharyngeal reflux: position statement of the committee on speech, voice, and swallowing disorders of the AAO-HNS, 2002) and was further replicated by Adhami’s beagle study (Adhami T, The role of gastric and duodenal agents in laryngeal injury: an experimental canine model, 2004), which additionally showed that pepsin alone or combined with bile acids caused the most severe inflammation. An ex vivo study on laryngeal tissue made the implication explicit: laryngeal tissue is essentially resistant to damage at pH 4.0 on its own, but pepsin makes the same refluxate damaging at that pH (Bulmer DM, Laryngeal mucosa: its susceptibility to damage by acid and pepsin, 2010).
Clinical implication: A negative upper GI endoscopy does not rule out LPR. Patients with “only a little” reflux on pH testing can still have substantial laryngeal symptoms because the threshold for laryngeal injury is an order of magnitude lower than for the esophagus.
LPR vs GERD at a glance
2. The Reflux Finding Score: Useful, But Don’t Over-Trust It
The Reflux Finding Score (RFS) was introduced by Belafsky in 2001 as a way to quantify endoscopic findings of LPR. It scores eight items on laryngoscopy:
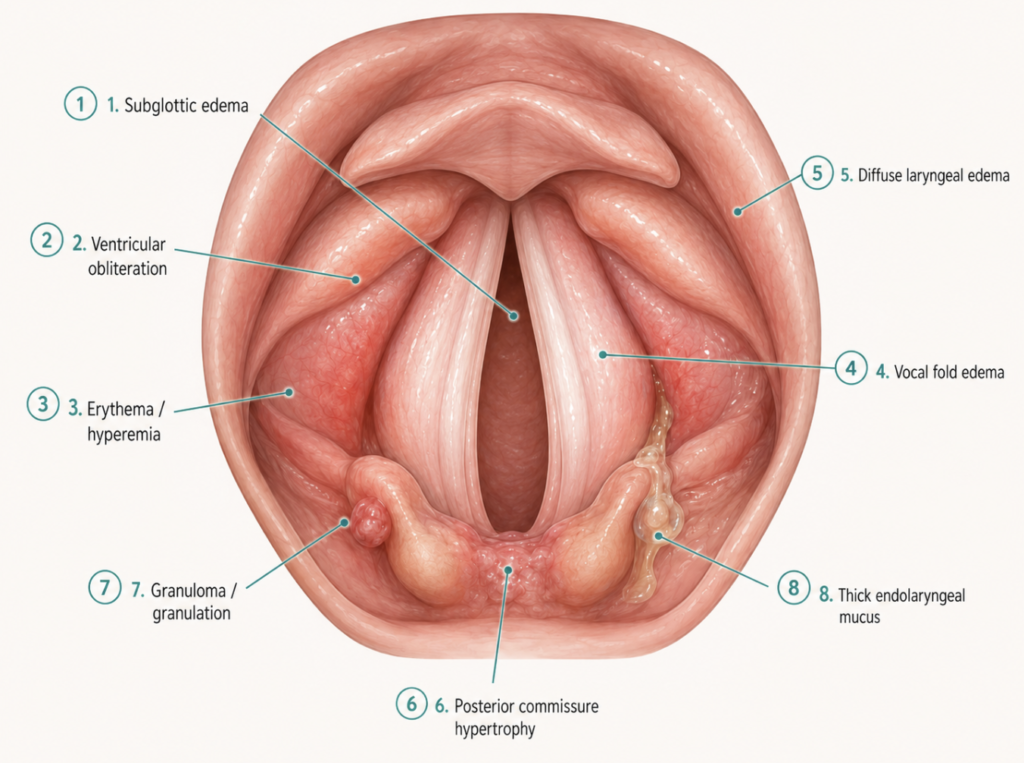
- Subglottic edema (0 or 2)
- Ventricular obliteration (0, 2, or 4)
- Erythema or hyperemia (0, 2, or 4)
- Vocal fold edema (0–4)
- Diffuse laryngeal edema (0–4)
- Posterior commissure hypertrophy (0–4)
- Granuloma or granulation tissue (0 or 2)
- Thick endolaryngeal mucus (0 or 2)
The original Belafsky paper reported a total score above 7 as having a 95% probability of indicating LPR, with an interobserver correlation coefficient above 0.90 between two laryngologists (Belafsky PC, The validity and reliability of the reflux finding score (RFS), 2001).
