A newborn falls asleep through REM. An adult falls asleep through NREM. Sleep cycles by age start with this single inversion — present at birth, gone by six months — and the differences only grow from there, shaping nearly everything that changes about sleep across the lifespan.
Most articles about sleep development stop at infancy or pick up at adulthood. This one walks the full arc — newborn, infant, toddler, school-age child, adolescent, adult — and ends with where ENT clinics see things go wrong.
The Three Variables That Change With Age
Three things shift across the lifespan: sleep cycle length, REM-to-NREM ratio, and circadian rhythm.
A sleep cycle is one round trip through the stages of sleep. In adults, that round trip averages about 90 minutes; in newborns, it’s roughly half that [Lenehan, Maternal Child Health Journal, 2023].
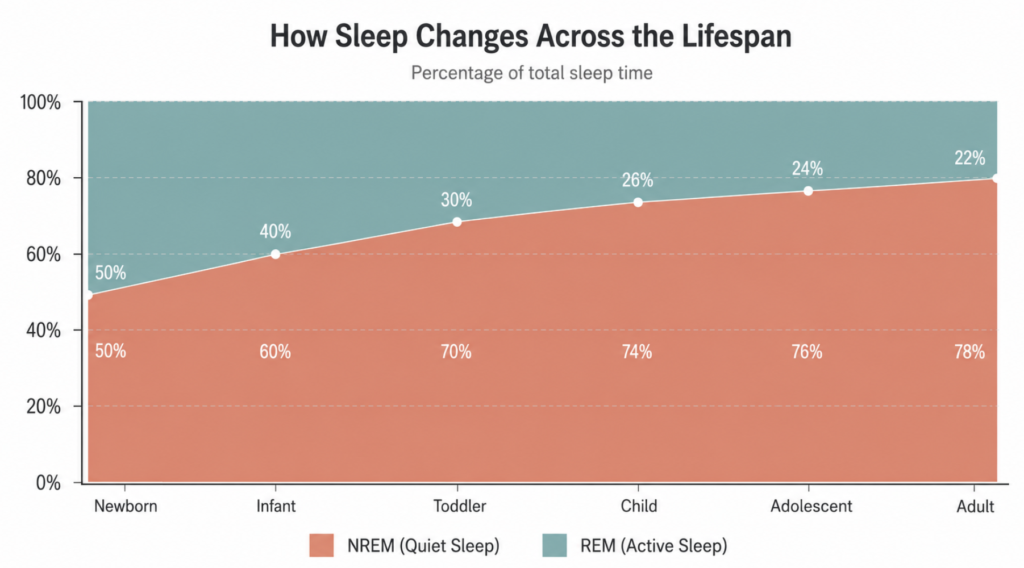
REM and NREM serve different jobs. REM (active sleep, in newborn terminology) supports neural plasticity and is thought to drive much of the rapid brain wiring that happens before age 2. NREM — particularly slow-wave sleep — supports synaptic homeostasis and physical growth. The balance between them is not fixed; it’s age-graded.
Circadian rhythm, the internal 24-hour clock, is not present at birth. Newborns operate on a feeding-driven ultradian rhythm (roughly 3 hours per cycle) and only develop day-night entrainment around 4–6 weeks postnatally [Lenehan, Maternal Child Health Journal, 2023].
Sleep Architecture by Age — The Comparison
| Age group | Total daily sleep | Cycle length | REM share | Defining feature |
|---|---|---|---|---|
| Newborn (0–1 mo) | 14–17 hours | 45–60 min | ~50% | Sleep onset through REM; no circadian rhythm |
| Infant (1–12 mo) | 12–16 hours | 50–60 min | 30–40% | NREM stages emerge at 2–3 mo; NREM-onset by ~6 mo |
| Toddler (1–3 yr) | 11–14 hours | 60–75 min | ~30% | Naps consolidate to 1–2/day; night terrors begin |
| Child (3–12 yr) | 9–12 hours | ~90 min | 20–25% | Adult-like architecture; adenotonsillar peak |
| Adolescent (13–18 yr) | 8–10 hours | ~90 min | ~20–25% | Melatonin onset delays ~2 hours |
| Adult | 7–9 hours | ~90 min | 20–25% | NREM-onset; 4–6 cycles/night |
Sleep duration recommendations follow the American Academy of Sleep Medicine consensus [Paruthi, Journal of Clinical Sleep Medicine, 2016].
