
Earbud hearing loss has shifted from a workplace problem to a personal-listening problem. A 2022 systematic review estimated that up to 1.35 billion people aged 12–34 may be at risk of hearing loss from personal listening devices and loud venues worldwide [Dillard, Prevalence and global estimates of unsafe listening practices in adolescents and young adults, 2022]. The audiometric signature is increasingly familiar: a quiet dip at 4 kHz, the classic fingerprint of noise-induced hearing loss — now appearing in young heavy earphone users rather than industrial workers.
This article explains what prolonged earbud use actually does to the inner ear, what early signs to watch for, and a practical daily protocol — without asking anyone to give up their AirPods.

What Prolonged Earbud Use Does to the Inner Ear
The human cochlea contains approximately 15,000 sensory hair cells — about 12,000 outer hair cells and 3,500 inner hair cells. Once permanently damaged, none of these cells regenerate. In-ear devices deliver sound directly into the canal at a few millimeters from the eardrum, so a volume that feels “moderate” is often well above what the cochlea evolved to handle for hours at a stretch.
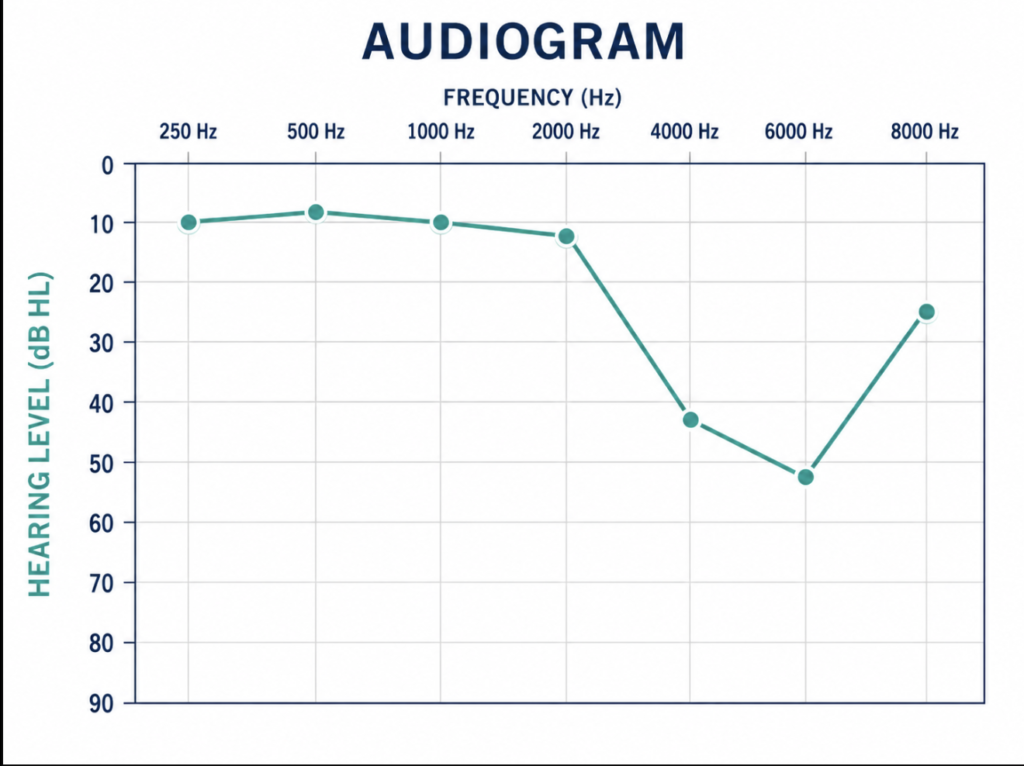
Damage almost always begins in the high-frequency region — most commonly the 4–6 kHz range, sometimes extending up to 16 kHz. This is the audiometric notch seen on a hearing test. It is silent at first: speech in quiet sounds normal, music sounds fine, but consonants like s, f, and th start to blur in noisy environments long before the listener notices anything is wrong [Chodankar, Hearing risk in the digital age: a systematic review on recreational audio device use among youth, 2025].
The Volume–Time Trade-off
For recreational listening, the World Health Organization recommends keeping weekly sound exposure under approximately 80 dB averaged across the week. The trade-off is non-linear: every 3 dB roughly halves the safe time.
| Volume | Approximate Safe Weekly Limit |
|---|---|
| 70 dB (normal conversation) | Not problematic in general situation |
| 80 dB | ~40 hours/week |
| 85 dB | ~12.5 hours/week |
| 95 dB | ~75 minutes/week |
| 100 dB (roughly 70% smartphone volume) | ~15 minutes/week |
Source: WHO-ITU Safe Listening Devices and Systems standard.
The figure that surprises most listeners is the last row. Many modern earbuds at 70% volume already sit around 100 dB sound pressure level, which means the entire weekly recreational budget can be spent during a single morning commute.