That number — 0.90 — became gospel. The problem is that it has not held up well in larger, more rigorous replication.
What the 2020 reliability study found
A more recent investigation enrolled 92 patients with LPR who had undergone both stroboscopy and 24-hour pH-impedance testing within 30 days, and asked four blinded observers of varying experience levels (a resident, two laryngology fellows, and an attending laryngologist) to score the RFS independently (Vance D, The Validity and Reliability of the Reflux Finding Score, 2023, J Voice).
The results were uncomfortable:
- Kappa between reviewers was 0.479 — fair to substantial, not excellent.
- Total RFS showed no correlation with any parameter of 24-hour pH-impedance testing.
- The most subjective items had the worst per-item agreement: vocal fold edema at 52.5%, posterior commissure hypertrophy at 52.5%, and thick endolaryngeal mucus at 55%.
In other words, the score most ENTs were taught to trust correlates with neither objective acid exposure nor consistent inter-rater interpretation. Some items — granuloma identification, for example — were nearly perfect at 96.8% agreement. But the inflammation-based scores that drive most clinical decisions are the least reliable.
Clinical perspective: RFS still has value, but for the right purpose. It is genuinely useful for tracking a single patient over time when scored by the same clinician. It is weak as a standalone diagnostic threshold. Treating an RFS of 8 as proof of LPR is overreaching the evidence.
3. PPIs for LPR: What the Evidence Actually Says
If the diagnosis is uncertain and the standard treatment works, the diagnostic uncertainty is forgivable. The trouble is that the standard treatment also has shakier evidence than most clinic conversations imply.
The meta-analyses
Four major meta-analyses have tried to answer whether PPIs help patients with LPR more than placebo:
- Liu et al. (2016), 8 RCTs, 370 patients: PPI vs placebo overall symptom improvement was not statistically significant (RR=1.22; 95%CI 0.93–1.58; p=0.149). Cough improvement also nonsignificant (Liu C, Meta-analysis of the efficacy of proton pump inhibitors for the symptoms of laryngopharyngeal reflux, 2016).
- Guo et al. (2016), 14 RCTs, 771 patients: modest response advantage for PPI (RD=0.15; 95%CI 0.01–0.30) and significantly improved total Reflux Symptom Index, but no advantage in Reflux Finding Score (Guo H, Proton pump inhibitor therapy for the treatment of laryngopharyngeal reflux: a meta-analysis of randomized controlled trials, 2016).
- Wei (2016), 13 RCTs, 831 patients: PPI significantly improved total RSI but no significant difference in response rate or RFS (Wei C, A meta-analysis for the role of proton pump inhibitor therapy in patients with laryngopharyngeal reflux, 2016).
- Jin et al. (2022): PPI improved RSI versus placebo, but overall efficacy was not statistically significantly different from placebo (OR=1.62; 95%CI 0.89–2.95; p>0.05) (Jin X, Meta-analysis of Proton Pump Inhibitors in the Treatment of Pharyngeal Reflux Disease, 2022).
The pattern is consistent: symptoms improve modestly, objective findings rarely do, and the placebo effect is large.
Why is it so hard to show PPI works?
