
A patient is told they have cancer—but no one can say where it started. That is the strange reality of cancer of unknown primary (CUP), which accounts for roughly 3–5% of all malignant epithelial tumors [Pavlidis, Cancer of unknown primary site, 2012]. This article walks through what CUP is, how it shows up, where the hidden origin usually hides, how often it stays hidden, and why the answer to “is it better or worse when we can’t find the source?” is more nuanced than it sounds. I’ll also spend extra time on the version of CUP that most often reaches an ENT: a lump in the neck.
What “Cancer of Unknown Primary” Actually Means
CUP is a confirmed metastatic cancer for which standard work-up cannot locate the organ where it began. The diagnosis is made by biopsy of a metastasis, while imaging, endoscopy, and pathology fail to point convincingly to a single source. It is characteristically aggressive, with early and widespread dissemination [Pavlidis, Cancer of unknown primary site, 2012].
The most common tissue type under the microscope is adenocarcinoma, making up about 80% of cases [Pavlidis, Cancer of unknown primary site, 2012]. The rest are largely squamous cell, neuroendocrine, or poorly differentiated carcinomas—and as we’ll see, that histology label carries real prognostic weight.
How CUP Usually Presents
There is no single “classic” symptom, because the presentation depends entirely on where the cancer has spread. A patient might notice a painless lump, swelling from an enlarged lymph node, persistent pain at a metastatic site, or constitutional signs like weight loss and fatigue. Because the disease spreads early, many patients present with symptoms from the metastasis long before any primary site declares itself [Pavlidis, Cancer of unknown primary site, 2012].
That pattern is exactly why CUP is a diagnosis of exclusion: the metastasis is loud, and the origin is silent.
Where the Hidden Primary Usually Lives—and How Often It Stays Hidden
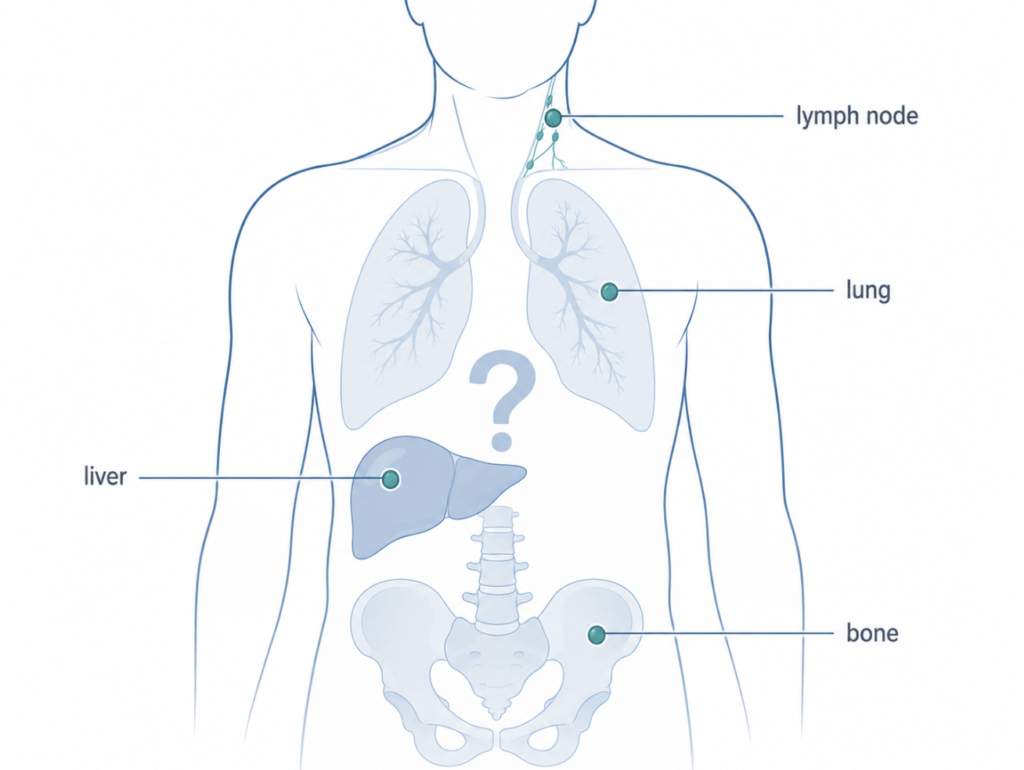
When the primary is eventually found, the pancreatic–hepatobiliary system and lung are among the more common origins. A large Swedish registry analysis specifically identified pancreatic and hepatobiliary cancers as frequent “hidden” primaries behind CUP [Riihimäki, Time trends in survival from cancer of unknown primary, 2013]. The pattern of spread itself offers a clue—as a textbook consequence of venous drainage anatomy rather than a study-specific finding, lung metastases are a strong pointer toward a primary above the diaphragm, while liver metastases point to one below it.
