
A patient walks in convinced something is wrong with their balance, yet the standard inner-ear tests come back clean. The problem is real, but the usual tools point everywhere and nowhere. This is exactly the gap where computerized stabilometry earns its place: a force platform under the feet that turns the invisible micro-sway of “just standing still” into numbers you can read.
This article explains what computerized stabilometry actually measures, how the test is performed, and the clinical situations where it adds information that caloric testing and video-nystagmography miss.
What Is Computerized Stabilometry?
Computerized stabilometry, also called posturography, measures how much your body sways while you try to stand still. You stand on a rigid platform fitted with load cells — pressure sensors at each corner — that record the vertical force your feet apply. From those forces, software calculates the center of pressure (CoP): the single moving point on the ground that represents where your body weight is being balanced at each instant.
Standing upright is never truly still. The CoP drifts and corrects dozens of times per second, tracing a small, jittery path. Stabilometry records that path and reduces it to objective values you can compare against normal ranges or against the same person before and after treatment.
What the Test Actually Measures
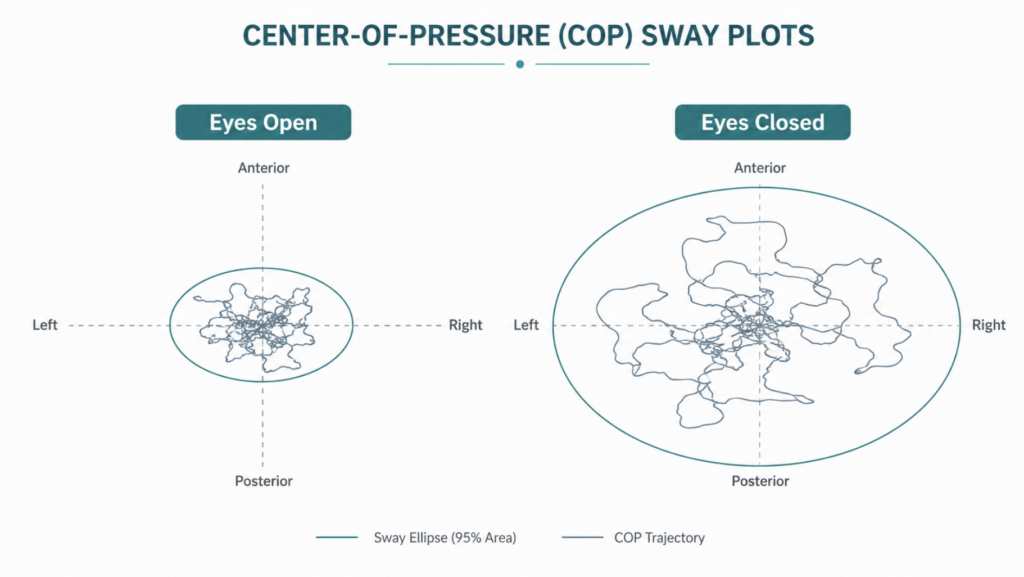
The raw output is the CoP trajectory, summarized by a handful of parameters. The most reported are the sway area (the size of the ellipse that contains most of the CoP path), sway velocity (how fast the CoP moves), and path length (total distance traveled). Larger and faster sway generally means poorer postural control.
These parameters are not academic curiosities. In older adults, CoP path length, CoP velocity, and the magnitude of sway in the side-to-side and front-to-back directions are the variables that most consistently separate people who fall from those who do not [Pizzigalli, The contribution of postural balance analysis in older adult fallers: A narrative review, 2016].
