
A patient wakes up, stands, and the room is spinning so violently they cannot walk to the bathroom without crawling. The spinning does not stop after a minute, or an hour — it lasts the entire day. There is no hearing loss, no weakness, no slurred speech. This is the classic picture of vestibular neuritis, the third most common peripheral vestibular disorder after BPPV and Ménière disease [Bae, Current diagnosis and treatment of vestibular neuritis: a narrative review, 2021]. This article walks through what causes it, the one question every clinician has to answer first, and what realistic recovery looks like.
What Is Vestibular Neuritis?
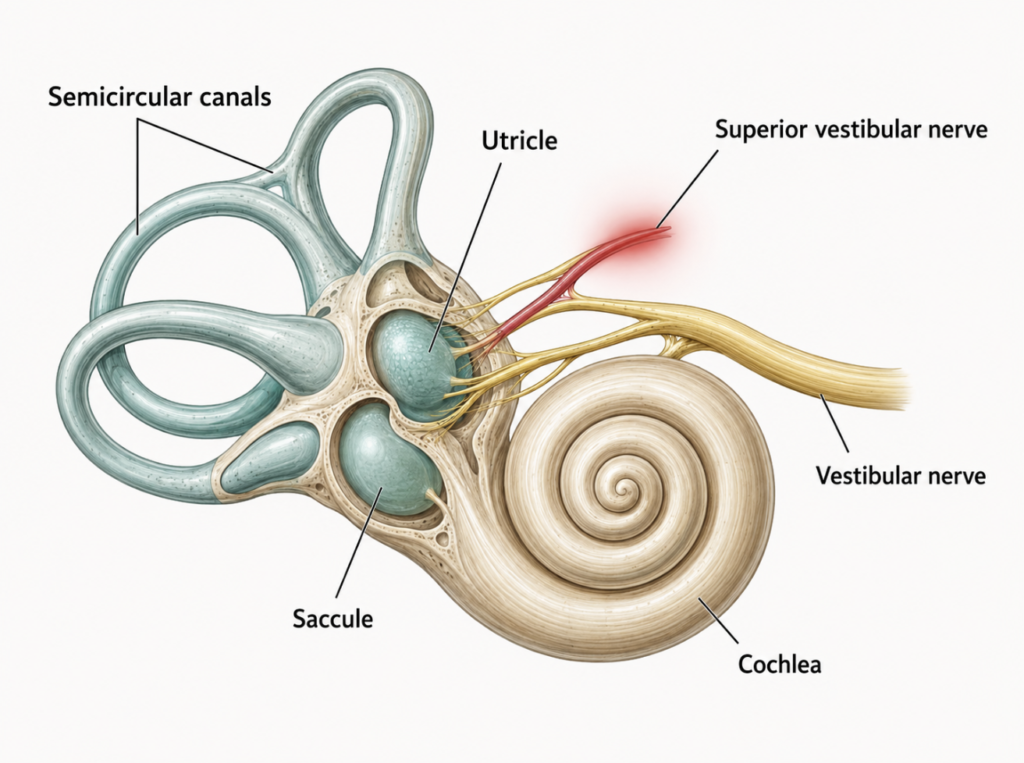
Vestibular neuritis is inflammation of the vestibular nerve, the cable carrying balance signals from the inner ear to the brain. When one side becomes inflamed, the brain suddenly receives lopsided input: the healthy ear keeps reporting motion while the affected ear goes quiet. The brain interprets that mismatch as continuous spinning.
The defining feature is what is missing. The vestibular nerve has two branches, and neuritis typically spares the cochlear nerve, so hearing stays normal [Bae, Current diagnosis and treatment of vestibular neuritis: a narrative review, 2021]. When vertigo arrives with hearing loss or tinnitus, the label shifts to labyrinthitis — a useful distinction that points toward different inner-ear structures.
What Causes It?
The honest answer is that the cause is not fully settled. The leading hypothesis is reactivation of latent herpes simplex virus type 1 in the vestibular ganglion, which is why the condition often follows a cold or upper-respiratory infection. Two other mechanisms are also described: ischemia of the anterior vestibular artery, and immune-mediated inflammation [Bae, Current diagnosis and treatment of vestibular neuritis: a narrative review, 2021].