The most likely explanation is that LPR is not a single-pathway disease. Acid suppression is one lever, but LPR has several gears:
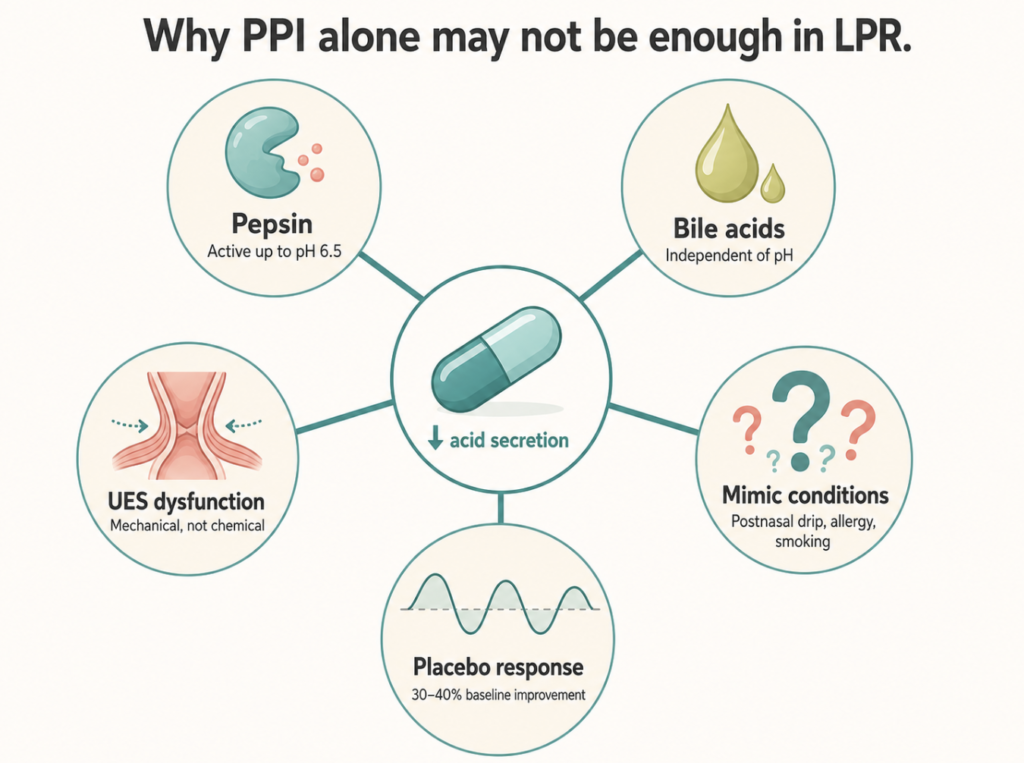
- Pepsin remains active up to about pH 6.5. PPIs raise gastric pH but do not remove the pepsin already deposited on laryngeal tissue, where it disrupts E-cadherin, activates inflammatory signaling, and damages epithelial barrier function (Bulmer DM, Laryngeal mucosa: its susceptibility to damage by acid and pepsin, 2010).
- Bile acids in duodenogastric reflux cause injury independently of pH, and PPIs do not address them.
- UES dysfunction is a mechanical problem. No amount of acid suppression repairs a leaky valve.
- Mimic conditions — postnasal drip, allergic rhinitis, smoking, vocal misuse, and inhaled corticosteroid effects — can produce identical symptoms and confound trials.
- Placebo response rates of 30–40% in LPR trials reflect the naturally fluctuating course of throat symptoms.
Put another way: a clinical trial of PPIs in LPR is testing whether one intervention can fix a problem driven by at least five mechanisms, while the control arm captures one-third of patients who would have improved anyway.
Empirical PPI trial vs investigate first?
The two strategies have different logics, and the empirical approach has real merit. An empirical 8–12 week twice-daily PPI trial is cheap, low-risk, widely available, and treats the single most modifiable contributor to LPR. For the patient population where reflux truly is the driver, it works — and it works without subjecting every globus or hoarseness patient to invasive pH-impedance monitoring upfront. Cost-effectiveness studies consistently support this as a sensible first move in most clinical settings.
The problem is not the empirical trial itself; it is what happens next. When de Bortoli and colleagues took 41 consecutive patients with a laryngoscopic diagnosis of LPR and put them through 24-hour multichannel impedance-pH testing after PPI washout, GERD was confirmed in fewer than 40% of cases, meaning over 60% of patients labeled clinically as LPR had no objective reflux to support the diagnosis (de Bortoli N, How many cases of laryngopharyngeal reflux suspected by laryngoscopy are gastroesophageal reflux disease-related?, 2012).
That is a substantial fraction of empirical PPI prescriptions treating the wrong target. The implication is not that empirical PPI is wrong — it remains a reasonable opening move — but that continuing or escalating PPI past the defined 8–12 week trial window without reassessment is hard to justify.
