
A competitive figure skater completes a quadruple jump — four full rotations in under a second — and glides away without a wobble. That same week, a patient recovering from vestibular neuritis feels the room pitch sideways just from rolling over in bed. Same inner ear, opposite tolerance for motion. The difference is not the hardware. It is what each brain has learned to do with the signals that hardware sends.
Can you train your vestibular system? The question comes from two very different directions. Patients who have lost balance function want to know whether they can get it back. Athletes and coaches want to know whether they can push a healthy system to perform beyond baseline. The answer to both depends on the same idea: the vestibular system is trainable, but training changes the brain far more than the sensor.
What “training the vestibular system” actually means
The peripheral vestibular organ is a set of precise motion detectors buried in each inner ear: three semicircular canals that sense rotation and two otolith organs that sense linear movement and gravity. The sensory cells that do this work, the hair cells, regenerate poorly in humans once they are lost. In that sense, the detector hardware is largely fixed for life.
What is not fixed is the brain. The brainstem and cerebellum continuously interpret vestibular input, weigh it against vision and body sensation, and decide how to move the eyes and body in response. This central processing is highly plastic, and it is the real target of every form of vestibular training. When clinicians talk about “retraining balance,” they mean teaching the brain to recalibrate, dampen, or work around vestibular signals — not rebuilding the inner ear.
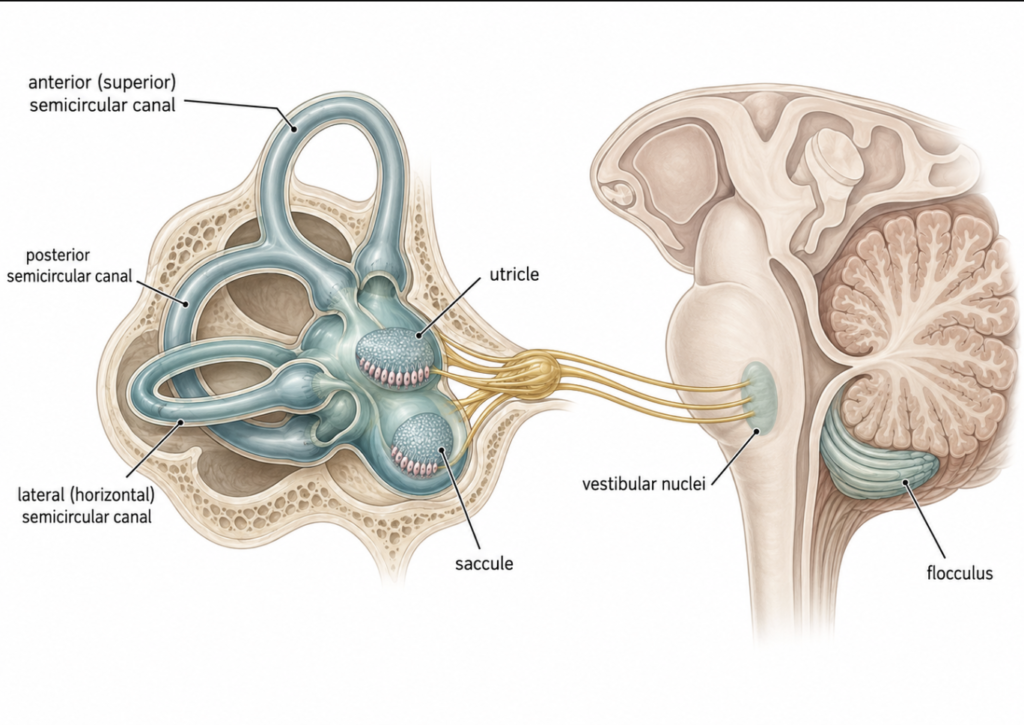
Two structures do much of this work. The vestibular nuclei in the brainstem rebalance their resting activity within days of an injury, which is why the violent spinning of an acute vestibular loss usually settles quickly [David, Posturographic sensory ratios provide evidence for neuroplasticity after computerized vestibular rehabilitation therapy, 2025]. The cerebellum — particularly the flocculus — fine-tunes the reflex itself, adjusting its gain so images stay stable during head movement, and the cerebellar–vestibular nucleus pathway is the leading model for how that gain is modulated [Maheu, Enhanced vestibulo-ocular reflex suppression in dancers during passive high-velocity head impulses, 2018].
