
Permanent hearing loss affects roughly 1 to 3 of every 1,000 newborns, yet a baby cannot raise a hand when it hears a tone. The entire field of objective audiometry exists to answer one question: how do you measure hearing in someone who cannot—or will not—tell you what they hear? This guide covers the three core objective hearing tests—otoacoustic emissions (OAE), the auditory brainstem response (ABR), and the auditory steady-state response (ASSR)—what each one measures, which patient it fits, and how to read them when they disagree.
Hearing: The Most Objectively Measurable Sense
Most clinical sensory testing depends on the patient reporting what they perceive: reading an eye chart, naming a smell, describing a touch. Hearing is the exception. Electrophysiologic tests can estimate a frequency-specific threshold with no voluntary response at all, accurately enough to serve as a surrogate for behavioral testing in infants. That capability is the reason universal newborn hearing screening is feasible.
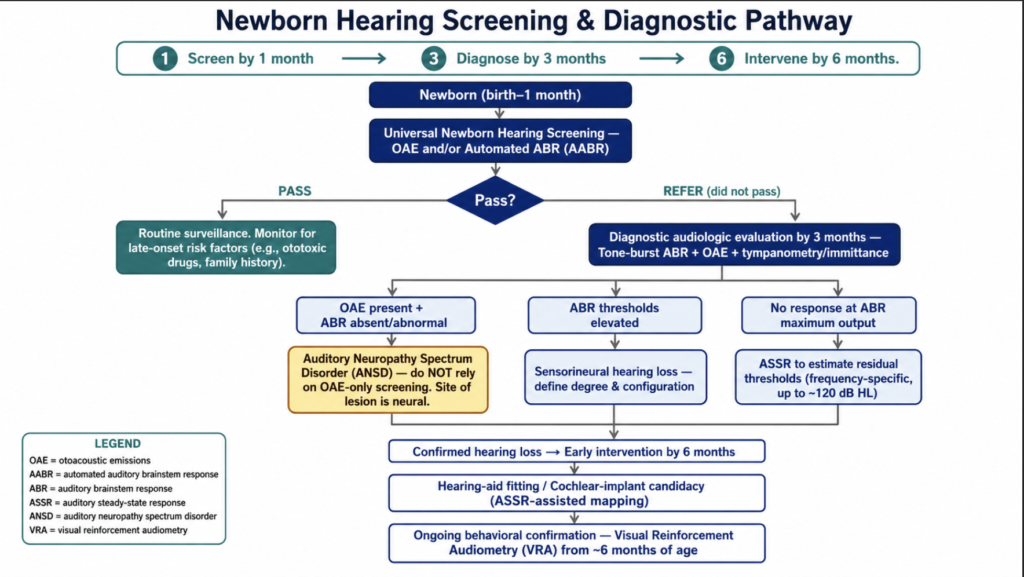
The stakes justify the effort. Children identified by 6 months of age and enrolled in early intervention show significantly better language outcomes than those identified later, an advantage that held across degrees of loss, communication modes, and socioeconomic strata [Yoshinaga-Itano, Language of early- and later-identified children with hearing loss, 1998]. Objective tests are what make identification before 6 months possible in the first place.
To be precise, hearing is not literally the only objectively measurable sense—vision has a counterpart. Visual evoked potentials can estimate visual acuity, and a systematic review of 155 studies confirms the VEP spatial-frequency limit works as an objective acuity estimator, especially in pre-verbal children [Hamilton, VEP estimation of visual acuity, 2020]. That same review notes the estimate is variable and depends heavily on age-stratified calibration. Hearing’s objective threshold measurement is simply more standardized and more routinely deployed at population scale, while smell, taste, and touch remain, in everyday practice, largely subjective.