Clinical perspective: An empirical 8–12 week PPI trial is a reasonable and cost-effective first move, especially when lifestyle modifications are introduced simultaneously and a stop-and-reassess date is set at the outset. What is rarely justified is continuing or escalating the PPI dose past 8–12 weeks in a patient who has not improved. At that point, the answer is almost never “more PPI”; it is to reconsider the diagnosis, add an alginate or mucosal protectant to target nonacidic reflux components, or pursue pH-impedance testing.
4. What the Honest Conversation Sounds Like
A few things tend to be true about LPR that clinics underemphasize:
- It is genuinely overdiagnosed in ENT clinics, but it is also a real condition with measurable pepsin-mediated tissue damage. Both extremes — “everyone’s symptoms are reflux” and “LPR is not a real disease” — are wrong.
- The single most underused intervention is alginate, which forms a physical raft on top of gastric contents and can block weakly acidic and nonacidic reflux that PPIs miss. A 2025 systematic review of 14 controlled studies found that the alginate-PPI combination yielded greater symptom improvement than PPI monotherapy, although the authors emphasized that the small number of studies and substantial heterogeneity preclude definitive conclusions and that further randomized trials are needed (Lechien JR, Treatment for Laryngopharyngeal Reflux Disease: A Systematic Review of Controlled Studies, 2025).
- The single most under-explained intervention is lifestyle modification. Avoiding meals within three hours of sleep, elevating the head of the bed, reducing alcohol and caffeine, losing weight if overweight, and stopping smoking address the mechanical and triggering factors that PPIs simply cannot reach.
- A patient on PPI longer than 8–12 weeks without symptom change deserves a fresh look, not a dose increase.
Key Takeaways
- LPR and GERD share a mechanism but differ in anatomic site, symptom pattern, and tissue vulnerability — the laryngeal epithelium can be damaged by as few as three reflux episodes per week, whereas the esophagus tolerates roughly fifty per day.
- The Reflux Finding Score has only fair-to-substantial interrater reliability and does not correlate with 24-hour pH-impedance testing in the most rigorous study to date.
- Meta-analyses consistently show PPIs improve LPR symptoms modestly but rarely outperform placebo on objective endpoints like the Reflux Finding Score.
- LPR is multifactorial — pepsin, bile, UES dysfunction, and mimic conditions all bypass acid suppression — which explains why a single-target drug performs unevenly.
- An empirical 8–12 week PPI trial is a reasonable and cost-effective first-line strategy, but continuing PPI beyond that window without improvement is rarely the right answer.
Frequently Asked Questions
How is LPR different from GERD?
LPR affects the larynx and pharynx and usually causes throat clearing, globus, and hoarseness without heartburn. GERD affects the esophagus and typically causes heartburn and chest discomfort. They can coexist, but most LPR patients (about 60%) have no concurrent GERD.
Can a doctor diagnose LPR from a laryngoscopy alone?
Not reliably. The Reflux Finding Score is the most commonly used endoscopic scoring system, but recent research shows it has fair-to-substantial reliability between observers and no correlation with objective 24-hour pH testing. It is more useful for tracking change in one patient over time than for confirming a new diagnosis.
Why isn’t my PPI working for silent reflux?
PPIs reduce acid but do not eliminate pepsin, which damages laryngeal tissue even in weakly acidic or nonacidic reflux. PPIs also do not address bile reflux, mechanical sphincter weakness, or the conditions that mimic LPR like postnasal drip and allergy. This is why up to half of LPR patients do not respond to PPIs alone.
Should I get a pH test before starting a PPI?
Most clinicians start with an empirical 8–12 week PPI trial because it is cheap and low-risk. If symptoms have not meaningfully improved by that point, pH-impedance testing becomes clinically useful, because in one study fewer than 40% of patients clinically diagnosed with LPR by laryngoscopy had reflux confirmed on objective testing.
What can I do besides medication?
Avoid eating within three hours of lying down, elevate the head of the bed, lose weight if overweight, reduce alcohol and caffeine, and stop smoking. These address the mechanical and triggering factors that medication cannot reach, and for many patients they outperform the PPI in long-term outcome.
References
- Adhami T, Goldblum JR, Richter JE, Vaezi MF. The role of gastric and duodenal agents in laryngeal injury: an experimental canine model. Am J Gastroenterol. 2004;99(11):2098-2106.