Why Newborns Enter REM First
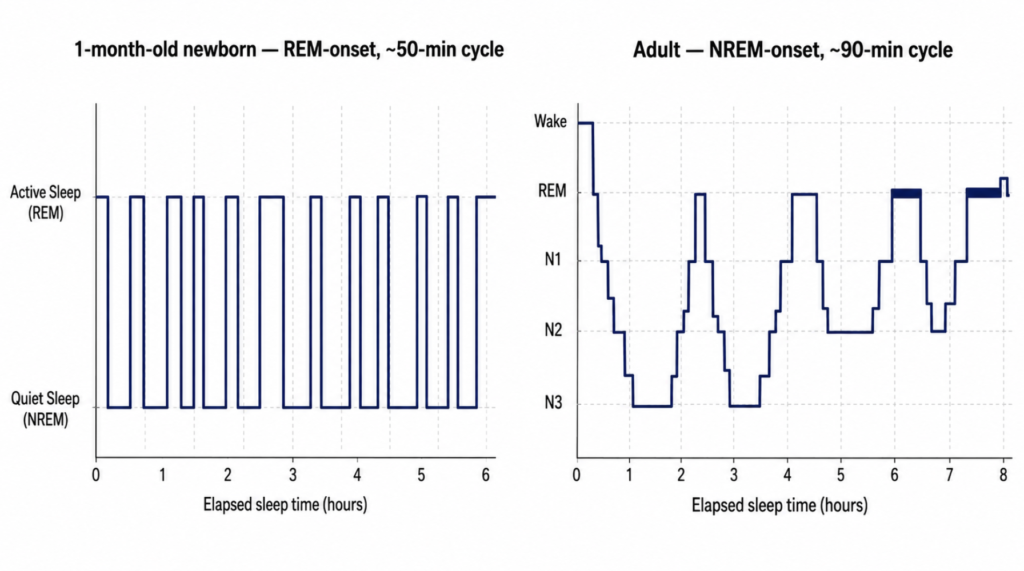
In newborns, sleep is divided into three categories: active sleep (the precursor to REM), quiet sleep (precursor to NREM), and indeterminate sleep. Sleep onset occurs through active sleep, and roughly half of total sleep is spent there [Lenehan, Maternal Child Health Journal, 2023]. This pattern is the opposite of mature sleep and likely reflects the dominance of brainstem-driven REM machinery before higher cortical networks come online.
Because each cycle is short (about 50 minutes) and ends in light sleep, newborns surface to near-waking many times per night. This is normal physiology, not a sleep problem.
The “4-Month Sleep Regression” Is Maturation, Not Regression
Around 3–4 months, the four-stage NREM architecture begins to appear, sleep spindles and K-complexes emerge on EEG, and sleep onset starts shifting from active to quiet sleep. By six months, most infants have transitioned to NREM-onset sleep, and the architecture closely resembles an adult’s [Lenehan, Maternal Child Health Journal, 2023].
What parents experience as “regression” — more frequent awakenings, harder bedtimes — coincides with this reorganization. The system isn’t breaking down; it’s rewiring.
Toddler and Child Sleep: Stabilization
Between ages 1 and 5, daytime sleep consolidates. Most children drop their morning nap around 12–18 months and the afternoon nap by age 4–5. Total sleep gradually drops from about 14 hours at age 1 to around 10–11 hours by age 6.
Cycle length elongates steadily and reaches the adult 90-minute range by school age. NREM slow-wave activity peaks around mid-childhood and then declines through adolescence — a curve that maps strikingly well onto cortical gray matter pruning, which has driven the hypothesis that deep sleep supports synaptic refinement during this window.
The Adolescent Shift Is Biological, Not Behavioral
The most common clinical misunderstanding about teenage sleep is that it’s a lifestyle problem. The biology says otherwise.
At puberty, the timing of dim light melatonin onset (DLMO) — the internal signal that says “begin night” — shifts roughly 2 hours later [Crowley, Sleep Medicine, 2007]. Adolescents also accumulate sleep pressure more slowly through the evening, meaning they don’t feel sleepy until later. Animal and human studies suggest this is driven by gonadal hormones and altered circadian sensitivity to light, not just by smartphones or school stress [Hagenauer, Developmental Neuroscience, 2009].
Adolescents still need 8–10 hours of sleep [Paruthi, Journal of Clinical Sleep Medicine, 2016]. The collision between a biologically delayed bedtime and an early school start produces chronic sleep restriction in a substantial fraction of the teenage population.
