
The audio feature drawing the most attention this year pivots on translation: a generative model in any pair of headphones, turning a language a person does not speak into one they do. The marketing is about borders and travel. The engineering underneath is about something else entirely. To translate live speech, a system has to recognize messy, accented, half-overlapping audio and regenerate it as clean, natural speech.
Strip away the part that changes the language, and what remains is a second capability that has nothing to do with foreign countries — clarifying speech in the same language for people who cannot make out words they can technically hear. That inward turn — the same engine aimed at intelligibility rather than translation — is what AI speech clarification means.
That second prospect is the more consequential one, because the most common complaint in an audiology clinic is not silence. It is unintelligibility. A patient with high-frequency hearing loss will often say, in some form, that they can hear perfectly well that someone is speaking but cannot tell what is being said. Their pure-tone audiogram looks treatable; their word recognition score — the percentage of single words they repeat back correctly — lags behind. The gap between those two numbers is where daily life actually breaks down. And it is exactly the gap a clean-speech regenerator seems built to close.
The appeal is obvious enough to be worth distrusting. Decades of effort have gone into making degraded speech clearer for damaged ears, and that history is mostly a record of one stubborn gap: acoustic improvements that show up on a lab bench but do not arrive at the dinner table. The newest approach — AI that pulls apart and rebuilds sound — has more going for it than its predecessors. It is also, on close reading of the evidence, strongest precisely where listening is already easy and weakest precisely where it is hard.
The promise is real. It is simply not the promise most people would assume.
The feature is translation. The capability is clarification.
The two tasks share a back end but solve different problems. Translation removes a language barrier. Same-language clarification confronts an audibility-and-discrimination barrier, which is a different obstacle with a different anatomy.
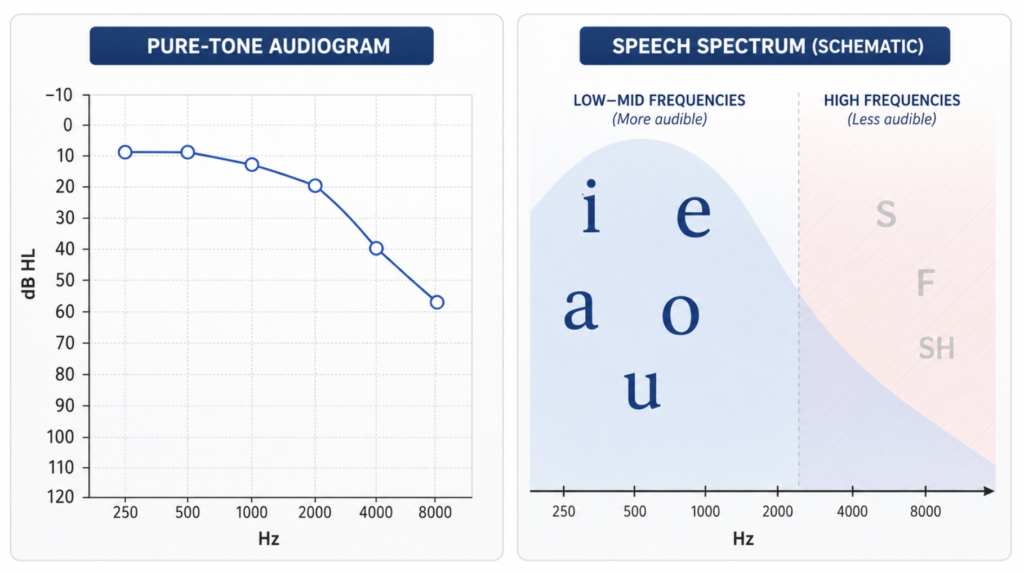
The anatomy is well understood. Vowels carry most of their energy in the low frequencies and are comparatively loud; consonants — the fricatives and stops like /s/, /f/, /sh/, and /th/ — sit high in the spectrum and are comparatively faint.
The information that distinguishes one word from another lives disproportionately in those quiet, high-frequency consonants. High-frequency sensorineural hearing loss removes them first. The result is a person who receives the loud, low scaffolding of speech and loses the fine detail that tells sip from ship from sit. The audiogram can look modest while word recognition collapses, because the missing band is small in size and large in consequence.