That single principle explains why the same biology serves two very different goals. For an injured patient, plasticity restores function that was lost. For a healthy athlete, plasticity refines function that already works. One engine, two destinations.
Part 1 — Restoring lost function: vestibular rehabilitation
When the balance system breaks
Vestibular hypofunction happens when one or both inner ears stop delivering reliable motion information. It can arrive suddenly, as in vestibular neuritis, an inflammation of the vestibular nerve that leaves people with severe vertigo, nausea, and unsteadiness. It can also creep in gradually with age, a decline sometimes called presbyvestibulopathy. This is not a rare problem. An estimated one-third of adults in the United States have some form of vestibular dysfunction, and the incidence rises with age [Hall, Vestibular Rehabilitation for Peripheral Vestibular Hypofunction, 2022].
That acute spinning is the part that tends to settle on its own. The stubborn part is what comes after: lingering imbalance, blurred vision during head movement, and a fear of moving that can quietly shrink a person’s life. Those chronic symptoms are exactly what rehabilitation targets.
The three mechanisms the brain uses to recover
Vestibular rehabilitation is not a single exercise. It is a strategy to trigger three distinct forms of neural adaptation.
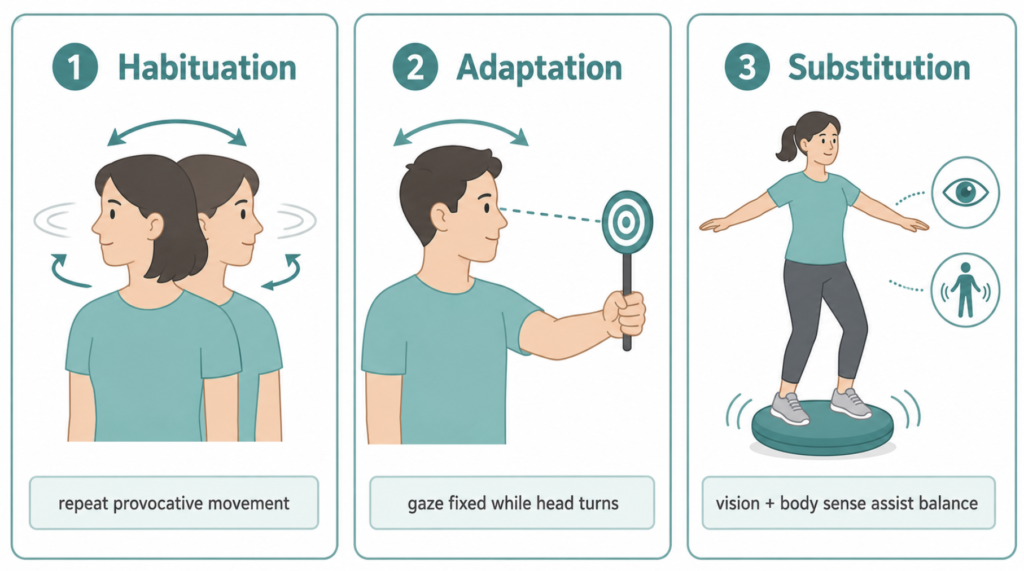
The first is habituation — deliberately repeating the movements that provoke dizziness so the brain gradually stops overreacting to them. The second is adaptation, best represented by gaze-stabilization exercises: a patient fixes their eyes on a target while turning the head, which recalibrates the vestibulo-ocular reflex so images stop slipping on the retina. The third is substitution, training the brain to lean more on vision and body sensation to cover for the damaged vestibular channel. Underlying all three is sensory reweighting, the brain’s ongoing adjustment of how much it trusts each source of balance information [Gimmon, Neuro-vestibular rehab: new developments, 2026].
A concrete example ties these together. Inducing a temporary drop in reflex gain briefly increases postural sway, and that sway then normalizes as the brain reweights its sensory inputs — a visible demonstration of central compensation happening in real time [Gimmon, Neuro-vestibular rehab: new developments, 2026].
Does it work?
The evidence here is unusually strong for a rehabilitation field. A rigorous clinical practice guideline reviewing decades of trials concluded that there is strong evidence vestibular physical therapy reduces symptoms and improves gaze and postural stability in people with unilateral and bilateral vestibular hypofunction, and that clinicians should offer it [Hall, Vestibular Rehabilitation for Peripheral Vestibular Hypofunction, 2022]. The same guideline gets specific about dosing — several short bouts of gaze-stabilization exercise daily over a few weeks — and, tellingly, notes that eye movements practiced in isolation, without head motion, do not help. The head has to move for adaptation to occur.
