
Hyperbaric oxygen for sudden hearing loss is one of the first add-on treatments patients reach for when standard therapy falls short—but does it actually work? Sudden sensorineural hearing loss (SSNHL) strikes an estimated 5 to 20 people per 100,000 every year, often overnight and usually in one ear, and most patients never learn the cause. This article explains what hyperbaric oxygen therapy (HBOT) does for the inner ear, who is most likely to benefit, and why the honest answer is “sometimes, under the right conditions.”

What Hyperbaric Oxygen Therapy Is
HBOT places the whole body inside a pressurized chamber—commonly 2.0 to 2.5 atmospheres absolute (ATA)—while the patient breathes 100% oxygen for roughly an hour per session. At that pressure, far more oxygen dissolves directly into the blood plasma rather than riding on hemoglobin. This dissolved oxygen can reach tissue that normal circulation struggles to supply.
That mechanism is why HBOT is established for conditions like decompression sickness, carbon monoxide poisoning, gas gangrene, radiation tissue injury, and chronic non-healing wounds such as diabetic foot ulcers. In each case, the common thread is the same: get oxygen into tissue that is starved of it.
Why the Inner Ear Might Care About Oxygen
The cochlea has an unusually high oxygen demand and a famously delicate blood supply. One leading hypothesis for idiopathic SSNHL is microvascular compromise—reduced blood flow and resulting cochlear hypoxia. Measurements show that perilymph oxygen tension rises significantly during HBOT [Psillas, Hyperbaric Oxygen Therapy in the Treatment of Sudden Sensorineural Hearing Loss, 2023].
On paper, this is a logical match: an oxygen-hungry organ, a possible oxygen-supply problem, and a therapy designed to flood tissue with oxygen. The clinical question is whether that logic translates into measurable hearing recovery.
Where HBOT Sits in the Guidelines
Here is the single most important point for patients to understand: HBOT is not a stand-alone cure for sudden hearing loss. Corticosteroids—oral, intravenous, or injected through the eardrum (intratympanic)—remain the primary treatment.
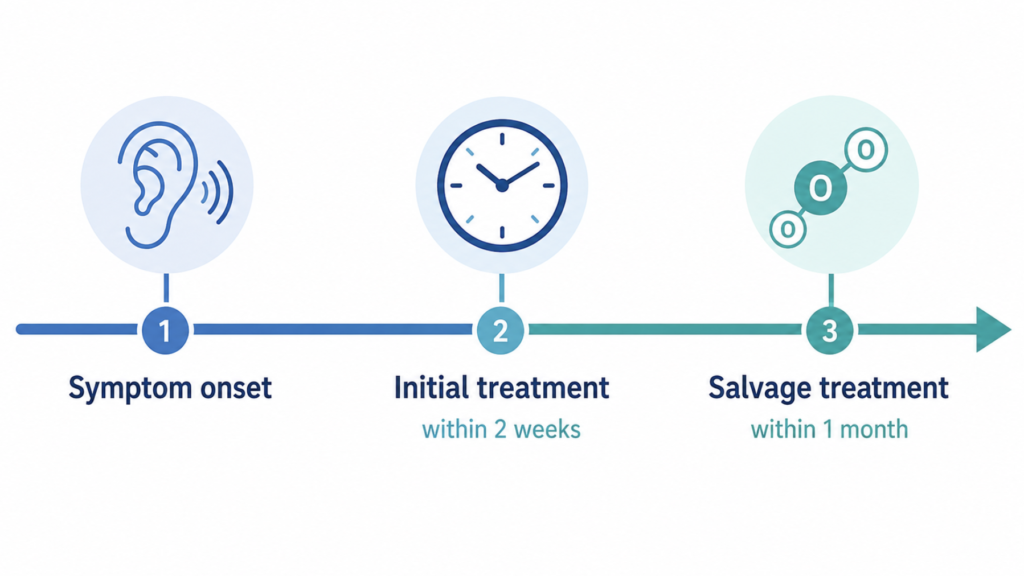
The 2019 American Academy of Otolaryngology–Head and Neck Surgery (AAO-HNS) Clinical Practice Guideline classifies HBOT as an optional therapy, and only when combined with steroid therapy [Chandrasekhar, Clinical Practice Guideline: Sudden Hearing Loss (Update), 2019]. Two specific scenarios are described:
- Initial therapy: HBOT combined with steroids within 2 weeks of onset.
- Salvage therapy: HBOT combined with steroids within 1 month of onset, when initial treatment has produced incomplete recovery.
“Optional” is a deliberate word. It signals that the evidence is real but not strong enough to make the therapy routine for everyone. The decision belongs in a shared conversation between clinician and patient.
