
A new brain-controlled hearing aid concept — published this week in Nature Neuroscience — may be the most direct response yet to a problem that current devices have never solved: following a conversation in a noisy room. More than 430 million people worldwide live with disabling hearing loss (WHO, 2021), and for many who rely on hearing devices, multi-talker environments remain consistently difficult regardless of how advanced the technology becomes.
Here is what the research actually demonstrates, why it matters for people with hearing loss and cochlear implants, and what remains years from clinical use.
The Problem No Hearing Aid Has Solved
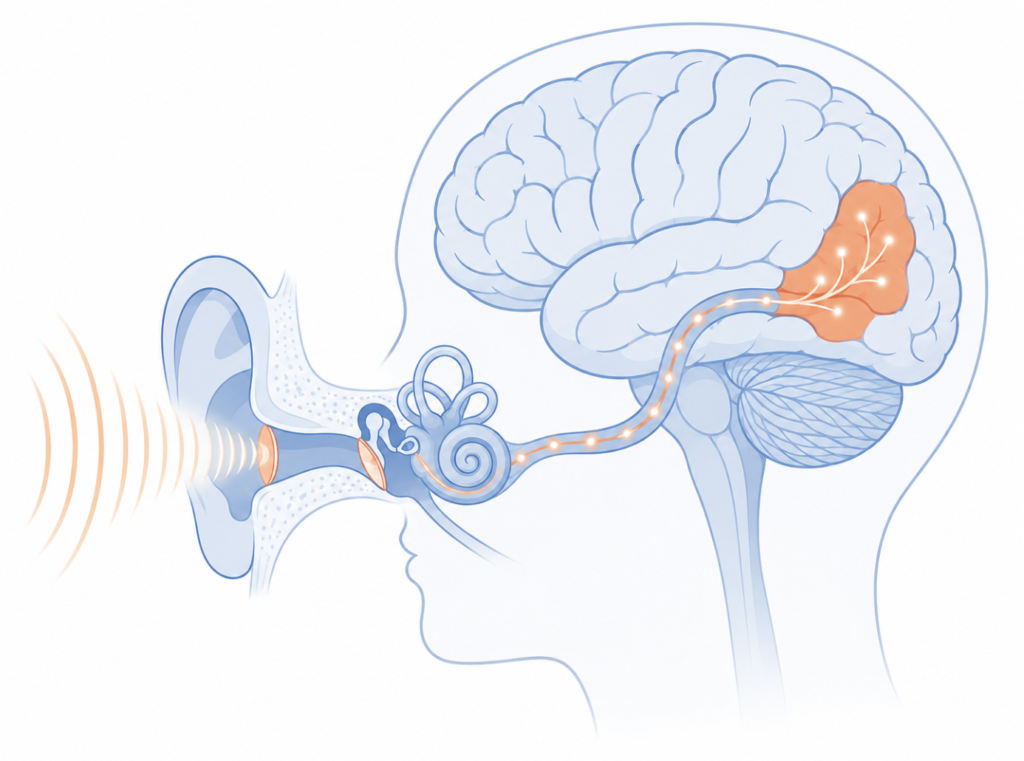
The “cocktail party problem” has a name precisely because it describes something so universally frustrating. In a room full of competing voices, a person with normal hearing can tune into one speaker almost effortlessly. The auditory cortex reconstructs that speaker’s voice and suppresses the rest — a feat of selective attention that happens automatically.
Current hearing aids, even those with advanced AI processors, cannot replicate this. They excel at reducing stationary background noise — traffic, air conditioning, ambient hum — but when two people speak at the same volume from similar directions, the devices have no mechanism to decide which voice to amplify. Both get boosted. Both get mixed together. The listener is left to do the hard work alone.
This is not a software problem that better algorithms will fix tomorrow. It is a fundamental limitation: the device has no access to what the listener wants to hear.
What the New System Does
The 2026 study from Columbia University’s Neural Acoustic Processing Lab built a closed-loop system to address exactly this gap [Choudhari et al., Nat Neurosci, 2026].
The system works in three steps:
- Record — Intracranial electrodes capture high-resolution signals from the auditory cortex in real time.
- Decode — A linear regression model identifies which of two competing voices the listener is focusing on, by matching the temporal envelope of neural activity to the acoustic envelope of each speaker.
- Amplify — The attended voice is boosted; the competing voice is reduced. Dynamically, in real time.
The system correctly identified the attended speaker approximately 90% of the time. When switched on, participants showed measurable improvements in speech comprehension and reduced listening effort compared to the unaided condition. The system also tracked self-initiated attention shifts — when participants spontaneously decided to switch focus between speakers, the system followed.