From there the logic almost writes itself: if a model can detect those degraded consonant cues and regenerate them cleanly, it should restore the discrimination that hearing loss took away. That inference is reasonable. It is also where the evidence begins to push back.
Clinical Perspective. The clinically useful number in this conversation is not the audiogram but the word recognition score, and the two often disagree. A feature that makes sound louder or sharper is solving a problem many of these patients do not have; their problem is that the cues carrying meaning were destroyed at the source. That distinction governs everything that follows.
Why clearer sound rarely makes clearer words
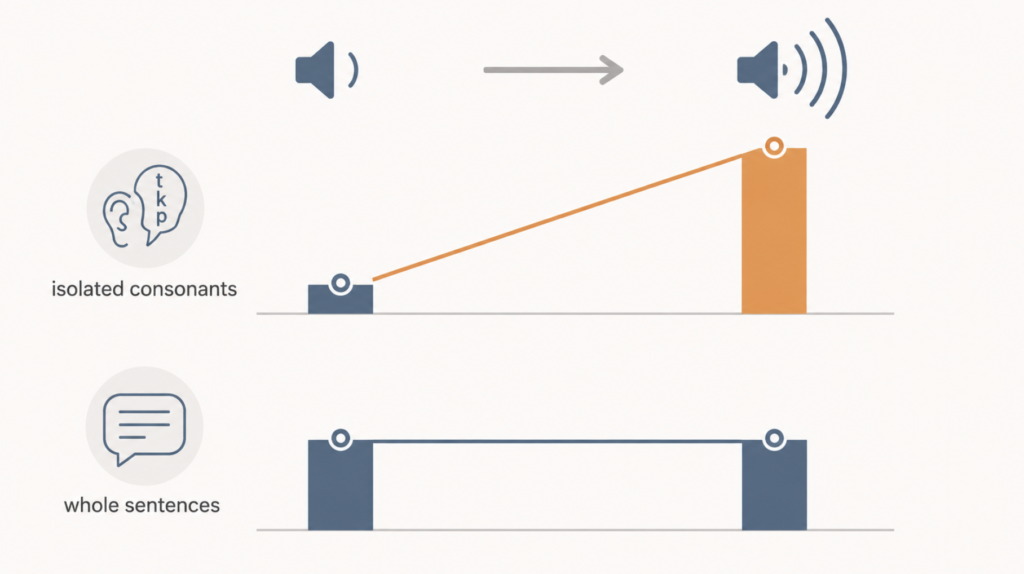
The cleanest test of the central premise comes from work that is not about AI at all. When older hearing-impaired listeners spent forty hours training their consonant identification, their ability to identify consonants in noise improved substantially — roughly a 9-decibel gain, with statistically significant benefit in about nineteen of twenty participants. By the logic above, sentence understanding should have followed. It did not. Their scores on understanding actual sentences showed no significant improvement [Woods, Perceptual Training in Older HI Listeners, 2015].
The gain stalled at the level of isolated sounds and never reached connected speech, because understanding a sentence is not an acoustic act. It is a predictive one, filled in by context and the brain. Restoring an /s/ does not restore that machinery.
The same pattern recurs wherever someone has tried to engineer high-frequency cues back into the signal. Nonlinear frequency compression — the established technique of lowering high-frequency energy into a range a damaged ear can still use — does produce a measurable word-recognition benefit in milder high-frequency loss. The benefit averages around seven percent: a handful of additional words correct in every hundred, tracking the small increase in audibility it provides [McCreery, Audibility and NFC, 2014]. That is a real effect. It is also a modest one, and it is the optimistic end of the single-feature approaches.
There is a deeper reason these gains stay small. Sensorineural hearing loss does not merely turn down the volume on certain frequencies; it broadens the ear’s internal tuning, smearing the fine spectral and temporal detail the brain uses to separate sounds. A regenerated signal, however pristine, still has to pass back through that damaged biology. Cleaning the input cannot lift a listener above their own discrimination capacity. The signal can be made perfect; the ear receiving it cannot.