Timing Is the Hidden Variable
The effect of HBOT is time-dependent, and its benefit shrinks as treatment is delayed. Some authors argue the window is even tighter than the guideline suggests, recommending that HBOT ideally begin within 24 to 48 hours of onset [Bayoumy, Hyperbaric Oxygen Therapy vs Medical Therapy for Sudden Sensorineural Hearing Loss, 2019].
The practical takeaway is blunt: sudden hearing loss is an emergency, not a “wait and see” symptom. Whatever the role of HBOT turns out to be in a given case, every day of delay erodes the potential upside of all treatments, steroids included.
Who Is Most Likely to Benefit
The evidence points consistently toward two groups. A systematic review and meta-analysis of 19 studies concluded that adding HBOT to standard medical therapy is a reasonable option, particularly for patients with severe-to-profound hearing loss at baseline and for those receiving it as salvage treatment with a prolonged course [Rhee, Addition of Hyperbaric Oxygen Therapy vs Medical Therapy Alone for Idiopathic Sudden Sensorineural Hearing Loss, 2018].
In other words, the worse the starting hearing level, the more measurable room there is for HBOT to add value on top of steroids. Patients with mild loss—who also have the highest spontaneous recovery rate—show little additional gain. HBOT is also worth discussing when high-dose steroids are contraindicated, such as in poorly controlled diabetes, though it does not replace steroids in that situation.
Clinical Perspective The strongest signal in the literature is not “HBOT helps everyone” but “HBOT helps a defined subset, early.” A severe or profound loss with vertigo, treated within the first two weeks alongside steroids, is the scenario where the combination has the best supporting rationale. Mild, late-presenting cases are where expectations should be tempered, because the marginal benefit is small and the logistics are demanding.
How a Course Looks, and What the Risks Are
A typical protocol uses 2.0 to 2.5 ATA for about 60 minutes of oxygen breathing per session, often 5 sessions per week for a total of 10 to 20 sessions. That means near-daily hospital visits—a real burden on time, cost, and adherence.
HBOT is generally safe, but it is not risk-free. The most common issue is middle-ear or sinus barotrauma from the pressure change; patients with poor Eustachian tube function are especially vulnerable and need counseling beforehand. Other effects include transient nearsightedness and, rarely, oxygen-toxicity seizures. Untreated pneumothorax and certain bullous lung diseases are contraindications, which is why a pre-treatment screen matters.
What the Evidence Says About Hyperbaric Oxygen for Sudden Hearing Loss
The case for HBOT is genuine but qualified. The same meta-analysis that found benefit in severe and salvage cases drew immediate commentary about the extensive heterogeneity of the underlying studies—differing protocols, small samples, and inconsistent outcome definitions make pooled conclusions fragile [Lammers, Extensive Heterogeneity in the Meta-analysis of Hyperbaric Oxygen Therapy for Idiopathic Sudden Sensorineural Hearing Loss, 2019]. A Cochrane review likewise found improvements in hearing but cautioned about the clinical significance and the quality of the evidence base [Bennett, Hyperbaric Oxygen for Idiopathic Sudden Sensorineural Hearing Loss and Tinnitus, 2012].
More recent syntheses point in the same direction without resolving the uncertainty. A 2022 meta-analysis found HBOT added to medical therapy associated with greater odds of hearing recovery [Joshua, Hyperbaric Oxygen Therapy for Patients With Sudden Sensorineural Hearing Loss, 2022], and a 2025 meta-analysis similarly concluded the combination is likely to benefit hearing recovery [Alter, Hyperbaric Oxygen and Sudden Sensorineural Hearing Loss, 2025]. Both, however, land on the same caveat: protocols and data reporting vary so widely across studies that standardization is needed before the size of the benefit can be stated with confidence.
This is exactly why the guideline says “optional” rather than “recommended.” The therapy is promising for the right patient at the right time, not a guaranteed rescue.
A Therapy Worth Watching—With Realistic Expectations
HBOT is drawing growing interest across sensory medicine. Beyond sudden hearing loss, it is studied in tinnitus and is an accepted treatment for central retinal artery occlusion, and the underlying idea—rescuing oxygen-starved sensory tissue—keeps generating new research questions across otolaryngology and ophthalmology. That trajectory is worth following.
But interest is not the same as proof. As with most adjunctive therapies, the sensible posture is conservative and selective: reserve HBOT for the patients and time windows where the evidence is strongest, pair it with—never instead of—standard steroid therapy, and frame the expected benefit accurately. Understood clearly and used with realistic expectations, HBOT is a reasonable tool. Marketed as a cure, it sets patients up for disappointment.