Five Early Signs Worth Taking Seriously
These early signs are commonly reported in the audiology and otolaryngology literature:
- Asking people to repeat themselves in restaurants — speech-in-noise difficulty is often the first complaint.
- A brief ringing or “stuffed” feeling after taking earbuds out (temporary threshold shift — animal studies suggest the underlying damage may not be temporary).
- Difficulty with consonants s, f, th — the high-frequency signature.
- Steady volume creep — turning music up over weeks without noticing.
- Tinnitus that outlasts the listening session — when the ringing persists for hours or days, it is a clinical signal, not an inconvenience.
Hidden Hearing Loss: Why a Normal Test Isn’t Enough
Landmark research by Kujawa and Liberman demonstrated that noise exposure can cause permanent damage to the synapses between cochlear hair cells and auditory nerve fibers — even when audiogram thresholds return to normal [Kujawa, Adding insult to injury: cochlear nerve degeneration after “temporary” noise-induced hearing loss, 2009]. This phenomenon is known as cochlear synaptopathy, or “hidden hearing loss.”
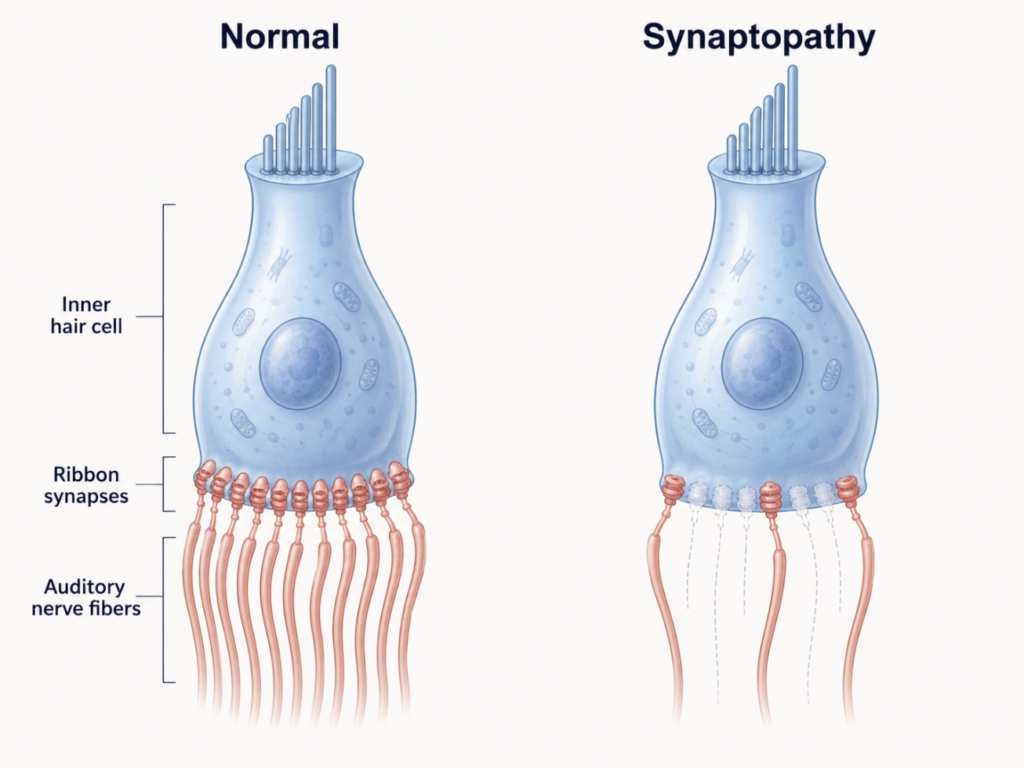
In practical terms, a young heavy earphone user with a “normal” hearing test may already have lost auditory nerve fibers needed to understand speech in noise. The standard pure-tone audiogram cannot detect this damage; it shows up only as a real-world struggle to follow conversations in busy environments [Liberman, Cochlear synaptopathy in acquired sensorineural hearing loss: manifestations and mechanisms, 2017]. For heavy earphone users, a normal hearing test should not be read as a clean bill of hearing health.
Does Noise-Cancelling Actually Protect You?
A common misconception is that active noise cancellation (ANC) protects hearing. It does not — at least not directly. ANC reduces ambient low-frequency noise, which allows the listener to lower their volume and still hear music clearly. Whether they actually do is the question.
The practical test is simple: if someone standing an arm’s length away can hear what’s playing in earbuds, the volume is likely above 85 dB and well into damage territory.
The 60/60 Rule
The most useful daily heuristic is the 60/60 rule, widely recommended by hearing health organizations and consistent with WHO Make Listening Safe principles:
- Keep volume at no more than 60% of maximum.
- Listen for no more than 60 minutes at a time.
- Then take a break before resuming.