The Three Objective Tests
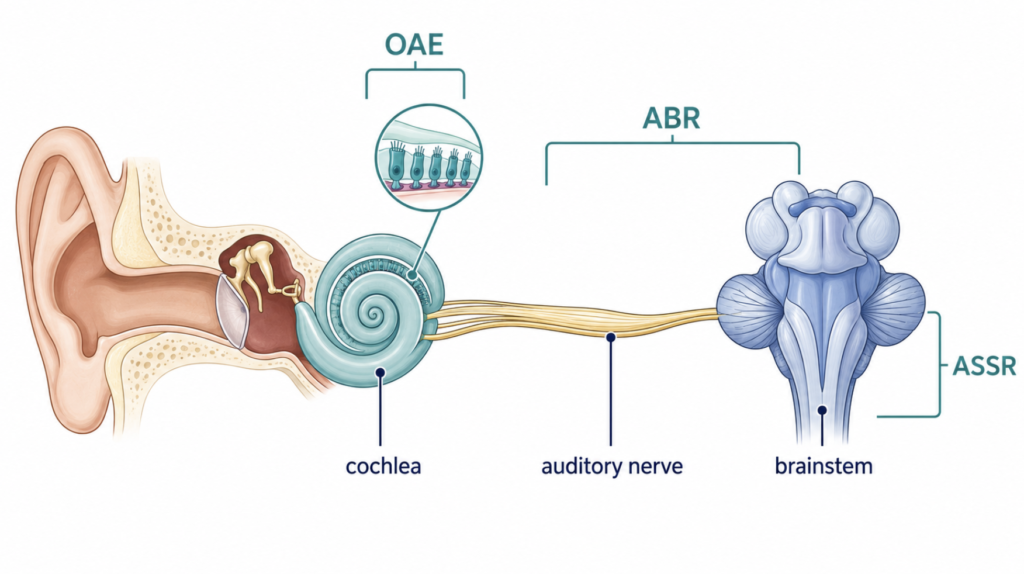
Each test interrogates a different point along the auditory pathway, and conflating them is the most common source of misreading. The table below is the 30-second version; the sections that follow add the clinical nuance.
| Test | What it measures | Threshold estimate? | Main clinical use |
|---|---|---|---|
| OAE (TEOAE / DPOAE) | Outer hair cell function in the cochlea | No | Screening, cochlear monitoring |
| ABR / BERA | Neural synchrony from auditory nerve to brainstem | Yes (with tone bursts) | Thresholds + retrocochlear screening |
| ASSR | Response locked to amplitude/frequency-modulated tones | Yes (frequency-specific) | Frequency-specific thresholds, severe loss |
OAE — TEOAE & DPOAE
OAEs are faint sounds the cochlea itself produces, generated by the outer hair cells and recorded with a probe in the ear canal. The phenomenon was first described by David Kemp, who identified a slowly decaying acoustic response present in normal ears but absent in ears with cochlear deafness [Kemp, Stimulated acoustic emissions from within the human auditory system, 1978]. Two evoked types dominate clinical use: the transient-evoked OAE (TEOAE), triggered by a click, and the distortion-product OAE (DPOAE), triggered by two simultaneous tones and read at a predictable distortion frequency.
The limitation deserves stating plainly: an OAE is not a hearing test. It confirms the outer hair cells are working—nothing more. It gives no threshold, and it says nothing about the auditory nerve behind the cochlea.
Within those bounds, OAEs do more than screen newborns. Because they isolate outer hair cell function, they help localize a sensorineural loss to the cochlea rather than the nerve behind it, and they detect cochlear damage earlier than the pure-tone audiogram—DPOAEs in particular flag injury from ototoxic drugs (cisplatin, aminoglycosides) or noise before a threshold shift appears, with greater sensitivity than audiometry for early change [Probst, Clinical monitoring using otoacoustic emissions, 1993]. A present OAE in an ear the patient reports as deaf also points toward a non-organic or exaggerated component. A “pass,” though, never proves normal hearing.
ABR / BERA
The ABR records the electrical volley traveling from the auditory nerve through the brainstem in roughly the first 10 milliseconds after a sound, captured by scalp electrodes as a series of waves labeled I through V. With tone-burst stimuli it estimates frequency-specific thresholds; with click stimuli and attention to wave latencies it screens for retrocochlear pathology such as a vestibular schwannoma. An adult with one-sided tinnitus and asymmetric hearing, for example, might undergo ABR to flag a possible tumor on the nerve before proceeding to imaging.