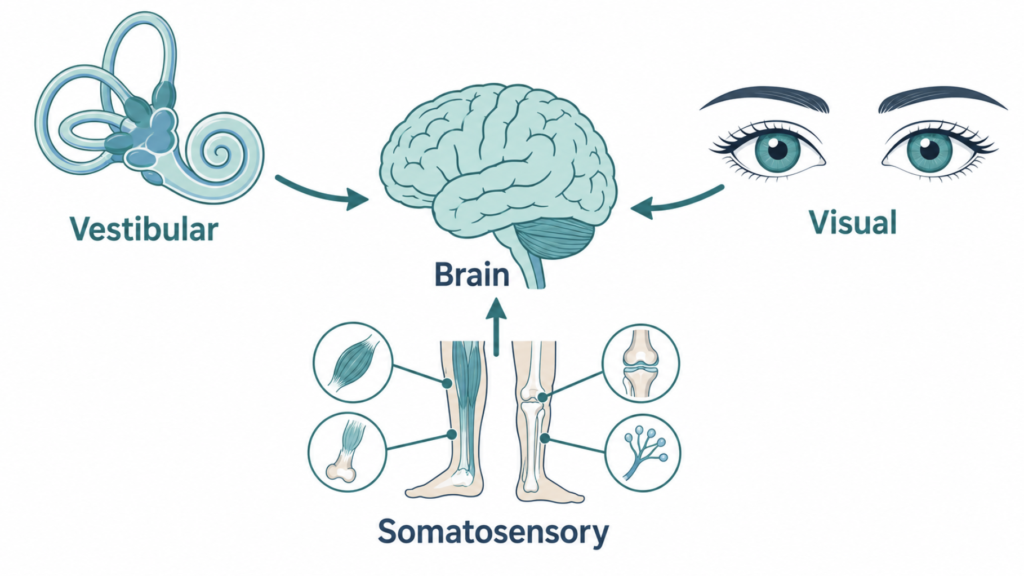
The three systems behind balance
Staying upright depends on three streams of information: the inner ear (vestibular), the eyes (visual), and the body’s position sensors in muscles and joints (somatosensory). The brain blends all three. Stabilometry becomes diagnostically useful when you start removing or distorting these inputs and watch what happens to sway — because that reveals which stream the patient is over-relying on, and which one is failing.
How Computerized Stabilometry Is Performed
The basic version is quick and non-invasive. You stand barefoot on the platform, arms at your sides, and hold as still as you can for a fixed recording window, typically 30 to 60 seconds per trial.

The key is varying the conditions. The classic comparison is eyes open versus eyes closed — the modern, instrumented descendant of the bedside Romberg test. A person whose sway balloons the moment their eyes close is leaning heavily on vision to compensate for weaker vestibular or somatosensory input. Adding a soft foam surface degrades the body’s position sense, pushing even more of the work onto the inner ear.
This logic is formalized in dynamic posturography and its Sensory Organization Test (SOT), where the platform and the visual surround can tilt in sync with the patient’s own sway to systematically cancel out vision and proprioception. Patients wear a safety harness, since the harder conditions are genuinely destabilizing. The result is a profile of which sensory system is doing the heavy lifting and which has dropped out.
When Stabilometry Helps
Unexplained dizziness with normal routine tests. This is a common use. Stabilometry and video-nystagmography assess different aspects of balance, and their results often do not line up — which is why the two are best read as complementary rather than interchangeable. A normal VNG characterizes the inner-ear reflex; it does not, on its own, describe how well a patient holds their posture, and that is the gap stabilometry fills [Gofrit, The association between video-nystagmography and sensory organization test of computerized dynamic posturography in patients with vestibular symptoms, 2019].
Connecting test results to how a patient actually feels. In acute vestibular neuritis, SOT composite scores tracked patients’ self-reported dizziness handicap, while caloric test results did not [Shim, Typical sensory organization test findings and clinical implication in acute vestibular neuritis, 2018]. When the goal is to explain a patient’s lived symptom rather than just localize a lesion, the balance measure can be the more relevant number.