This is the trap the translation analogy hides. A clearer recording of speech is not the same as clearer hearing of speech.
Clinical Perspective. The most honest framing for any clarification technology is that it improves the signal, not the receiver. For a patient whose low word recognition stems from neural or central loss rather than missing high-frequency audibility, sharper consonants have a low ceiling — and visual support, such as live captions, may do more than any audio regeneration can.
The frequency-lowering trap, and a debate the AI inherits
A specific marketing claim deserves specific scrutiny: that a smart enough model could outperform conventional frequency-lowering hearing aids by knowing where each patient’s cochlear dead regions are — the spots along the cochlea where sensory cells are so damaged that sound delivered there yields no useful hearing — and routing sound around them.
The trouble is that the premise beneath the claim is itself unsettled.
On one side, careful work on patients with extensive dead regions found that frequency-lowering algorithms did make some high-frequency sounds audible, yet at the group level produced no significant improvement on any speech measure — not consonant identification, not sentences in noise, not the patients’ own ratings [Salorio-Corbetto, Frequency Transposition vs Compression in Dead Regions, 2019]. Audibility went up; understanding did not move. That argues for caution about pushing sound into damaged regions at all.
On the other side, a large study of typical hearing-aid candidates found dead regions in roughly one in three patients, and concluded the opposite: there was no evidence to support reducing high-frequency amplification for them, because making high frequencies audible helped on average regardless of dead-region status [Cox, Dead Regions in Hearing Aid Candidates, 2011]. By this account, the very thing a “smart” system would do — avoid the dead regions — may be unnecessary or counterproductive.
So the field does not agree on whether dead regions should be avoided in the first place. A model marketed as cleverly optimizing around them is not resolving that question. It is inheriting it. The hard part here was never the intelligence of the processing; it is that clinicians do not yet agree on what the processing should be trying to do.
Clinical Perspective. When experts disagree about the goal, sophistication applied to the wrong goal is not progress. Any claim that AI “personalizes around” cochlear dead regions should be read as a claim built on contested ground, not as a settled advantage over existing hearing aids.
Where the evidence actually moves: separating voices, not sharpening sounds
If the single-feature record is sobering, one approach has a genuinely different trajectory — and it is not about reconstructing consonants. It is about pulling one voice out of many.
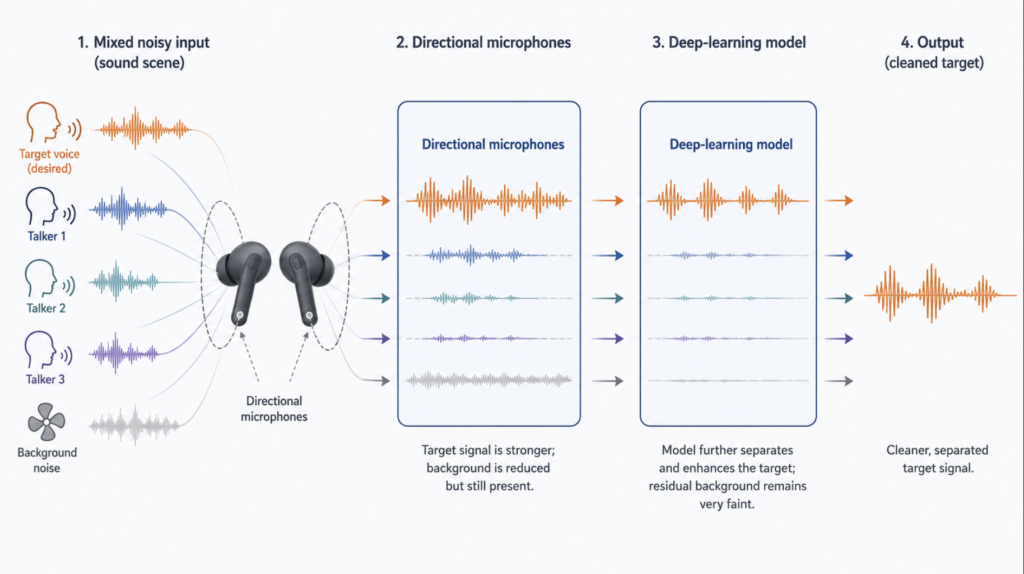
Here the evidence is the strongest in this whole area. In a controlled study with real patients fitted with commercial hearing aids, deep-neural-network noise reduction combined with directional microphones consistently outperformed traditional processing across speech recognition, listening effort, and sound quality [Folkeard, DNN Speech Recognition and Listening Effort, 2026].
