
Picture a 72-year-old who hears the doorbell, the microwave, and the neighbor’s dog without trouble — then sits down at a family dinner and catches maybe half of what is said. Age-related hearing loss (presbycusis) is one of the most common conditions of aging, and left untreated it tracks with isolation, depression, and higher dementia risk [Gates, Presbycusis, 2005; Uchida, Age-related hearing loss and cognitive decline – The potential mechanisms linking the two, 2018]. But the everyday complaint is rarely “the world got quieter.” It is “I can hear you — I just can’t understand you.” Three specific changes in the aging cochlea explain that gap, and only one of them is about volume.

The Physiology of Age-Related Hearing Loss
Age-related hearing loss(Presbycusis) is not a single failure but the slow breakdown of several cochlear structures at once [Gates, Presbycusis, 2005]. Three parts of the inner ear carry most of the burden: the sensory hair cells that turn sound into nerve signals, the spiral ganglion neurons that carry those signals to the brain, and the stria vascularis, the cochlea’s metabolic “battery” [Keithley, Pathology and mechanisms of cochlear aging, 2019].
Each failure has a distinct consequence. When the stria vascularis atrophies, the electrical potential that powers the cochlea drops, so the outer hair cells can no longer amplify soft sounds — and because that amplification matters most at high frequencies, those fade first. Direct loss of outer hair cells removes the amplifier as well, while degeneration of the auditory neurons blunts the ear’s ability to encode speech, especially in noise [Keithley, Pathology and mechanisms of cochlear aging, 2019].
Underneath all of this sits cellular aging. Decades of oxidative stress, mitochondrial DNA damage, noise exposure, and declining blood supply gradually wear these structures down, which is why presbycusis is progressive and, so far, irreversible [Keithley, Pathology and mechanisms of cochlear aging, 2019]. Those physiological changes are what produce the three everyday problems the rest of this article explains.
Age-Related Hearing Loss Turns the Volume Down Unevenly
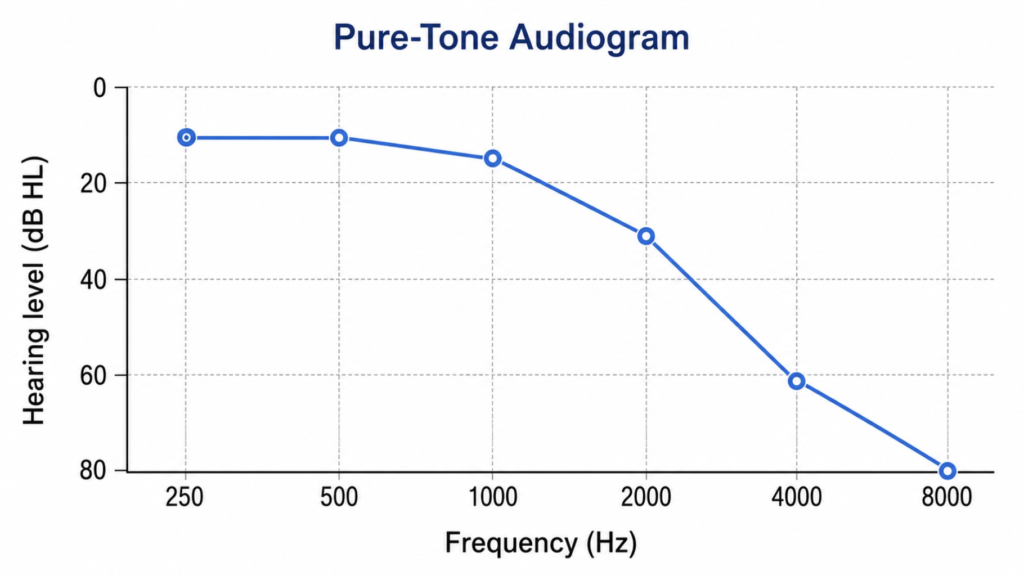
Presbycusis raises hearing thresholds from the top of the frequency range downward, so high pitches fade first. The reason is anatomical: the outer hair cells at the base of the cochlea, which encode high frequencies, are the most vulnerable to a lifetime of aging, noise, and metabolic stress [Keithley, Pathology and mechanisms of cochlear aging, 2019].