It is deliberately simple because most listeners cannot read decibel meters in real time. On most smartphones, 60% volume sits around 75–85 dB — a range the cochlea can tolerate for meaningful daily listening when broken into sessions.

Using Built-in AI Tools to Monitor Yourself
This is one area where current technology genuinely helps. Several consumer tools now provide real exposure data:
- iOS Health → Headphone Audio Levels: tracks 7-day rolling average decibel exposure through AirPods and supported headphones. If the average is consistently above 80 dB, exposure is too high.
- Apple Watch Noise app: real-time ambient decibel monitoring; helpful for concerts, gyms, and transit.
- hearWHO (free, from the World Health Organization): uses validated digits-in-noise testing to screen hearing status on a smartphone.
These tools do not replace an audiogram — they cannot detect hidden hearing loss, and they vary in accuracy depending on the device and environment. But for heavy earphone users, they provide something previously unavailable: a way to know whether daily exposure is in a reasonable range.
When to See an ENT
Some signs warrant clinical evaluation rather than another app:
- Sudden hearing loss in one ear — sudden sensorineural hearing loss is a medical emergency. Outcomes are best when treatment begins within 72 hours, and clinical guidelines recommend evaluation as soon as possible and ideally within 2 weeks.
- Tinnitus persisting beyond one week, especially if it disrupts sleep or concentration.
- Hearing change after a single high-intensity event (concert, headphone malfunction, loud headset feedback).
- A family member repeatedly asking you to turn the TV down.
A clinic visit typically includes pure-tone audiometry, tympanometry, and sometimes otoacoustic emissions — together they reveal patterns a smartphone test cannot.
Key Takeaways
- Noise-induced hearing loss is permanent; damaged cochlear hair cells do not regenerate.
- High-frequency loss at 4–6 kHz is the earliest sign and is usually silent at first.
- The 60/60 rule — 60% volume, 60 minutes maximum, then a break — is the most practical daily heuristic.
- A normal audiogram does not rule out cochlear synaptopathy (“hidden hearing loss”) in heavy earphone users.
- Active noise cancellation protects hearing only if the listener actually lowers the volume; it is not protection by itself.
- iOS Headphone Audio Levels and hearWHO give heavy users a free, daily way to monitor exposure.
FAQ
How many hours of earbuds per day is safe? Hearing health guidance suggests keeping daily listening to around 60–90 minutes at 60% volume, with breaks in between. Beyond that, cumulative risk rises, and the risk depends as much on volume as on time.
Can earbud hearing loss be reversed? No. Once cochlear hair cells or auditory nerve synapses are permanently damaged, current medicine cannot restore them. Early prevention is the only effective intervention.
Is sleeping with earbuds in bad for hearing? Yes. Eight or more hours of continuous canal occlusion increases the risk of cerumen impaction and ear canal infection, and any sustained sound exposure during sleep occurs without the user able to monitor or adjust it.
Does noise-cancelling prevent hearing damage? Indirectly, by removing the need to raise volume above ambient noise. ANC by itself does not reduce sound levels reaching the eardrum from the music or content being played.
When should I see an ENT instead of using a hearing app? See an ENT urgently for sudden hearing loss in one ear, tinnitus that persists beyond a week, or hearing change after a single high-intensity sound event. Apps screen — they do not diagnose.
References
- Dillard LK, Arunda MO, Lopez-Perez L, Martinez RX, Jiménez L, Chadha S. Prevalence and global estimates of unsafe listening practices in adolescents and young adults: a systematic review and meta-analysis. BMJ Glob Health. 2022;7(11):e010501.
- Kujawa SG, Liberman MC. Adding insult to injury: cochlear nerve degeneration after “temporary” noise-induced hearing loss. J Neurosci. 2009;29(45):14077-14085.
- Liberman MC, Kujawa SG. Cochlear synaptopathy in acquired sensorineural hearing loss: manifestations and mechanisms. Hear Res. 2017;349:138-147.
- Chodankar S, et al. Hearing risk in the digital age: a systematic review on recreational audio device use among youth. Int J Res Med Sci. 2025;13(12):5450-5453.
- World Health Organization, International Telecommunication Union. Safe listening devices and systems: a WHO-ITU standard. Geneva: WHO; 2019.
- World Health Organization. World Report on Hearing. Geneva: WHO; 2021.
Joonpyo Hong, MD is a board-certified otolaryngologist practicing in Korea. This article reflects his clinical interpretation of published research and does not constitute individual medical advice.
For more interesting contents:
https://curiousmd.com/music-genre-and-hearing-loss/
https://curiousmd.com/shingles-vaccine-and-hearing-loss/
https://curiousmd.com/objective-hearing-tests-abr-assr-oae/
Link out to:
https://www.who.int/activities/making-listening-safe
https://support.apple.com/en-us/108803
https://www.who.int/teams/noncommunicable-diseases/sensory-functions-disability-and-rehabilitation/hearwho