
Two patients walk into clinic with the same diagnosis: HPV-positive throat cancer, removed cleanly by surgery. One sails through with no further treatment. The other gets weeks of radiation and chemotherapy. For years, deciding which patient is which has relied on staging rules that everyone agrees are imperfect. A 2026 study asks whether a machine-learning model can draw that line more precisely — and the answer is interesting, with an asterisk.
This look at AI de-escalation in HPV throat cancer covers what the model actually did, what “C-index 0.77” means for a real patient, and why the researchers themselves are telling clinicians not to change practice yet.
AI De-escalation in HPV Throat Cancer
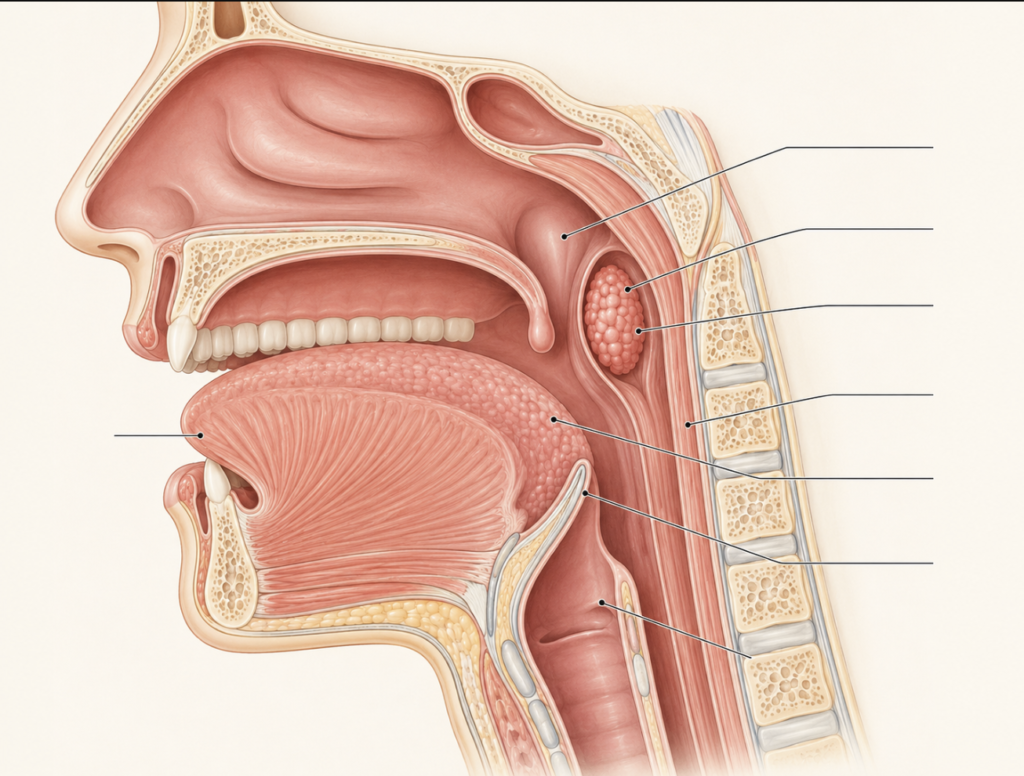
HPV-positive oropharyngeal cancer — cancer of the tonsils and base of tongue driven by the human papillomavirus — behaves very differently from the smoking-and-alcohol type. It responds strikingly well to treatment, and cure rates are high. The catch is that the patients are often younger and will live for decades with whatever side effects the treatment leaves behind: dry mouth, swallowing trouble, dental damage, neck stiffness.
That mismatch — excellent prognosis, heavy long-term toxicity — is the entire rationale for de-escalation. The goal is to keep the cure while subtracting the harm (Chen, De-escalation for Human Papillomavirus-Positive Oropharyngeal Cancer: A Look at the Prospective Evidence, 2025).
The problem is that subtracting treatment has proven dangerous when done with a broad brush. The first generation of randomized trials that tried to swap out or reduce chemotherapy largely failed to change the standard of care, and in some cases compromised outcomes without actually reducing toxicity (Kang, Consensuses, Controversies, and Future Directions in Treatment Deintensification for Human Papillomavirus-Associated Oropharyngeal Cancer, 2022). The lesson was blunt: de-escalation only works if you can pinpoint exactly who can afford it.
What the Machine-Learning Model Did
A 2026 study set out to sharpen that targeting (Costantino, Optimizing Adjuvant Therapy Selection With Machine Learning After Transoral Surgery in HPV-Related Oropharyngeal Cancer, 2026). The researchers used the National Cancer Database, pulling 5,569 patients with HPV-positive throat cancer who had been treated with transoral surgery — minimally invasive removal of the tumor through the mouth.