That uneven loss matters because speech is not acoustically uniform. Vowels are low-pitched and loud; consonants like /s/, /f/, /th/, and /k/ are high-pitched and faint — and consonants carry most of the meaning. When the high frequencies drop out, “fifteen” and “fifty” blur into each other, and a sentence arrives as a stream of vowels with the edges sanded off. The listener hears that someone spoke, but the information-carrying sounds are already gone.
Loudness Recruitment: Too Quiet, Then Suddenly Too Loud
Here is the counterintuitive part. Even though soft sounds are inaudible, once a sound crosses the raised threshold its loudness grows abnormally fast — a phenomenon called loudness recruitment. The usable window between “I can’t hear that” and “that’s uncomfortably loud” becomes narrow.
The mechanism is a lost gain control. A healthy cochlea compresses an enormous range of sound intensities into a manageable internal range, and that compression is the work of the outer hair cells. When those cells are damaged, the response becomes more linear, so each step up in sound level produces an outsized jump in perceived loudness [Oxenham, Cochlear compression: perceptual measures and implications for normal and impaired hearing, 2003]. This is exactly why shouting backfires: to a person with recruitment, a whisper is nothing and a raised voice is jarring. “Don’t shout — I’m not deaf” turns out to be a physiologically accurate complaint.
Reduced Frequency Selectivity: The Real Reason Words Dissolve
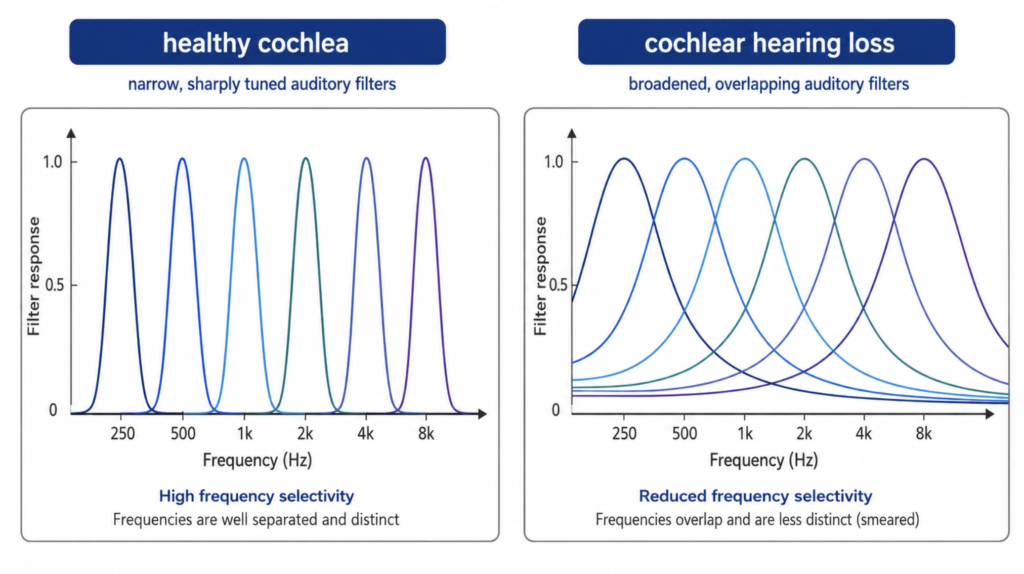
The change that best explains “hearing without understanding” is the least visible on a standard hearing test. A healthy inner ear behaves like a bank of finely tuned filters, each responding to a narrow band of frequencies, which lets the brain pull one voice out of the clatter of a restaurant. Outer hair cell damage broadens those filters, so neighboring frequencies smear together and the target voice is no longer cleanly separated from the background [Moore, Frequency selectivity and temporal resolution in normal and hearing-impaired listeners, 1985].
This is why the quiet-room audiogram can mislead. In a silent booth, one-on-one, the person may do fine; drop them into a dinner party and comprehension collapses, because the noise now falls inside the same broadened filters as the speech. Reduced frequency resolution, not raw volume loss, is a leading driver of real-world speech-in-noise difficulty, alongside age-related changes in central auditory processing [Moore, Frequency selectivity and temporal resolution in normal and hearing-impaired listeners, 1985; Keithley, Pathology and mechanisms of cochlear aging, 2019].