Adult Sleep — and What Happens Beyond
Adult sleep settles into roughly four to six 90-minute cycles per night, starting in NREM. Slow-wave sleep dominates the first third of the night; REM lengthens across the second half. With aging, slow-wave sleep continues to thin out, sleep becomes more fragmented, and circadian phase tends to drift earlier — the opposite of adolescence.
Clinical Perspective — Where the ENT Sees the Damage
The lifespan story above describes normal sleep. In an ENT clinic, the question is what disrupts it.
Pediatric obstructive sleep apnea peaks between ages 2 and 8, driven primarily by adenotonsillar hypertrophy at the very window when tonsil and adenoid tissue is largest relative to the pharyngeal airway. The American Academy of Pediatrics has explicitly identified this as the period of highest risk and recommends that all children who snore be screened for OSA [Marcus, Pediatrics, 2012]. Untreated pediatric OSA disrupts REM-stage breathing in a phase of life when REM still plays a developmental role, and is associated with measurable effects on growth and neurocognition.
Chronic mouth breathing from nasal obstruction — allergic rhinitis, adenoid hypertrophy, septal deviation — flattens slow-wave sleep in children whose architecture is still maturing. Parents often report the surface symptom (snoring, restless sleep, daytime irritability) without recognizing the upstream cause.
In adolescents, the late bedtime is biological, but coexisting OSA from obesity or persistent adenotonsillar tissue can convert “tired teenager” into actual pathology. A teenager who snores loudly and is sleepy at school deserves more than a lecture about screen time.
Key Takeaways
- Newborn sleep cycles are about 45–60 minutes; adult cycles are about 90 minutes.
- REM share drops from roughly 50% at birth to 20–25% by mid-childhood and stays there through adulthood.
- Circadian rhythm is not present at birth — it begins developing around 4–6 weeks.
- The “4-month sleep regression” reflects normal emergence of four-stage NREM architecture, not a sleep problem.
- Adolescent late bedtimes are driven by a ~2-hour delay in melatonin onset at puberty, not laziness.
- Habitual snoring in children is not normal and should prompt evaluation for obstructive sleep apnea.
FAQ
How long is a baby’s sleep cycle? About 45–60 minutes in the first months of life, gradually lengthening across the first year. By age 5, most children have reached the adult cycle length of approximately 90 minutes [Lenehan, Maternal Child Health Journal, 2023].
Is the 4-month sleep regression a real regression? No — it reflects the emergence of the four-stage NREM architecture and the shift from REM-onset to NREM-onset sleep. The system is reorganizing toward maturity, not deteriorating.
Why do teenagers stay up so late? At puberty, the brain’s melatonin release shifts roughly 2 hours later, and homeostatic sleep pressure builds more slowly in the evening [Crowley, Sleep Medicine, 2007]. Biology, not just choice, is moving bedtime later.
Should I be worried if my child snores every night? Yes — habitual snoring in children warrants evaluation. The American Academy of Pediatrics recommends screening any child who snores for obstructive sleep apnea, since untreated pediatric OSA can affect growth and cognition [Marcus, Pediatrics, 2012].
References
- Lenehan SM, Fogarty L, O’Connor C, Mathieson S, Boylan GB. The Architecture of Early Childhood Sleep Over the First Two Years. Matern Child Health J. 2023;27(2):226-250.
- Crowley SJ, Acebo C, Carskadon MA. Sleep, circadian rhythms, and delayed phase in adolescence. Sleep Med. 2007;8(6):602-612.
- Hagenauer MH, Perryman JI, Lee TM, Carskadon MA. Adolescent changes in the homeostatic and circadian regulation of sleep. Dev Neurosci. 2009;31(4):276-284.
- Paruthi S, Brooks LJ, D’Ambrosio C, et al. Recommended Amount of Sleep for Pediatric Populations: A Consensus Statement of the American Academy of Sleep Medicine. J Clin Sleep Med. 2016;12(6):785-786.
- Marcus CL, Brooks LJ, Draper KA, et al. Diagnosis and management of childhood obstructive sleep apnea syndrome. Pediatrics. 2012;130(3):576-584.
Joonpyo Hong, MD is a board-certified otolaryngologist practicing in Korea. This article reflects his clinical interpretation of published research and does not constitute individual medical advice.