This builds on foundational work by the same group, who showed in 2012 that the human auditory cortex encodes the attended speaker’s voice so robustly that it can be decoded computationally [Mesgarani and Chang, Nature, 2012].
Why the Study Design Matters — and Its Limits
The four participants in this study were patients undergoing neurosurgery for epilepsy. They already had intracranial electrodes placed on the cortical surface as part of their treatment — not implanted for the purpose of this experiment. All had self-reported normal hearing.
This design allowed exceptional signal quality. Intracranial recordings capture neural activity at a resolution that scalp EEG cannot match. That precision is why the decoding accuracy reached 90%.
But it also defines the current ceiling of this technology:
- Only four participants, all with normal hearing
- Invasive setup — the electrodes required brain surgery
- No data yet on hearing loss — the neural signal may be weaker and less reliable in people with sensorineural hearing loss, a concern raised by MIT auditory neuroscientist Josh McDermott in response to the study
None of this diminishes what was demonstrated. The study is a proof-of-concept that the principle works in humans in real time — something that had not been shown before. The question is not whether the science is sound, but how long the path to a wearable device actually is.
What This Means for Cochlear Implant Users
Clinical Perspective
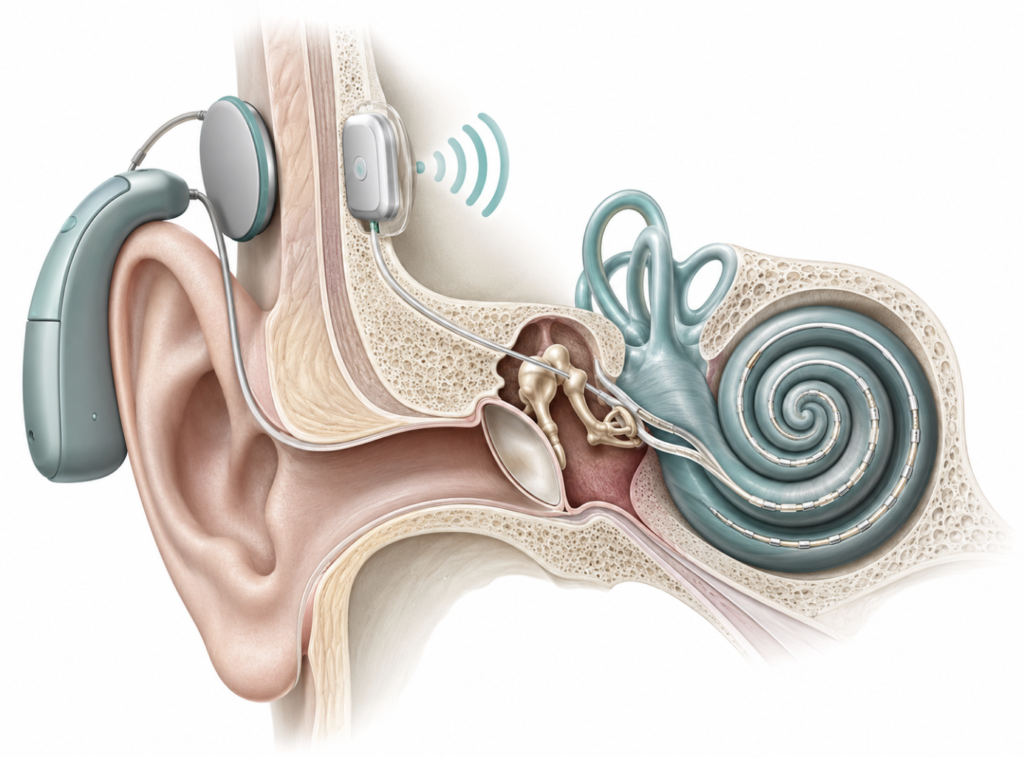
Cochlear implant users face a particularly demanding version of the cocktail party problem. Unlike hearing aid users, they receive electrical stimulation directly to the auditory nerve — bypassing the outer and middle ear entirely. Current speech processors are programmed for average listening conditions and have limited capacity to adapt to complex multi-talker environments.
The brain-controlled hearing concept is worth watching closely for this population. Because cochlear implants already operate at the brain-device interface, they may offer a more direct integration pathway for auditory attention decoding than conventional hearing aids. This remains speculative — no cochlear implant studies using this approach have been published to date — but it is a reasonable direction for future research to explore.
Where Current AI Hearing Aids Actually Stand
For those wondering whether to wait for this technology before choosing a hearing device: the short answer is no.