The same response also works as a real-time monitor in the operating room. During hearing-preservation surgery for vestibular schwannoma, ABR tracks the integrity of the cochlear nerve, and loss of the response is a meaningful predictor of postoperative hearing loss [Gu, Diagnostic accuracy of intraoperative brainstem auditory evoked potential for predicting hearing loss after vestibular schwannoma surgery, 2022].
ASSR
The ASSR presents tones modulated in amplitude or frequency and detects—by statistics rather than visual waveform reading—whether ongoing electrical activity locks onto that modulation. Its practical advantage shows up at the severe-to-profound end. When a click-ABR is flat at maximum output, the ASSR can still extract residual hearing: in a series of children with no recordable click-ABR, ASSR thresholds tracked behavioral thresholds closely and identified ears with usable residual hearing that the ABR alone had missed [Rance, Steady-state evoked potential and behavioral hearing thresholds in children with absent click-evoked ABR, 1998].
Two features extend that role. ASSR can drive frequency-specific stimuli to very high intensities—up to roughly 120 dB HL, beyond the usable ceiling of click-ABR—and it can test both ears across several frequencies at once. Together these make it well suited to mapping residual hearing in cochlear implant candidates and to ear-specific hearing-aid fitting in infants with severe-to-profound loss [Swanepoel, Estimations of auditory sensitivity for young cochlear implant candidates using the ASSR, 2004].
Which Objective Test for Which Patient?
Each test earns its place in different situations, and each carries limits worth keeping in view. The table sorts the three by indication, strength, and limitation.
| Test | When it’s the right test | Strengths | Key limitations |
|---|---|---|---|
| OAE (TEOAE / DPOAE) | Newborn screening; ototoxicity and noise monitoring; cochlear vs. retrocochlear site-of-lesion; flagging non-organic loss | Fast, non-invasive, no sedation; detects cochlear damage before the audiogram shifts; fully objective | Not a threshold test; blocked by middle-ear fluid or canal debris; blind to the nerve, so it misses auditory neuropathy spectrum disorder (ANSD) |
| ABR / BERA | Newborn screening (AABR); infant frequency-specific thresholds; retrocochlear screening; intraoperative cochlear-nerve monitoring | Estimates thresholds; assesses neural conduction to the brainstem; standardized and widely available | Click-ABR has poor frequency specificity; flat at maximum output can’t grade severe vs. profound; needs sedation in children and takes time |
| ASSR | Residual hearing in severe, profound, or total loss; cochlear-implant candidacy; ear-specific hearing-aid fitting | Frequency-specific; tests to very high output (~120 dB HL); both ears and several frequencies at once; statistical auto-detection | Needs sleep or sedation in children; less accurate near normal or mild thresholds; characterizes ANSD less well than ABR’s waveform |
A few combinations follow directly from the table:
- Newborn screening → OAE + AABR, read as a cross-check, since OAE alone misses ANSD.
- Severe, profound, or total loss with possible residual hearing → ASSR, with tone-burst ABR.
- Early ototoxic or noise-induced damage → DPOAE, before the audiogram shifts.
- Asymmetric loss or one-sided tinnitus → ABR for retrocochlear screening.
- Suspected non-organic or exaggerated loss → ABR or ASSR, supported by OAE.
Clinical Perspective
No single objective test should stand alone. The cross-check principle—pairing any one result with an independent measure—was formalized decades ago precisely because individual tests mislead [Jerger, The cross-check principle in pediatric audiometry, 1976]. In practice that means OAE and ABR are interpreted together, never in isolation.
The clearest reason why is ANSD. In these patients the outer hair cells function, so OAEs are present, yet neural transmission is disordered, so the ABR is absent or grossly abnormal—the pattern originally characterized as auditory neuropathy by Starr and colleagues, who found preserved emissions sitting alongside absent or distorted brainstem responses [Starr, Auditory neuropathy, 1996]. An OAE-only screen passes these children. Only the combination catches them.
Key Takeaways
- OAE measures outer hair cell function and screens the cochlea, but it is not a threshold test and cannot tell you how well someone hears.