The gains also last. In a trial using computerized vestibular retraining, patients showed durable improvement in the sensory ratios that reflect reliance on vestibular information, with benefits still present 10 to 12 months later. Notably, the patients who started with the most disability improved the most [David, Posturographic sensory ratios provide evidence for neuroplasticity after computerized vestibular rehabilitation therapy, 2025].
None of this progress has to be guessed at. Clinicians quantify it with objective tests: the video head impulse test (vHIT) and rotational chair testing measure vestibulo-ocular reflex gain directly, while computerized posturography tracks how well the brain is reweighting vision, body sensation, and vestibular input. These are the same tools that reveal balance adaptations in the first place, and they let a clinician confirm that rehabilitation is moving the needle rather than relying only on how a patient says they feel.
Clinical Perspective. In practice, the most important message for patients is that rehabilitation is not an optional extra to wait out alongside “natural healing.” The brain compensates best when it is given the right, repeated stimulus, and passively avoiding provocative movement often prolongs symptoms rather than protecting against them. The finding that more-affected patients tend to gain the most runs against many people’s assumption that severe cases are hopeless — often the opposite is true.
Modern tools are widening access
The core exercises are decades old, but delivery is changing. Incremental reflex-adaptation devices, gamified mobile applications with wearable sensors, virtual reality programs, and telehealth supervision are all expanding home-based rehabilitation, and adjuncts such as galvanic vestibular stimulation and vibrotactile feedback are being explored as complements [Gimmon, Neuro-vestibular rehab: new developments, 2026]. The principle stays the same; the packaging is becoming easier to stick with.
Part 2 — Building higher-than-normal function: the athlete question
Restoring lost balance is one thing. Can a healthy person train past their baseline for the split-second control that sports demand? Here the evidence is genuinely interesting, and more nuanced than most training blogs suggest.
Elite athletes really do have measurably different vestibular function
This is not just marketing. When researchers measured the reflexes of competitive figure skaters on a rotational chair, the skaters’ vestibulo-ocular reflex gain was 27 to 32 percent lower than matched controls, and provocative rotation triggered far less motion sickness in the skaters [Tanguy, Vestibulo-ocular reflex and motion sickness in figure skaters, 2008]. Years of spinning had produced measurable vestibular habituation — the brain had turned down a reflex that would otherwise make rapid rotation intolerable.
There is a deeper mechanism behind why spinning makes most people dizzy at all. A central circuit called velocity storage works like an integrator that keeps the brain’s sense of rotation going after the head has actually stopped — the lingering “still spinning” feeling that drags out dizziness and drives motion sickness. Repeated vestibular stimulation can shorten this circuit’s time constant, and in one habituation study that shortening cut motion sickness sharply and lasted for weeks, with no change in reflex gain [Dai, Prolonged reduction of motion sickness sensitivity by visual-vestibular interaction, 2011]. The skaters above adapted by a different route — their reflex gain fell while their time constant held steady [Tanguy, Vestibulo-ocular reflex and motion sickness in figure skaters, 2008] — a reminder that the brain has more than one way to tame rotation.
Dancers show a related adaptation. On the video head impulse test (vHIT), trained dancers demonstrated an enhanced ability to suppress the reflex during fast head movements, an effect strongest in those with more than ten years of training [Maheu, Enhanced vestibulo-ocular reflex suppression in dancers during passive high-velocity head impulses, 2018].

The key nuance: sometimes added control, not just a dulled reflex
It would be easy to conclude that elite training simply blunts the vestibular system, but a small, preliminary study suggests something more precise. In trained dancers, the resting reflex gain was entirely normal — no different from non-dancers, and even their reflex-suppression scores did not separate the groups outright. What distinguished the dancers instead were subtler signs of learned control: their suppression ability tracked their preferred turning direction, and those with more than fifteen years of training produced earlier anti-compensatory eye movements, around 75 milliseconds. The authors read this as enhanced voluntary control developing on top of an intact reflex [Jha, Dance Training and the Neuroplasticity of the Vestibular-Ocular Reflex, 2025].
That detail matters. Elite training does not appear to degrade the reflex that keeps vision stable in daily life. Instead it layers a faster, top-down control system on top of a healthy reflex — the brain learns when to let the reflex run and when to override it. For a dancer spotting a turn or a gymnast landing a twist, that voluntary override is the skill.