That result comes from a team that includes researchers affiliated with a hearing-aid manufacturer, which is reason to weigh it carefully — but an independent academic group reported the same direction, finding that a deep-learning system extracting a target talker from a mixture improved intelligibility and reduced listening effort for hearing-impaired listeners, who in fact benefited more than normal-hearing listeners did [Sinha, Target Speaker Extraction for Hearing-Impaired Listeners, 2025]. Two separate lines, one industry and one academic, pointing the same way.
The mechanism is mundane and important. The dominant variable for understanding speech in noise is the signal-to-noise ratio — how much louder the target voice is than the competition. Directional microphones raise it by spatial filtering, and much of the AI’s benefit comes from being handed a cleaner signal to begin with. The lesson is that the gain is not magic generated from nothing; it is a better front end feeding a capable model.
The same evidence marks the boundary. The benefit concentrated in steady background noise with the talker in front, and shrank in multi-talker babble — the crowded restaurant where several people speak at once, which is the exact situation patients struggle with most.
Reverberant rooms erode it further. The most futuristic version, in which a brain-computer interface reads which speaker a listener is attending to and amplifies that one, does work in the laboratory: electroencephalography can identify the attended talker with around 81 percent accuracy — right roughly four times in five — but only within a one-to-two-second window and in simple two-speaker setups [Vandecappelle, EEG Auditory Attention Decoding, 2021]. A delay of a second or two is awkward for a conversation that turns quickly, and a controlled two-voice trial is not a dinner party.
Clinical Perspective. This is the lever worth taking seriously, and its limits are not incidental — they map onto daily life. It performs where listening is already manageable and falters in the noisy, echoing, fast-switching scenes that define real difficulty. Optimism here should be specific, not general.
The bear case: more processing is not more hearing
The most reliable way to misjudge this technology is to assume that more aggressive processing must mean better hearing. The evidence says the opposite can be true.
In a randomized, double-blind trial in which patients wore hearing aids in their own daily environments, stronger signal processing produced worse speech recognition as listeners got older [Souza, Variability in Response to Hearing Aid Processing, 2019]. Cognitive capacity sharpened the effect: when distortion and noise were at their worst, working memory alone accounted for nearly a third of the difference between listeners, and those with weaker working memory fared worse under heavier processing [Arehart, Working Memory and Hearing Aid Distortion, 2013].
The more a system manipulates a signal that has already passed through a damaged ear, the more some listeners — often the older ones who most need help — are left chasing a transformed signal they cannot follow. A “hearing-loss mode” that does more to the sound is not guaranteed to help everyone. For some, it does harm.
Layer that onto the transfer problem established earlier, and a pattern emerges. Component-level acoustic wins — sharper consonants, lowered frequencies, cleaner spectra — have repeatedly failed to become sentence-level understanding. Heavier processing carries its own risk for vulnerable listeners. And the approach that does work best in trials is weakest in the conditions that matter most.
Then there is the gap between what has been measured and what is being sold. Nearly all of the encouraging data come from speech-in-noise tests and computed quality scores in laboratories. Long-term, real-world outcomes — what changes after months of living with these earbuds — are essentially absent. The most plausible near-term harm may not be technical failure at all but delayed care: a person concluding that consumer earbuds are good enough and postponing the audiological evaluation, the hearing aid, or the cochlear implant they actually need.
The honest summary of the skeptical case is short. Making sound clearer is not the same as making words clearer, and doing more to a signal is not the same as doing more for a listener.
The bull case: what to realistically expect
None of this argues that the technology is empty. It argues that expectations belong in the right place.