Current AI-enabled hearing aids — such as those using automatic environment classification and directional beamforming — offer real, measurable benefits for many users. They reduce background noise adaptively, improve signal-to-noise ratio in common environments, and have become considerably more sophisticated over the past five years. What they cannot do is what this study demonstrated: decode neural intent to select a specific voice.
The path from laboratory prototype to consumer wearable is long. It requires developing scalp EEG systems with sufficient signal fidelity, validating the decoding algorithm in populations with actual hearing loss, conducting randomized clinical trials, and navigating regulatory pathways.
Editorial note: Based on the current stage of the technology and historical precedent in neural interface development, a rough estimate of five to ten years to a viable non-invasive device seems reasonable — but this projection comes with significant uncertainty. The pace of technical progress in AI and neuroscience has accelerated considerably, compressing timelines that once seemed fixed. At the same time, the relationship between rapid technological development and institutional regulation is growing more complex, not less. In this environment, confident timelines are increasingly difficult to defend in either direction.

Key Takeaways
- A 2026 Nature Neuroscience study demonstrated the first real-time, brain-controlled hearing system that amplifies the voice a listener is focused on, achieving approximately 90% accuracy.
- The system uses intracranial EEG to decode auditory cortex activity in real time — a technique called Auditory Attention Decoding (AAD) — building on the 2012 finding that the auditory cortex selectively encodes attended speech.
- Current hearing aids excel at reducing background noise but cannot select between competing voices — this requires access to the listener’s neural attention signal, which no consumer device currently provides.
- The technology was tested in only four participants with normal hearing using invasive intracranial electrodes; clinical application for hearing loss patients is not imminent.
- Cochlear implant users may be among the most relevant future beneficiaries of this research direction, though no cochlear implant studies using this approach have been published.
FAQ
How does a brain-controlled hearing aid work? It reads electrical activity from the auditory cortex to detect which voice the listener is focusing on, then automatically amplifies that voice. In the 2026 Columbia study, the system used intracranial electrodes to capture neural signals with high resolution; future non-invasive versions would need to achieve similar decoding using scalp sensors.
Can current AI hearing aids focus on one voice in a noisy room? Not in the way this research describes. Today’s AI hearing aids use directional microphones and noise suppression algorithms that improve speech-to-noise ratios, but they cannot identify and isolate a specific speaker among several competing voices — that requires input from the listener’s nervous system.
When will brain-controlled hearing aids be available? No clinical timeline has been announced. Moving from an intracranial research prototype to a non-invasive consumer device requires signal fidelity improvements, clinical validation in hearing loss populations, and regulatory review. A rough estimate of five to ten years is defensible, but predicting timelines in this space is genuinely difficult — technical progress is accelerating while the regulatory environment surrounding AI-driven neural devices is growing more complex. Both forces are in play simultaneously.
Does this research apply to cochlear implant users? Not directly yet. Cochlear implants already interface electrically with the auditory nerve, which may offer a more direct path for integrating attention decoding in the future — but this has not been tested and remains an open research question.
Do I need to worry about brain surgery to use this technology eventually? The current prototype relied on existing surgical electrodes. The goal of ongoing research is to develop wearable, non-invasive systems that can decode attention from scalp recordings, which would not require surgery.
References
- Choudhari V, Nentwich M, Johnson S, Herrero JL, Bickel S, Mehta AD, Friedman D, Flinker A, Chang EF, Mesgarani N. Real-time brain-controlled selective hearing enhances speech perception in multi-talker environments. Nat Neurosci. 2026. [Note: DOI and final pagination to be confirmed against published article prior to posting.]
- Mesgarani N, Chang EF. Selective cortical representation of attended speaker in multi-talker speech perception. Nature. 2012;485(7397):233-6.
- World Health Organization. World Report on Hearing. Geneva: WHO; 2021.
Joonpyo Hong, MD is a board-certified otolaryngologist practicing in Korea. This article reflects his clinical interpretation of published research and does not constitute individual medical advice.
For more interesting contents:
https://curiousmd.com/ai-hearing-aids-2026-ent-review/
https://curiousmd.com/psap-vs-hearing-aid-clinical-evidence/
https://curiousmd.com/airpods-hearing-test-what-it-can-and-cannot-do/
https://curiousmd.com/objective-hearing-tests-abr-assr-oae/
Link out to:
https://www.nature.com/articles/s41593-026-02281-5
https://www.nature.com/articles/nature11020
https://www.who.int/publications/i/item/world-report-on-hearing
Pingback: Do AI Hearing Aids Work? An ENT's 2026 Take