Key Takeaways
- HBOT for sudden hearing loss is an adjunct to steroid therapy, not a stand-alone or first-line treatment.
- The AAO-HNS 2019 guideline lists HBOT as an “optional” therapy: initial use within 2 weeks of onset, salvage use within 1 month.
- The clearest benefit appears in severe-to-profound hearing loss and in salvage cases started early.
- The evidence is positive but heterogeneous, which is why the recommendation stays at “optional” rather than “recommended.”
- Sudden hearing loss is a medical emergency; earlier treatment improves the odds for every available option.
FAQ
Does hyperbaric oxygen therapy cure sudden hearing loss? No. HBOT is an add-on to steroid treatment, not a cure. It may improve recovery in selected patients—especially those with severe loss treated early—but steroids remain the primary therapy and many patients also recover partially on their own.
How quickly do I need to start treatment? As fast as possible. Sudden hearing loss is treated as an emergency, and HBOT’s benefit declines with delay—guidelines favor starting within 2 weeks of onset, and some experts argue for the first 24 to 48 hours.
Is HBOT safe for my ears? For most people, yes, but the pressure change can cause middle-ear barotrauma, particularly with poor Eustachian tube function. Untreated pneumothorax and some lung diseases are contraindications, so a screening evaluation is done before starting.
Why isn’t HBOT used for everyone with hearing loss? Because the benefit is modest and concentrated in specific groups, the studies are inconsistent, and a full course requires near-daily sessions with real cost and time demands. Guidelines therefore label it “optional,” to be considered through shared decision-making.
References
- Chandrasekhar SS, Tsai Do BS, Schwartz SR, et al. Clinical practice guideline: sudden hearing loss (update). Otolaryngol Head Neck Surg. 2019;161(1 Suppl):S1-S45.
- Rhee TM, Hwang D, Lee JS, Park J, Lee JM. Addition of hyperbaric oxygen therapy vs medical therapy alone for idiopathic sudden sensorineural hearing loss: a systematic review and meta-analysis. JAMA Otolaryngol Head Neck Surg. 2018;144(12):1153-1161.
- Bayoumy AB, van der Veen EL, de Ru JA. Hyperbaric oxygen therapy vs medical therapy for sudden sensorineural hearing loss. JAMA Otolaryngol Head Neck Surg. 2019;145(8):699-700.
- Lammers MJ, Lea J, Westerberg BD. Extensive heterogeneity in the meta-analysis of hyperbaric oxygen therapy for idiopathic sudden sensorineural hearing loss. JAMA Otolaryngol Head Neck Surg. 2019;145(5):483-484.
- Psillas G. Hyperbaric oxygen therapy in the treatment of sudden sensorineural hearing loss. J Clin Med. 2023;12(4):1515.
- Bennett MH, Kertesz T, Perleth M, Yeung P, Lehm JP. Hyperbaric oxygen for idiopathic sudden sensorineural hearing loss and tinnitus. Cochrane Database Syst Rev. 2012;(10):CD004739.
- Joshua TG, Ayub A, Wijesinghe P, Nunez DA. Hyperbaric oxygen therapy for patients with sudden sensorineural hearing loss: a systematic review and meta-analysis. JAMA Otolaryngol Head Neck Surg. 2022;148(1):5-11.
- Alter IL, Hamiter M, Han J, Leu CS, Usseglio J, Lalwani AK. Hyperbaric oxygen and sudden sensorineural hearing loss: a systematic review and meta-analysis. Laryngoscope. 2025. Online ahead of print.
Joonpyo Hong, MD is a board-certified otolaryngologist practicing in Korea. This article reflects his clinical interpretation of published research and does not constitute individual medical advice.
For more interesting contents:
https://curiousmd.com/earbud-hearing-loss-ent-guide/
https://curiousmd.com/airpods-hearing-test-what-it-can-and-cannot-do/
https://curiousmd.com/airpods-hearing-test-ent-perspective/
Link out to:
AAO-HNS – Clinical Practice Guideline: Sudden Hearing Loss (Update):
https://www.entnet.org/quality-practice/quality-products/clinical-practice-guidelines/sudden-hearing-loss-update/
NIDCD (NIH) – Sudden Deafness:
https://www.nidcd.nih.gov/health/sudden-deafness
Rhee et al. 2018 – HBOT meta-analysis:
https://pubmed.ncbi.nlm.nih.gov/30267033/
Cochrane Review – HBOT for idiopathic SSNHL and tinnitus:
https://pubmed.ncbi.nlm.nih.gov/23076907/