Start by removing them from the wrong place. Single-feature tricks have a low ceiling: frequency compression buys roughly seven additional words in a hundred at best, and often nothing at the sentence level in severely damaged ears. No amount of regeneration crosses the biological limit — a listener whose word recognition has fallen for neural reasons cannot be lifted past their own capacity to discriminate. AI does not restore lost hearing. That sentence should anchor every reasonable expectation.
What it can realistically do falls into three areas.
The first is understanding in noise. This is where the evidence genuinely moves. Deep-learning separation paired with directional microphones improved speech recognition, quality, and effort for real patients in trials, and target-talker extraction helped hearing-impaired listeners more than it helped normal-hearing ones. The right way to state the win is precise: the technology does not return lost hearing, it makes residual hearing more usable, by raising the effective signal-to-noise ratio so the same ear can survive a harder room.
The second is reduced effort. For a hearing-impaired person, conversation is sustained cognitive labor — a continuous task of guessing at gaps — and that labor accumulates as measurable fatigue. Even when AI processing does not dramatically raise a recognition score, achieving the same score with less effort is a real outcome: it shortens the end-of-day exhaustion and lets a person stay in a conversation longer. Across several patient studies, effort and comfort improved earlier and more consistently than raw intelligibility did.
The third is access. This class of processing once lived inside expensive premium hearing aids. The same kind of model now runs on ordinary earbuds. Independent of any clinical effect, moving hearing support out of the exclusive domain of medical devices is a meaningful shift on its own.
The lever-by-lever picture, read coldly, looks like this:
| Approach | What it does | Realistic benefit | The catch |
|---|---|---|---|
| Sharpening consonant cues | Boosts the faint sounds that distinguish words | Gains at the level of isolated sounds | Rarely transfers to sentence understanding [Woods 2015] |
| Frequency lowering | Moves high-frequency energy into a usable range | Around seven words in a hundred, in milder loss | Often no measurable speech gain in severely damaged ears [McCreery 2014; Salorio-Corbetto 2019] |
| AI noise reduction + directional mics | Raises the target voice above the background | Real improvement in noise, for real patients | Shrinks in multi-talker babble and reverberation [Folkeard 2026] |
| AI target-talker extraction | Pulls one chosen voice from a mixture | Better intelligibility and less effort in small trials | Algorithm-dependent; small samples [Sinha 2025] |
| Brain-steered selection | Reads the attended talker and amplifies it | Identifies the right voice in the lab | Seconds of delay; two-speaker setups only [Vandecappelle 2021] |
Clinical Perspective. The realistic outcome is not cure but amplified usefulness — not the recovery of lost hearing, but more practical use of the hearing that remains. A patient who follows family a little better in a loud restaurant, tires less by the end of the day, and gets that help without an expensive device has received exactly what the evidence supports. That is a smaller claim than the marketing makes. It is also not a small thing.
Key Takeaways
- The headline capability is translation, but the more consequential one beneath it is clarifying speech in the same language for people who hear sound yet miss words.
- Word recognition, not the audiogram, is the number that tracks daily difficulty — and the two routinely disagree.
- Making sound clearer has repeatedly failed to make words clearer; gains at the level of isolated sounds stall before they reach sentence understanding.
- Heavier processing is not safer processing: stronger signal manipulation can reduce recognition for older listeners and those with weaker working memory.
- The approach with the best patient evidence is separating one voice from many — and it performs best in easy listening conditions and worst in the noisy, echoing scenes that define real difficulty.
- The defensible promise is amplified usefulness of residual hearing, not restoration of lost hearing.
FAQ
Can AI earbuds replace a hearing aid or cochlear implant? No. The supporting evidence comes from short laboratory speech-in-noise tests, not long-term real-world outcomes, and none of it shows recovery of lost hearing. The realistic role is making residual hearing more usable, which is an aid to care, not a substitute for it [Folkeard, DNN Speech Recognition and Listening Effort, 2026].
Will clearer audio fix a low word recognition score? Usually not on its own. Word recognition often falls because of damage at the source that regenerated sound still has to pass back through, so cleaning the signal has a ceiling. When listeners improved at identifying isolated consonants, their sentence understanding did not follow [Woods, Perceptual Training in Older HI Listeners, 2015].