Here is the part patients find hardest to accept: in a substantial share of cases, the primary is never identified, even when the search is thorough. CUP is defined by that failure, and for many patients the source remains unknown through the entire course of illness. This is not sloppy medicine—it reflects how biologically elusive these tumors are.
Prognosis by Primary Site and Subset
Historically, CUP carries a poor prognosis, and outcomes vary widely by histology and metastatic pattern. The single most useful framework divides patients into two groups: a favorable subset (about 20%) and an unfavorable subset (about 80%) [Pavlidis, Cancer of unknown primary site, 2012].
The favorable subset includes presentations that behave like a recognizable cancer in disguise—for example, women with isolated axillary nodes (suggesting breast origin), peritoneal serous adenocarcinomatosis in women (suggesting ovarian origin), squamous cell carcinoma in cervical nodes, and neuroendocrine carcinomas. These patients are treated as if the presumed primary were known, and their responses and survival resemble those of patients with the corresponding known primary tumor [Pavlidis, Cancer of unknown primary site, 2012]. Encouragingly, survival has improved over time for adenocarcinoma CUP and for certain locations such as the peritoneum and ovary [Riihimäki, Time trends in survival from cancer of unknown primary, 2013].
The unfavorable subset—the majority—is treated with empirical chemotherapy, typically platinum- or taxane-based, and outcomes are generally poor [Pavlidis, Cancer of unknown primary site, 2012].
Found vs. Not Found: Which Has the Better Prognosis?
The intuitive question is whether patients do better when the origin is identified. In general, yes—but with an important caveat.
Identifying a primary, especially one that falls into a treatable favorable subset, allows site-directed therapy, and those patients can do as well as patients with a known primary of the same type [Pavlidis, Cancer of unknown primary site, 2012]. So “finding it” usually helps because it unlocks a specific treatment.
The caveat: simply assigning a likely site by gene-expression profiling has not been clearly shown to improve survival. Microarray-based diagnosis is highly sensitive [Pavlidis, Cancer of unknown primary site, 2012], but in a randomized trial, site-specific therapy directed by that profiling did not significantly improve one-year survival compared with empirical paclitaxel–carboplatin chemotherapy [Hayashi, Randomized Phase II Trial Comparing Site-Specific Treatment Based on Gene Expression Profiling With Carboplatin and Paclitaxel for Patients With Cancer of Unknown Primary Site, 2019]. In other words, the benefit comes from finding a tumor you can actually treat differently—not from a label alone.