Symptoms, and Who Gets It
The presentation is dramatic and consistent: abrupt, true spinning vertigo that lasts more than 24 hours, paired with nausea, vomiting, unsteady gait, and intolerance of head movement. Spontaneous nystagmus — rhythmic eye-beating away from the affected side — is usually visible. Crucially, there are no cochlear symptoms and no other neurological signs [Bae, Current diagnosis and treatment of vestibular neuritis: a narrative review, 2021].
It is generally reported to affect working-age adults, most often between 30 and 60, with no strong sex predilection. Symptoms are typically most severe in the first 24 to 72 hours, then ease as the brain begins to adapt.
The Question That Comes First: Is It a Stroke?
This is the section that matters most. Acute vestibular syndrome — sudden vertigo with nystagmus and gait unsteadiness — usually means vestibular neuritis, but a posterior-circulation stroke can produce an almost identical picture. Mistaking one for the other is dangerous, and focal neurological signs are often absent in these strokes, so “the exam looks clean” is not reassurance.
Here is the counterintuitive part: a focused three-step bedside eye exam can outperform early imaging. The HINTS exam (Head Impulse, Nystagmus, Test of Skew) was 100% sensitive and 96% specific for stroke in patients with acute vestibular syndrome — and more sensitive than MRI diffusion-weighted imaging performed in the first 48 hours, which was falsely negative in 12% of cases [Kattah, HINTS to diagnose stroke in the acute vestibular syndrome, 2009].
One precondition makes or breaks its use: HINTS is only valid in acute vestibular syndrome — a patient with continuous vertigo and spontaneous nystagmus. Applied to brief, position-triggered spells like BPPV, or to anyone without spontaneous nystagmus, the exam can mislead rather than clarify [Jeong, Vestibular neuritis, 2013]. A normal head impulse test only carries its “red flag for stroke” meaning inside that specific setting.
The logic of each step is worth understanding:
- Head impulse test — In vestibular neuritis, the reflex that keeps the eyes locked on a target during a quick head turn is broken on the affected side, producing a visible corrective eye-jerk. A normal result during acute vertigo is paradoxically a red flag for stroke.
- Nystagmus — Peripheral nystagmus beats in one fixed direction. Nystagmus that changes direction with gaze suggests a central cause.
- Test of skew — A vertical misalignment of the eyes points toward the brainstem.
Clinical Perspective A common reflex is to order an MRI and feel reassured when it is clean. But in the first 48 hours that reassurance can be false, while a careful bedside exam done well is more sensitive. The takeaway is not “skip imaging” — it is that the eyes, examined properly, often tell the story before the scanner does.
| Feature | Vestibular neuritis (peripheral) | Posterior-circulation stroke (central) |
|---|---|---|
| Head impulse test | Abnormal — visible corrective eye-jerk on the affected side | Often normal (a red flag in this setting) |
| Nystagmus | Unidirectional, horizontal, fixed direction | Direction-changing or vertical |
| Test of skew | Absent | May show vertical eye misalignment |
| Hearing | Usually normal | Usually normal; new hearing loss is a warning sign |
| Gait | Unsteady but usually able to walk | Often severe — unable to stand or walk unaided |
Essential Diagnostic Tests
Vestibular neuritis is ultimately a clinical diagnosis, supported by targeted vestibular testing rather than a single confirmatory scan. The core studies are the head impulse test, the bithermal caloric test (which measures how each ear responds to warm and cool irrigation and quantifies the weakness on the affected side), and vestibular-evoked myogenic potentials, which probe specific branches of the vestibular nerve [Bae, Current diagnosis and treatment of vestibular neuritis: a narrative review, 2021]. Imaging is reserved for ruling out central causes when the history, risk factors, or exam raise concern.
Treatment: Acute Phase vs Recovery Phase
Acute phase — calm the storm. In the first days, the priority is controlling vertigo and vomiting with short-term symptomatic medication: vestibular suppressants and antiemetics [Bae, Current diagnosis and treatment of vestibular neuritis: a narrative review, 2021]. These drugs are deliberately short-term — generally kept to no more than 3 to 5 days — because leaning on them longer slows central compensation, the very brain adaptation that drives recovery.