The brain adapts structurally, too
These changes are not limited to eye reflexes. Balance experts — gymnasts, acrobats, slackliners — outperformed sedentary adults on spatial perspective-taking, and the authors note that sustained balance training induces structural plasticity in brain regions that process visual and vestibular self-motion [Hötting, Balance Expertise Is Associated with Superior Spatial Perspective-Taking Skills, 2021]. Training the balance system appears to reshape the neural tissue that supports spatial cognition.
But does training transfer to performance? The honest limits
For healthy athletes, three findings need to be held together.
First, balance training reliably improves balance. A meta-analysis found that neuromuscular training substantially improved athletes’ balance ability, with a large pooled effect [Shi, Effects of Neuromuscular Training on Athletes’ Balance Ability, 2025]. Training on unstable surfaces produced similar gains on standing-balance tests [Yin, The effects of instability training on balance and jump performance in athletes, 2025].
Second, that improvement does not automatically convert into raw athletic power. In the same instability-training analysis, balance measures improved clearly — a large effect on single-leg stance — but transfer to jump performance was limited, with no significant effect on the countermovement jump [Yin, The effects of instability training on balance and jump performance in athletes, 2025]. Better balance scores do not guarantee a higher vertical leap.
Third, where balance training pays off most consistently is injury prevention. Programs that include balance exercises cut ankle injury rates in soccer players, with balance exercises alone associated with roughly a 42 percent reduction [Al Attar, Injury prevention programs that include balance training exercises reduce ankle injury rates among soccer players, 2022]. The same approach reduced anterior cruciate ligament injuries by 58 percent, with an even larger effect in female athletes [Su, Injury risk reduction programs including balance training reduce the incidence of anterior cruciate ligament injuries in soccer players, 2025].
There is one more limit worth naming: the adaptations are specific. The reflex changes in dancers and skaters scale with years of training and track the exact demands of their discipline — even their preferred direction of rotation [Jha, Dance Training and the Neuroplasticity of the Vestibular-Ocular Reflex, 2025; Maheu, Enhanced vestibulo-ocular reflex suppression in dancers during passive high-velocity head impulses, 2018]. A skater’s tolerance for spinning does not hand them a general balance superpower for every other task.
Clinical Perspective. For a healthy athlete, the practical takeaway is to treat balance work as a specific tool, not a magic upgrade. It is one of the best-supported interventions available for reducing ankle and knee injuries, and it clearly sharpens the balance qualities a sport depends on. But it should be built to mirror the actual demands of the sport, because the brain adapts to what it practices — and it should be positioned as a complement to strength and skill work, not a substitute for either.
So, can you train your vestibular system?
Yes — and the reason holds across the whole spectrum. The injured patient and the elite athlete sit at two ends of the same process. In both cases, the trainable element is central: how the brain calibrates the vestibulo-ocular reflex, how it weighs competing sensory inputs, and how much voluntary control it layers on top. In neither case is anyone growing new inner-ear sensors.
That is why the same exercise principles — repeated, specific, progressively challenging movement — drive both recovery and refinement. Give the brain the right stimulus often enough, and it adapts. The destination differs, but the mechanism is shared.
Key Takeaways
- Vestibular function is trainable, but the change happens in the brain’s processing, not through regeneration of inner-ear sensors.
- Vestibular rehabilitation works through three mechanisms — habituation, adaptation, and substitution — and strong evidence supports it for people with vestibular hypofunction.
- Rehabilitation gains can last a year or more, and patients with greater initial disability often improve the most.
- Elite athletes show real vestibular adaptation, but it takes different forms — a turned-down, habituated reflex in figure skaters versus enhanced voluntary control over a normal reflex in dancers — rather than a single universal change.
- For healthy athletes, balance training reliably improves balance and sharply reduces ankle and ACL injuries, though transfer to raw power output is limited and adaptations are specific to the trained task.
FAQ
Can a damaged vestibular system recover? Yes. While lost inner-ear sensor cells do not meaningfully regenerate, the brain can compensate through vestibular rehabilitation, and strong evidence shows this reduces dizziness and improves gaze and postural stability in people with vestibular hypofunction. Recovery relies on retraining central processing rather than repairing the sensor, and consistent, movement-based exercise is what drives it.
Can healthy people improve their balance beyond normal? Yes, within limits. Balance and neuromuscular training reliably improve balance performance in athletes, and elite performers such as dancers and skaters develop measurable vestibular adaptations over years of practice. The gains are real but specific to the trained demands, so they do not translate into a general, all-purpose balance advantage.