The ENT Angle: When CUP Arrives as a Lump in the Neck
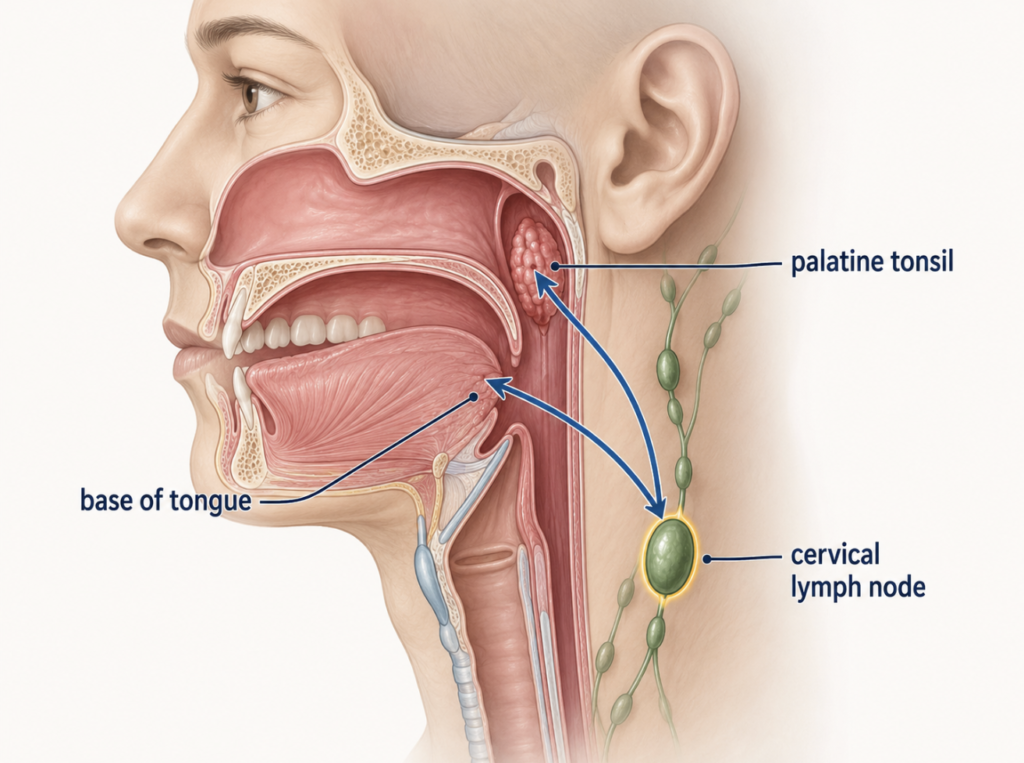
In otolaryngology, CUP often takes a specific and more hopeful form. A patient presents with an enlarged cervical lymph node, the biopsy shows squamous cell carcinoma, and endoscopy plus imaging cannot find the source. The hidden primary in these cases typically lives in the oropharynx—the tonsil or base of tongue—or less often the nasopharynx or hypopharynx.
What makes the head and neck version distinct is the role of viral markers. HPV/p16 status carries strong prognostic and localizing information, and these neck-node CUPs share a risk profile with oropharyngeal squamous cell carcinoma; p16, combined with performance status, can stratify patients into distinct risk groups [Wagner, Predictors for Survival of Patients with Squamous Cell Carcinoma of Unknown Primary in the Head and Neck Region, 2023]. A p16/HPV-positive result points toward an oropharyngeal origin and toward a more favorable course. The current staging system reflects this: under the AJCC eighth edition, p16-positive cervical nodal squamous cell carcinoma with an unknown primary is assigned to the HPV-positive oropharyngeal staging system, which places these patients in a comparatively favorable (lower) stage category [Casswell, Setting the stage: contemporary staging of non-melanomatous skin cancer and implementation of the new American Joint Committee on Cancer eighth edition staging manual, 2019].
The work-up is also more surgical than for CUP elsewhere. Beyond flexible endoscopy and PET/CT, ENT surgeons can perform a diagnostic tonsillectomy or a tongue-base mucosectomy by transoral robotic surgery (TORS) to physically uncover the primary [Civantos, Metastatic squamous cell carcinoma to the cervical lymph nodes from an unknown primary cancer: management in the HPV era, 2020]. In a Danish national cohort, TORS tongue-base mucosectomy revealed the primary tumor in 49% of patients overall, rising to 58% in those with HPV-associated disease [Nielsen, The value of tongue base mucosectomy in the work-up of squamous cell carcinoma of unknown primary, 2024].