- ABR and ASSR estimate frequency-specific hearing thresholds without any patient response, which is what makes universal newborn screening possible.
- ASSR outperforms conventional ABR at the severe-to-profound end—through higher maximum stimulus output (~120 dB HL) and simultaneous multi-frequency testing—recovering residual hearing that click and tone-burst ABR can miss.
- Normal OAEs alongside an absent or abnormal ABR is the signature of ANSD—and the reason no single test should be trusted alone.
- Hearing is the sense with the most standardized, routinely deployed objective threshold measurement; vision’s VEP equivalent exists but is less calibrated.
FAQ
What is the difference between OAE, ABR, and ASSR?
They measure different points along the hearing pathway. OAE checks the cochlea’s outer hair cells, ABR checks neural transmission from the auditory nerve through the brainstem, and ASSR estimates frequency-specific thresholds from the response to modulated tones. OAE is a screening and cochlear-monitoring tool, while ABR and ASSR can actually estimate how loud a sound must be before the auditory system responds.
Is hearing the only sense with objective clinical measurement?
No, but it is the most standardized. Vision can be assessed objectively with visual evoked potentials, which estimate acuity in patients who cannot read a chart. Hearing stands out because objective tests estimate frequency-specific thresholds reliably enough to serve as an accurate surrogate for behavioral testing in infants—until techniques like visual reinforcement audiometry (VRA) become developmentally feasible—and to anchor population-wide newborn screening, a level of routine deployment the other senses do not match.
Can objective tests replace a standard audiogram?
Not exactly; they estimate it. ABR and ASSR predict behavioral thresholds closely, but they measure the auditory system’s electrical response, not conscious hearing. In anyone who can respond reliably, behavioral audiometry remains the reference. Objective tests earn their place when behavioral testing is impossible or unreliable: infants, sedated patients, or suspected non-organic loss.
Which objective test is used for newborns?
Newborn screening typically uses automated ABR (AABR), OAE, or both together. Pairing the two as a cross-check is more accurate than either alone, because OAE by itself misses auditory neuropathy spectrum disorder (ANSD), where the cochlea works but the nerve does not. Babies who do not pass screening are referred for full diagnostic ABR.
References
- Jerger JF, Hayes D. The cross-check principle in pediatric audiometry. Arch Otolaryngol. 1976;102(10):614-20.
- Kemp DT. Stimulated acoustic emissions from within the human auditory system. J Acoust Soc Am. 1978;64(5):1386-91.
- Starr A, Picton TW, Sininger Y, Hood LJ, Berlin CI. Auditory neuropathy. Brain. 1996;119(Pt 3):741-53.
- Rance G, Dowell RC, Rickards FW, Beer DE, Clark GM. Steady-state evoked potential and behavioral hearing thresholds in a group of children with absent click-evoked auditory brain stem response. Ear Hear. 1998;19(1):48-61.
- Yoshinaga-Itano C, Sedey AL, Coulter DK, Mehl AL. Language of early- and later-identified children with hearing loss. Pediatrics. 1998;102(5):1161-71.
- Hamilton R, Bach M, Heinrich SP, Hoffmann MB, Odom JV, McCulloch DL, Thompson DA. VEP estimation of visual acuity: a systematic review. Doc Ophthalmol. 2020;142(1):25-74.
- Probst R, Harris FP, Hauser R. Clinical monitoring using otoacoustic emissions. Br J Audiol. 1993;27(2):85-90.
- Gu F, Yang X, Wang Z, Tan X, Xue T, Chen Z, Wang Z, Chen G. Diagnostic accuracy of intraoperative brainstem auditory evoked potential for predicting hearing loss after vestibular schwannoma surgery. Front Neurol. 2022;13:1018324.
- Swanepoel D, Hugo R. Estimations of auditory sensitivity for young cochlear implant candidates using the ASSR: preliminary results. Int J Audiol. 2004;43(7):377-82.
Joonpyo Hong, MD is a board-certified otolaryngologist practicing in Korea. This article reflects his clinical interpretation of published research and does not constitute individual medical advice.