On disease-modifying treatment, the evidence is clarifying and, for many readers, surprising. In a randomized double-blind trial, methylprednisolone significantly improved the recovery of peripheral vestibular function at 12 months, while the antiviral valacyclovir did not — and adding the antiviral to the steroid offered no advantage over the steroid alone [Strupp, Methylprednisolone, valacyclovir, or the combination for vestibular neuritis, 2004]. Corticosteroids work best early, during active inflammation.
Clinical Perspective “It might be viral, so let’s add an antiviral” is intuitive, but the strongest trial data did not support antivirals for this condition. That gap between a plausible mechanism and a measured outcome is exactly why evidence, not instinct, should drive the prescription.
Recovery phase — retrain the brain. Once the acute nausea settles, the engine of long-term recovery is vestibular rehabilitation: structured exercises that push the brain to recalibrate around the weakened ear. A Cochrane review of 39 trials found moderate-to-strong evidence that vestibular rehabilitation is a safe and effective treatment for unilateral peripheral vestibular dysfunction, improving symptoms and daily function [McDonnell, Vestibular rehabilitation for unilateral peripheral vestibular dysfunction, 2015].
Prognosis
Most people recover well. The intense vertigo usually fades within days as central compensation begins, and balance continues to improve over the following weeks. Some patients are left with mild, lingering unsteadiness or motion sensitivity — and this is precisely the group that benefits most from sticking with rehabilitation rather than waiting passively for it to pass.
Key Takeaways
- Vestibular neuritis causes sudden spinning vertigo lasting more than 24 hours, with no hearing loss and no other neurological signs.
- The leading suspected cause is viral (HSV-1 reactivation), though ischemic and immune mechanisms are also described; the cause is not fully proven.
- The first job is to exclude stroke — and a well-performed HINTS bedside exam can be more sensitive than early MRI.
- Steroids improved recovery in randomized data; antivirals did not.
- Vestibular rehabilitation is the evidence-based driver of long-term recovery.
FAQ
How long does vestibular neuritis last? The severe vertigo usually lasts a few days, then improves steadily over weeks. Most people recover well, though some have mild residual unsteadiness that rehabilitation can address.
Is vestibular neuritis the same as a stroke? No, but they can look identical at onset, which is why ruling out stroke is the first priority. A focused bedside eye exam (HINTS) helps distinguish them and can outperform early MRI.
What’s the difference between vestibular neuritis and labyrinthitis? Vestibular neuritis spares hearing; labyrinthitis involves hearing loss or tinnitus because it affects additional inner-ear structures. The presence or absence of cochlear symptoms is the dividing line.
Can it come back? Recurrence is uncommon. Most cases are single episodes, and the brain’s compensation typically holds once recovery is complete.
Further Reading
- Vestibular Neuritis — Cleveland Clinic: a clear patient-facing overview of symptoms, causes, and recovery.
- Vestibular Neuronitis — Merck Manual (Professional Version): a concise clinician-level reference, including the HINTS exam.
- Medications for Dizziness & Vertigo — Vestibular Disorders Association (VeDA): how symptom-relief medications are used, and why they are kept short-term.
References
- Bae CH, Na HG, Choi YS. Current diagnosis and treatment of vestibular neuritis: a narrative review. J Yeungnam Med Sci. 2021;39(2):81-88.
- Jeong SH, Kim HJ, Kim JS. Vestibular neuritis. Semin Neurol. 2013;33(3):185-194.
- Kattah JC, Talkad AV, Wang DZ, Hsieh YH, Newman-Toker DE. HINTS to diagnose stroke in the acute vestibular syndrome: three-step bedside oculomotor examination more sensitive than early MRI diffusion-weighted imaging. Stroke. 2009;40(11):3504-3510.
- Strupp M, Zingler VC, Arbusow V, et al. Methylprednisolone, valacyclovir, or the combination for vestibular neuritis. N Engl J Med. 2004;351(4):354-361.
- McDonnell MN, Hillier SL. Vestibular rehabilitation for unilateral peripheral vestibular dysfunction. Cochrane Database Syst Rev. 2015;1(1):CD005397.
Joonpyo Hong, MD is a board-certified otolaryngologist practicing in Korea. This article reflects his clinical interpretation of published research and does not constitute individual medical advice.
For more interesting contents:
https://curiousmd.com/room-spins-when-youre-drunk/
https://curiousmd.com/motion-sickness-aftereffects/
https://curiousmd.com/senaptec-strobe-vestibular-neuroplasticity/