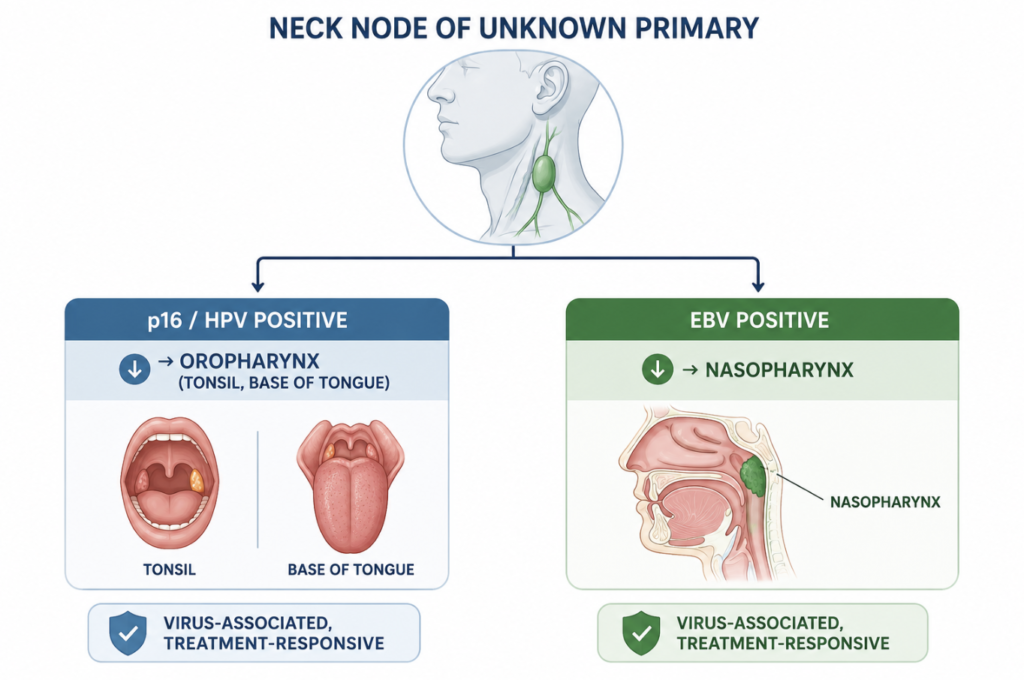
There is an important regional nuance here. Much of the recent literature centers on HPV-driven oropharyngeal cancer, which reflects Western epidemiology—but in East Asia, nasopharyngeal carcinoma is a major hidden primary behind a malignant neck node. Epstein–Barr virus (EBV) is strongly associated with nasopharyngeal carcinoma and serves as a diagnostic and prognostic biomarker [Xue, Epstein-Barr virus DNA in nasopharyngeal carcinoma: a brief review, 2020], so EBV positivity in nodal tissue points toward a nasopharyngeal source. Practically, this means a neck-node work-up in an Asian patient should test for both markers: p16/HPV for an oropharyngeal origin and EBV for a nasopharyngeal one—each pointing to a virus-associated cancer that tends to respond well to treatment.
One pitfall worth flagging: p16 positivity is not unique to HPV-driven oropharyngeal cancer. Nodal metastases from cutaneous head and neck squamous cell carcinoma are frequently p16-positive without any high-risk HPV and without the favorable prognosis that p16 implies in oropharyngeal disease [McDowell, p16-positive lymph node metastases from cutaneous head and neck squamous cell carcinoma: no association with high-risk human papillomavirus or prognosis, 2016]. A positive stain alone should therefore not be treated as proof of an oropharyngeal source; confirmatory HPV testing alongside p16 helps, and the clinical picture, viral testing, and tissue findings all have to line up.
Clinical Perspective
The head and neck is the one place where “we couldn’t find the primary” is often not a sentence of despair. A neck node with squamous histology and a positive HPV/p16 marker frequently behaves like a treatable, favorable cancer—even when the original tumor is never visualized. In Asian practice the same logic extends to EBV: a positive EBV result reframes an “unknown” neck node as a likely nasopharyngeal cancer, which has its own established treatment path. That single distinction is why a neck lump deserves an ENT work-up that actively hunts the oropharynx and nasopharynx rather than stopping at “unknown.”
Key Takeaways
- Cancer of unknown primary is a confirmed metastatic cancer whose origin can’t be found on standard work-up, making up about 3–5% of malignant epithelial tumors.
- Adenocarcinoma is the most common histology (~80%), and pancreatic/hepatobiliary and lung sites are common hidden origins.
- In many patients the primary is never identified, even with thorough evaluation.
- About 20% of patients fall into a favorable subset with outcomes similar to the matching known cancer; the other ~80% have a poorer prognosis.
- Finding a treatable primary generally improves prognosis—but assigning a site by gene profiling alone has not been proven to do so.
- A neck node with squamous histology and positive HPV/p16 is a comparatively favorable form of CUP that ENT surgeons can often trace to the oropharynx.
- In East Asia, including Korea, EBV-positive neck-node disease points to a nasopharyngeal primary, so both HPV/p16 and EBV testing belong in the work-up.