Does balance training make you better at sports? Partly. Balance training clearly improves balance-related qualities and is one of the most effective tools for preventing ankle and knee injuries, which keeps athletes available to perform. Its transfer to raw performance measures like jump height is more limited, so it is best used as a targeted complement to strength and skill training.
Can you “strengthen” your inner ear? Not in the muscular sense. The inner ear’s balance sensors are not a muscle you build up, and their cells regenerate poorly. What you can strengthen is the brain’s ability to interpret, adapt to, and voluntarily control the signals those sensors send — which is what every effective balance program actually trains.
References
Al Attar WSA, Khaledi EH, Bakhsh JM, Faude O, Ghulam H, Sanders RH. Injury prevention programs that include balance training exercises reduce ankle injury rates among soccer players: a systematic review. J Physiother. 2022;68(3):165-173.
Dai M, Raphan T, Cohen B. Prolonged reduction of motion sickness sensitivity by visual-vestibular interaction. Exp Brain Res. 2011;210(3-4):503-513.
David EA, Shahnaz N. Posturographic sensory ratios provide evidence for neuroplasticity after computerized vestibular rehabilitation therapy in a single group interventional trial. J Neuroeng Rehabil. 2025;22(1):81.
Gimmon Y, Gordon CR. Neuro-vestibular rehab: new developments. Curr Opin Neurol. 2026;39(1):83-87.
Hall CD, Herdman SJ, Whitney SL, Anson ER, Carender WJ, Hoppes CW, et al. Vestibular Rehabilitation for Peripheral Vestibular Hypofunction: An Updated Clinical Practice Guideline From the Academy of Neurologic Physical Therapy of the American Physical Therapy Association. J Neurol Phys Ther. 2022;46(2):118-177.
Hötting K, Rogge AK, Kuhne LA, Röder B. Balance Expertise Is Associated with Superior Spatial Perspective-Taking Skills. Brain Sci. 2021;11(11):1401.
Jha RH, Piker EG, Scalzo M, Trinidad D. Dance Training and the Neuroplasticity of the Vestibular-Ocular Reflex: Preliminary Findings. Brain Sci. 2025;15(4):355.
Maheu M, Behtani L, Nooristani M, Delcenserie A, Champoux F. Enhanced vestibulo-ocular reflex suppression in dancers during passive high-velocity head impulses. Exp Brain Res. 2018;237(2):411-416.
Shi K, Xiang M, Shi H, Duan R. Effects of Neuromuscular Training on Athletes’ Balance Ability: A Meta-Analysis. Sports Med. 2025;56(1):201-213.
Su W, Wang J, Ying Y, Lu B, Liu H, Zhou Z, et al. Injury risk reduction programs including balance training reduce the incidence of anterior cruciate ligament injuries in soccer players: a systematic review and meta-analysis. J Orthop Surg Res. 2025;20(1):248.
Tanguy S, Quarck G, Etard O, Gauthier A, Denise P. Vestibulo-ocular reflex and motion sickness in figure skaters. Eur J Appl Physiol. 2008;104(6):1031-1037.
Yin X, Wu Q, Zhao X, Shi L, Li L. The effects of instability training on balance and jump performance in athletes: A systematic review and meta-analysis. Physiol Rep. 2025;13(21):e70650.
Joonpyo Hong, MD is a board-certified otolaryngologist practicing in Korea. This article reflects his clinical interpretation of published research and does not constitute individual medical advice.
For more interesting contents:
https://curiousmd.com/computerized-stabilometry-balance-test/
https://curiousmd.com/room-spins-when-youre-drunk/
https://curiousmd.com/motion-sickness-aftereffects/
https://curiousmd.com/senaptec-strobe-vestibular-neuroplasticity/
Link out to:
Balance Disorders — National Institute on Deafness and Other Communication Disorders (NIDCD): https://www.nidcd.nih.gov/health/balance-disorders
Vestibular Rehabilitation Therapy (VRT) — Vestibular Disorders Association (VeDA): https://vestibular.org/article/diagnosis-treatment/treatments/vestibular-rehabilitation-therapy-vrt/
Vestibular Rehabilitation Resources — Academy of Neurologic Physical Therapy, APTA:
https://www.neuropt.org/special-interest-groups/vestibular-rehabilitation/resources