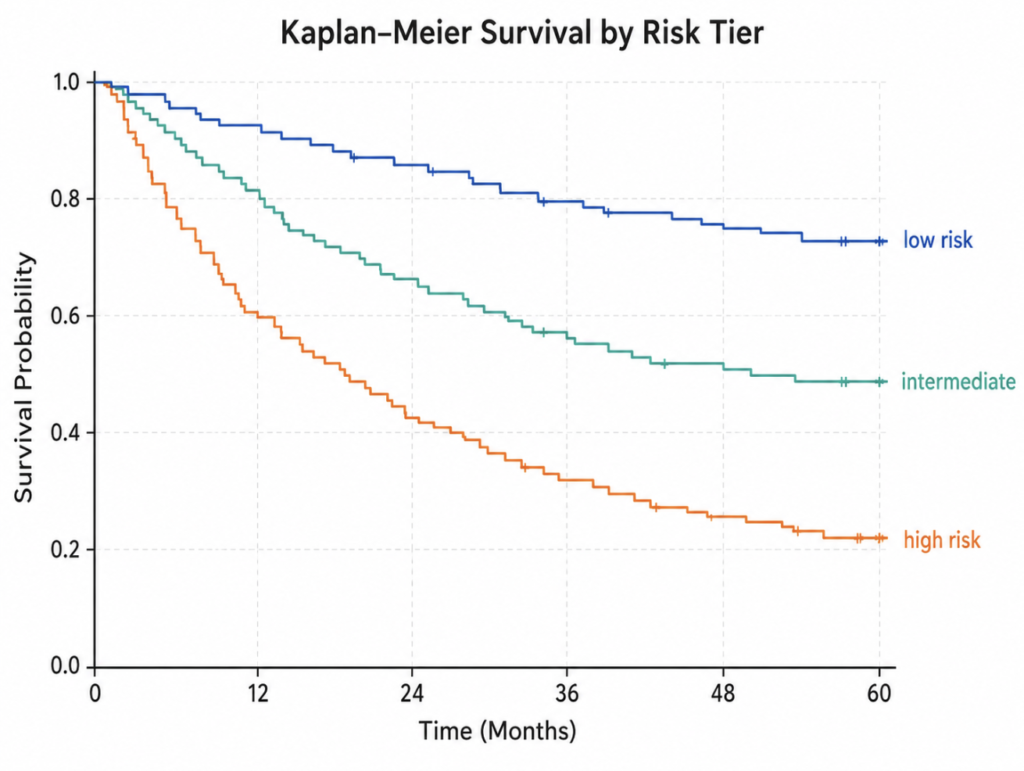
They trained three different survival models: DeepSurv, Neural Multi-Task Logistic Regression, and Random Survival Forest. Each one learned from the subset of patients who had surgery alone, then scored the full cohort and sorted patients into three buckets — low, intermediate, and high risk.
The point was not just to predict survival. It was to ask, within each risk group, whether adding radiation or chemoradiation after surgery actually improved overall survival.
What “C-index 0.77–0.80” Actually Means
All three models landed in a C-index range of 0.77 to 0.80, with acceptable calibration (Costantino, 2026). The concordance index, or C-index, is the standard way to grade a survival model: 0.50 is a coin flip, 1.0 is perfect. Roughly speaking, 0.77 means that if you pick two patients at random, the model correctly ranks who is at higher risk about 77% of the time.
That is solidly good for clinical prediction — better than staging alone tends to manage — but it is nowhere near perfect. One in five rankings is wrong. That gap is exactly why this is a research tool and not yet a bedside one.
Can AI Decide Who Skips Radiation?
No — and that is the honest headline. The model proposes risk groups; it does not make treatment decisions. Its value is in matching the intervention to the risk.

In the study, the pattern was consistent and clinically sensible (Costantino, 2026). In the low-risk group, adding radiation or chemoradiation conferred no measurable benefit to overall survival. In the intermediate group, radiation or chemoradiation did help. In the high-risk group, the heavier chemoradiation regimen showed the largest benefit. In other words, the model pushed de-escalation toward patients whose survival odds did not improve with more treatment, and escalation toward those who clearly gained.
Here is the part that matters most for any patient reading this. “No survival benefit” is not the same as “safe to skip radiation.” The model measured overall survival — whether patients were alive years later. It did not measure locoregional control, which is whether the cancer comes back in the throat or neck. Those are different questions. A patient can survive just as long statistically and still face a recurrence that means more surgery, more recovery, and real suffering.
Randomized trials in this disease have shown that cutting radiation can raise the risk of local recurrence even when survival holds steady (Kang, 2022). Complete omission of radiation is not a current standard of care, even for low-risk patients with clean margins.