FAQ
What percentage of cancers are cancer of unknown primary? About 3–5% of all malignant epithelial tumors are CUP [Pavlidis, Cancer of unknown primary site, 2012]. It is uncommon but not rare, and it spans many different underlying cancers.
How often is the primary never found? Frequently. CUP is defined by an origin that standard work-up cannot locate, and for a large share of patients the source remains unknown throughout the illness, reflecting how aggressively and early these tumors spread [Pavlidis, Cancer of unknown primary site, 2012].
Is it more dangerous if the primary can’t be found? Usually, yes, because an unidentified origin often means no specific targeted treatment. The main exceptions are favorable subsets—such as HPV-positive neck-node disease—where outcomes can be good even without ever seeing the primary [Pavlidis, Cancer of unknown primary site, 2012; Wagner, Predictors for Survival of Patients with Squamous Cell Carcinoma of Unknown Primary in the Head and Neck Region, 2023].
Can surgery help find the source in a neck-node case? Yes. Diagnostic tonsillectomy and TORS tongue-base mucosectomy can uncover a hidden oropharyngeal primary, with detection reaching roughly half of patients and higher in HPV-associated disease [Nielsen, The value of tongue base mucosectomy in the work-up of squamous cell carcinoma of unknown primary, 2024].
Why does EBV testing matter for a neck lump in Korea? Because nasopharyngeal carcinoma is a common hidden primary in East Asia, and EBV is strongly tied to it. A positive EBV result in nodal tissue points toward a nasopharyngeal origin and a virus-associated cancer with an established treatment path [Xue, Epstein-Barr virus DNA in nasopharyngeal carcinoma: a brief review, 2020].
References
Pavlidis N, Pentheroudakis G. Cancer of unknown primary site. Lancet. 2012;379(9824):1428-1435.
Riihimäki M, Hemminki A, Sundquist K, Hemminki K. Time trends in survival from cancer of unknown primary: small steps forward. Eur J Cancer. 2013;49(10):2403-2410.
Hayashi H, Kurata T, Takiguchi Y, et al. Randomized phase II trial comparing site-specific treatment based on gene expression profiling with carboplatin and paclitaxel for patients with cancer of unknown primary site. J Clin Oncol. 2019;37(7):570-579.
Casswell G, Cavanagh K, Ravi Kumar AS, Giddings C, McDowell L. Setting the stage: contemporary staging of non-melanomatous skin cancer and implementation of the new American Joint Committee on Cancer eighth edition staging manual. Oral Oncol. 2019;98:102-108.
McDowell LJ, Young RJ, Johnston ML, et al. p16-positive lymph node metastases from cutaneous head and neck squamous cell carcinoma: no association with high-risk human papillomavirus or prognosis and implications for the workup of the unknown primary. Cancer. 2016;122(8):1201-1208.
Civantos FJ, Vermorken JB, Shah JP, et al. Metastatic squamous cell carcinoma to the cervical lymph nodes from an unknown primary cancer: management in the HPV era. Front Oncol. 2020;10:593164.
Wagner S, Langer C, Wuerdemann N, et al. Predictors for survival of patients with squamous cell carcinoma of unknown primary in the head and neck region. Cancers (Basel). 2023;15(7):2167.
Xue F, He X. Epstein-Barr virus DNA in nasopharyngeal carcinoma: a brief review. Methods Mol Biol. 2020;2204:99-107.
Nielsen SB, Holm Larsen MH, Channir HI, et al. The value of tongue base mucosectomy in the work-up of squamous cell carcinoma of unknown primary: a Danish national cohort study. Oral Oncol. 2024;159:107083.
Joonpyo Hong, MD is a board-certified otolaryngologist practicing in Korea. This article reflects his clinical interpretation of published research and does not constitute individual medical advice.
Link out to:
National Cancer Institute — Cancer of Unknown Primary Treatment (PDQ®)
American Cancer Society — Cancer of Unknown Primary (CUP)
American Cancer Society — Key Statistics for Cancers of Unknown Primary
For more interesting contents:
https://curiousmd.com/ai-de-escalation-in-hpv-throat-cancer/
https://curiousmd.com/cnn-laryngeal-cancer-diagnosis/
https://curiousmd.com/hpv-oropharyngeal-cancer/
https://curiousmd.com/hpv-vocal-cord-cancer-young-non-smokers/