- Belafsky PC, Postma GN, Koufman JA. The validity and reliability of the reflux finding score (RFS). Laryngoscope. 2001;111(8):1313-1317.
- Bulmer DM, Ali MS, Brownlee IA, Dettmar PW, Pearson JP. Laryngeal mucosa: its susceptibility to damage by acid and pepsin. Laryngoscope. 2010;120(4):777-782.
- de Bortoli N, Nacci A, Savarino E, Martinucci I, Bellini M, Fattori B, Ceccarelli L, Costa F, Mumolo MG, Ricchiuti A, Savarino V, Berrettini S, Marchi S. How many cases of laryngopharyngeal reflux suspected by laryngoscopy are gastroesophageal reflux disease-related? World J Gastroenterol. 2012;18(32):4363-4370.
- Guo H, Ma H, Wang J. Proton pump inhibitor therapy for the treatment of laryngopharyngeal reflux: a meta-analysis of randomized controlled trials. J Clin Gastroenterol. 2016;50(4):295-300.
- Jin X, Zhou X, Fan Z, Qin Y, Zhan J. Meta-analysis of Proton Pump Inhibitors in the Treatment of Pharyngeal Reflux Disease. Comput Math Methods Med. 2022;2022:9105814.
- Johnston N, Knight J, Dettmar PW, Lively MO, Koufman J. Pepsin and carbonic anhydrase isoenzyme III as diagnostic markers for laryngopharyngeal reflux disease. Laryngoscope. 2004;114(12):2129-2134.
- Koufman JA. The otolaryngologic manifestations of gastroesophageal reflux disease (GERD): a clinical investigation of 225 patients using ambulatory 24-hour pH monitoring and an experimental investigation of the role of acid and pepsin in the development of laryngeal injury. Laryngoscope. 1991;101(4 Pt 2 Suppl 53):1-78.
- Koufman JA, Aviv JE, Casiano RR, Shaw GY. Laryngopharyngeal reflux: position statement of the committee on speech, voice, and swallowing disorders of the American Academy of Otolaryngology-Head and Neck Surgery. Otolaryngol Head Neck Surg. 2002;127(1):32-35.
- Lechien JR. Treatment for Laryngopharyngeal Reflux Disease: A Systematic Review of Controlled Studies. J Otolaryngol Head Neck Surg. 2025;54:19160216251347602.
- Liu C, Wang H, Liu K. Meta-analysis of the efficacy of proton pump inhibitors for the symptoms of laryngopharyngeal reflux. Braz J Med Biol Res. 2016;49(7):e5149.
- Vance D, Alnouri G, Shah P, O’Connell Ferster AP, Lyons K, Ross J, Sataloff RT. The Validity and Reliability of the Reflux Finding Score. J Voice. 2023;37(1):92-96.
- Wang L, Wang G, Li L, Fan X, Liu H, Sun Z, Han H, Li B, Ding R, Wu W. Relationship between laryngopharyngeal reflux disease and gastroesophageal reflux disease based on synchronous esophageal and oropharyngeal Dx-pH monitoring. Am J Otolaryngol. 2020;41(4):102441.
- Wei C. A meta-analysis for the role of proton pump inhibitor therapy in patients with laryngopharyngeal reflux. Eur Arch Otorhinolaryngol. 2016;273(11):3795-3801.
Joonpyo Hong, MD is a board-certified otolaryngologist practicing in Korea. This article reflects his clinical interpretation of published research and does not constitute individual medical advice.
For more interesting contents:
https://curiousmd.com/cnn-laryngeal-cancer-diagnosis/
https://curiousmd.com/hpv-vocal-cord-cancer-young-non-smokers/
https://curiousmd.com/cough-that-wont-go-away-after-a-cold/
Link outu to:
AAO-HNS Position Statement: Laryngopharyngeal Reflux:
https://www.entnet.org/resource/position-statement-laryngopharyngeal-reflux/
AGA Clinical Practice Update on Extraesophageal GERD (2023, open access):
https://www.cghjournal.org/article/S1542-3565(23)00143-X/fulltext
Lechien JR 2025 Systematic Review (alginate–PPI):
https://journals.sagepub.com/doi/10.1177/19160216251347602