Is more aggressive processing better? It depends, and sometimes it is worse. In a randomized trial, stronger processing lowered speech recognition as listeners aged, and those with weaker working memory did worse under heavier processing [Souza, Variability in Response to Hearing Aid Processing, 2019].
Where does AI actually help most? In noise. Deep-learning separation with directional microphones improved understanding and reduced effort for real patients, and helped hearing-impaired listeners more than normal-hearing ones — though the benefit narrows in crowded, multi-talker rooms [Sinha, Target Speaker Extraction for Hearing-Impaired Listeners, 2025].
References
- Folkeard P, Ashkanichenarlogh V, Rahme M, et al. The effect of deep neural network implementation on speech recognition, listening effort, and sound quality in older adults with mild to moderately severe hearing loss. Trends Hear. 2026;30:23312165261449983. https://doi.org/10.1177/23312165261449983
- Sinha R, Scherer AC, Doclo S, Rollwage C, Rennies J. Evaluation of speaker-conditioned target speaker extraction algorithms for hearing-impaired listeners. Trends Hear. 2025;29:23312165251365802. https://doi.org/10.1177/23312165251365802
- Woods DL, Doss Z, Herron TJ, et al. Speech perception in older hearing impaired listeners: benefits of perceptual training. PLoS One. 2015;10(3):e0113965. https://doi.org/10.1371/journal.pone.0113965
- Salorio-Corbetto M, Baer T, Moore BCJ. Comparison of frequency transposition and frequency compression for people with extensive dead regions in the cochlea. Trends Hear. 2019;23:2331216518822206. https://doi.org/10.1177/2331216518822206
- Cox RM, Alexander GC, Johnson J, Rivera I. Cochlear dead regions in typical hearing aid candidates: prevalence and implications for use of high-frequency speech cues. Ear Hear. 2011;32(3):339-348. https://doi.org/10.1097/AUD.0b013e318202e982
- Souza P, Arehart K, Schoof T, Anderson M, Strori D, Balmert L. Understanding variability in individual response to hearing aid signal processing in wearable hearing aids. Ear Hear. 2019;40(6):1280-1292. https://doi.org/10.1097/AUD.0000000000000717
- Arehart KH, Souza P, Baca R, Kates JM. Working memory, age, and hearing loss: susceptibility to hearing aid distortion. Ear Hear. 2013;34(3):251-260. https://doi.org/10.1097/AUD.0b013e318271aa5e
- McCreery RW, Alexander J, Brennan MA, Hoover B, Kopun J, Stelmachowicz PG. The influence of audibility on speech recognition with nonlinear frequency compression for children and adults with hearing loss. Ear Hear. 2014;35(4):440-447. https://doi.org/10.1097/AUD.0000000000000027
- Vandecappelle S, Deckers L, Das N, Ansari AH, Bertrand A, Francart T. EEG-based detection of the locus of auditory attention with convolutional neural networks. Elife. 2021;10:e56481. https://doi.org/10.7554/eLife.56481
Joonpyo Hong, MD is a board-certified otolaryngologist practicing in Korea. This article reflects his clinical interpretation of published research and does not constitute individual medical advice.
This article is not intended to advertise or promote any specific company or product.
For more interesting contents:
https://curiousmd.com/ai-de-escalation-in-hpv-throat-cancer/
https://curiousmd.com/anti-tslp-antibody-nasal-polyps/
https://curiousmd.com/deviated-septum-diagnosis-ai/
https://curiousmd.com/cnn-laryngeal-cancer-diagnosis/
https://curiousmd.com/ai-laryngeal-cancer-detection/
Link out to:
NIDCD — Age-Related Hearing Loss:
https://www.nidcd.nih.gov/health/age-related-hearing-loss
FDA — Authorizes First Over-the-Counter Hearing Aid Software:
https://www.fda.gov/news-events/press-announcements/fda-authorizes-first-over-counter-hearing-aid-software
WHO — Deafness and Hearing Loss (fact sheet):
https://www.who.int/news-room/fact-sheets/detail/deafness-and-hearing-loss