Clinical Perspective
These three deficits together explain why the old advice — “just turn it up” — was never enough, and why modern hearing aids do far more than amplify. They apply compression to counter recruitment (boosting quiet sounds more than loud ones) and, increasingly, AI-driven noise reduction and directional processing to help lift speech out of background noise.
It is worth being honest about the ceiling, though. When researchers simulate all three problems at once — raised thresholds, recruitment, and broadened filters — and then apply well-fitted linear amplification, listeners recover only part of their lost speech-in-noise performance; a stubborn gap remains [Nejime, Simulation of the effect of threshold elevation and loudness recruitment combined with reduced frequency selectivity on the intelligibility of speech in noise, 1997]. Amplification can make sounds audible again, but it cannot un-smear a blurred frequency map. That is precisely where AI noise reduction is both most promising and most limited: it can clean up the signal arriving at a damaged ear, but it does not restore the ear’s lost resolution. The practical lessons are unglamorous — realistic expectations, careful hearing-aid fitting, and not waiting years before acting.
Key Takeaways
- Age-related hearing loss is three problems at once: sounds get quieter, loudness grows harsher, and frequencies blur together.
- High-frequency loss erases faint consonants first, so speech is heard but not understood.
- Loudness recruitment means soft sounds vanish while loud sounds turn uncomfortable — which is why shouting rarely helps.
- Reduced frequency selectivity, not simple volume loss, is a leading reason speech falls apart in noisy rooms.
- A near-normal audiogram can coexist with real difficulty understanding speech in noise.
FAQ
Why can I hear people but not understand their words? Because two things fail together. High-frequency loss removes the faint consonants that distinguish words, while broadened cochlear filters let background noise smear into the speech signal. The result is audible but unintelligible speech, especially in groups or noisy rooms — even when the overall volume seems fine.
Does turning up the volume fix age-related hearing loss? Not fully. Volume restores audibility, but it cannot sharpen the ear’s blurred frequency tuning or undo loudness recruitment. That is why shouting — or a hearing aid that only amplifies — leaves speech-in-noise problems behind, and why compression and noise reduction are built into modern devices.
What is loudness recruitment? It is the abnormally rapid growth of loudness once a sound becomes audible. The window between too soft and too loud narrows, so quiet speech is missed while loud sounds feel harsh. It reflects the loss of the cochlea’s natural compression when outer hair cells are damaged.
References
Gates GA, Mills JH. Presbycusis. Lancet. 2005;366(9491):1111-1120.
Keithley EM. Pathology and mechanisms of cochlear aging. J Neurosci Res. 2019;98(9):1674-1684.
Moore BCJ. Frequency selectivity and temporal resolution in normal and hearing-impaired listeners. Br J Audiol. 1985;19(3):189-201.
Nejime Y, Moore BCJ. Simulation of the effect of threshold elevation and loudness recruitment combined with reduced frequency selectivity on the intelligibility of speech in noise. J Acoust Soc Am. 1997;102(1):603-615.
Oxenham AJ, Bacon SP. Cochlear compression: perceptual measures and implications for normal and impaired hearing. Ear Hear. 2003;24(5):352-366.
Uchida Y, Sugiura S, Nishita Y, Saji N, Sone M, Ueda H. Age-related hearing loss and cognitive decline – the potential mechanisms linking the two. Auris Nasus Larynx. 2018;46(1):1-9.
Joonpyo Hong, MD is a board-certified otolaryngologist practicing in Korea. This article reflects his clinical interpretation of published research and does not constitute individual medical advice.
For more interesting contents:
https://curiousmd.com/ai-speech-clarification-hearing-loss/
https://curiousmd.com/otc-hearing-aids-2026/
https://curiousmd.com/airpods-hearing-test-what-it-can-and-cannot-do/
https://curiousmd.com/airpods-hearing-test-ent-perspective/
Link out to:
https://www.nidcd.nih.gov/health/age-related-hearing-loss
https://www.who.int/news-room/fact-sheets/detail/deafness-and-hearing-loss
https://www.hearingloss.org/understanding-hearing-loss/types-causes-and-treatments/age-related-hearing-loss