What this kind of research points toward is not “no treatment” but better-calibrated treatment — for example, reduced-dose or reduced-volume radiation for carefully selected patients, an approach the field is actively testing rather than one that is settled (Chen, 2025).
The features driving these predictions were not exotic: age, surgical margin status, other illnesses (comorbidity), insurance status, and how high-volume the treating facility was all carried weight. One important factor, extranodal extension, varied in influence between models. Extranodal extension means the cancer has broken through the outer capsule of a lymph node and spread into surrounding tissue — a finding that typically signals a need for more aggressive treatment, which is exactly why a model that handles it inconsistently warrants caution.
Clinical Perspective
The encouraging part is that the model’s risk grouping lines up with surgical intuition. A clean-margin, otherwise-healthy patient with a small tumor is precisely who a surgeon already suspects sits at the low end of the risk spectrum. When a model trained on 5,569 cases independently reaches the same conclusion, it adds quantitative weight to a judgment that used to be made by feel. That is useful for designing trials and counseling patients — not for unilaterally dropping treatment.
The sobering part is the word “retrospective.” This model learned from records of decisions already made, not from a trial that deliberately withheld radiation from low-risk patients to see what happened. Database studies carry hidden biases — the healthiest patients may have skipped radiation for reasons the data never captured. Two of the model’s top features, insurance status and facility volume, are markers of access and resources, not biology. A prediction engine that leans on them is partly modeling the healthcare system, not just the tumor.
That is why the study authors explicitly call for prospective, model-guided trials before any of this touches practice (Costantino, 2026). It echoes the field’s hard-won caution: stage and HPV status alone have proven insufficient to guide de-escalation safely, and adding a clever model does not erase the need to test it forward in time (Kang, 2022).
Key Takeaways
- A 2026 machine-learning study sorted 5,569 HPV-positive throat cancer patients into risk groups with a C-index of 0.77–0.80, good but imperfect discrimination (Costantino, 2026).
- In the model’s low-risk group, adding radiation or chemoradiation offered no measurable benefit to overall survival — but the study did not measure local recurrence, so this is not evidence that radiation can be safely skipped.
- The strongest predictors included age, surgical margin status, comorbidity, insurance status, and facility volume — a mix of biology and healthcare access.
- The study is retrospective; the authors call for prospective trials before any change to clinical practice, and complete radiation omission is not a current standard even for low-risk patients.
- For now, following the standard treatment a multidisciplinary team recommends remains the safest course; first-generation de-escalation trials failed when applied broadly (Kang, 2022).
FAQ
Can AI safely reduce my cancer treatment?
Not on its own, and not yet. The model in this study identifies risk groups but does not decide treatment, and it has only been tested on past records, not in a forward-looking trial. Any treatment decision belongs to a patient and their oncology team.
How accurate is the model?
Its C-index of 0.77–0.80 means it correctly ranks which of two patients is higher-risk roughly 77–80% of the time (Costantino, 2026). That is strong for clinical prediction but still wrong in about one in five cases.
Should patients ask their doctor for less treatment?
No — not based on this study. It measured survival, not the risk of the cancer returning in the throat or neck, and reducing radiation can raise that recurrence risk even when survival stays the same (Kang, 2022). For now, following the standard treatment a multidisciplinary team recommends is the safest way to keep recurrence rates low. The right move is to discuss the science with a treating physician, not to seek less treatment based on a risk score.
References
- Chen AM. De-escalation for human papillomavirus-positive oropharyngeal cancer: a look at the prospective evidence. Curr Oncol Rep. 2025;27(4):355-361.
- Costantino A, Paleri V, Williamson A, et al. Optimizing adjuvant therapy selection with machine learning after transoral surgery in HPV-related oropharyngeal cancer. Oral Oncol. 2026;179:108024.
- Kang JJ, Yu Y, Chen L, et al. Consensuses, controversies, and future directions in treatment deintensification for human papillomavirus-associated oropharyngeal cancer. CA Cancer J Clin. 2022;73(2):164-197.
For more interesting contents:
https://curiousmd.com/hpv-vocal-cord-cancer-young-non-smokers/
https://curiousmd.com/hpv-oropharyngeal-cancer/
Link out to
- National Cancer Institute — HPV and Cancer
- National Cancer Institute — Oropharyngeal Cancer Treatment (PDQ)
- NIDCR — HPV & Oropharyngeal Cancer
- Source study — Oral Oncology (2026)
Joonpyo Hong, MD is a board-certified otolaryngologist practicing in Korea. This article reflects his clinical interpretation of published research and does not constitute individual medical advice.