Tracking rehabilitation. Because the output is quantitative, it lends itself to before-and-after comparison. As one illustration, patients with stable one-sided vestibular loss showed improved SOT composite scores after a course of computerized vestibular retraining, and that improvement tracked a drop in their fear of falling — though this came from a small single-arm study (n=13) and should be read as suggestive rather than definitive [David, Dynamic posturography after computerized vestibular retraining for stable unilateral vestibular deficits, 2023].
Fall-risk screening in older adults. Posturographic parameters are associated with fall history, and the eyes-open-on-a-compliant-surface condition has been especially good at separating fallers from non-fallers [Merlo, Postural stability and history of falls in cognitively able older adults: the Canton Ticino study, 2012].
Clinical Perspective
A useful way to frame stabilometry is that it answers a different question than the caloric test. Caloric testing asks, “Is one labyrinth weaker than the other?” Stabilometry asks, “Can this person actually keep themselves upright, and which sensory crutch are they using to do it?” Those questions have different answers more often than patients expect — which is precisely why a normal caloric result should not end the conversation when someone insists their balance is off.
The honest caveat: sway numbers describe postural control well but predict individual falls only modestly. Stabilometry is strongest as one input in a fuller assessment and as a tool for measuring change over time, not as a standalone crystal ball.
Key Takeaways
- Computerized stabilometry quantifies postural sway by tracking the center of pressure on a force platform.
- Comparing eyes-open with eyes-closed sway reveals how much a person depends on vision to stay balanced.
- It measures something different from caloric and video-nystagmography testing, so it can flag problems those tests miss.
- Its quantitative output makes it well suited to tracking progress through vestibular rehabilitation.
- Sway parameters relate to fall risk in older adults but are best used alongside other clinical information.
FAQ
Is computerized stabilometry the same as posturography? Yes — the terms are used interchangeably. Both describe measuring postural sway via a force platform. “Static posturography” refers to standing on a fixed surface, while “dynamic posturography” adds a platform and visual surround that can move to challenge balance.
Does the test hurt or cause dizziness? No, it is non-invasive and painless. You simply stand on a platform. The harder dynamic conditions can feel briefly destabilizing, which is why patients wear a safety harness, but the test does not involve any uncomfortable stimulation.
Static or dynamic posturography — which one is needed? It depends on the question. Static testing with eyes open and closed is fast and screens overall sway. Dynamic testing with the Sensory Organization Test is used when the goal is to isolate which sensory system — vestibular, visual, or somatosensory — is responsible for the imbalance.
References
- Gofrit SG, Ilan O, Mayler Y, Eliashar R, Bdolah-Abram T, de Jong MA, Gross M. The association between video-nystagmography and sensory organization test of computerized dynamic posturography in patients with vestibular symptoms. Eur Arch Otorhinolaryngol. 2019;276(12):3513-3517.
- Shim DB, Song MH, Park HJ. Typical sensory organization test findings and clinical implication in acute vestibular neuritis. Auris Nasus Larynx. 2018;45(5):916-921.
- David EA, Shahnaz N. Dynamic posturography after computerized vestibular retraining for stable unilateral vestibular deficits. Acta Otolaryngol. 2023;143(5):396-401.
- Merlo A, Zemp D, Zanda E, Rocchi S, Meroni F, Tettamanti M, Recchia A, Lucca U, Quadri P. Postural stability and history of falls in cognitively able older adults: the Canton Ticino study. Gait Posture. 2012;36(4):662-666.
- Pizzigalli L, Micheletti Cremasco M, Mulasso A, Rainoldi A. The contribution of postural balance analysis in older adult fallers: A narrative review. J Bodyw Mov Ther. 2016;20(2):409-417.
Joonpyo Hong, MD is a board-certified otolaryngologist practicing in Korea. This article reflects his clinical interpretation of published research and does not constitute individual medical advice.
For more interesting contents:
https://curiousmd.com/vestibular-neuritis/
https://curiousmd.com/room-spins-when-youre-drunk/
https://curiousmd.com/motion-sickness-aftereffects/