
Eustachian tube function is easiest to appreciate the moment it fails. The plane starts its descent, your ears stop keeping up, sound goes muffled, and you swallow hard waiting for the small click that means the two sides finally equalized. That click is a tube barely two centimetres long doing its job — and when the same tube fails, it sits behind a surprising share of ear problems. This piece covers four things: what the eustachian tube actually does, why it matters more than most people realize, why it is genuinely hard to measure how well it is working, and whether good tube function is something you are born with or something you can train.
What the Eustachian Tube Actually Does
The eustachian tube links the middle ear to the back of the nose, and it has three jobs: it equalizes middle-ear pressure with the outside world, it drains secretions out of the middle ear, and it protects the middle ear from pathogens and reflux coming up from the nose and throat [Schilder, Eustachian tube dysfunction: consensus statement on definition, types, clinical presentation and diagnosis, 2015]. When any one of those three fails, the label doctors reach for is eustachian tube dysfunction (ETD).
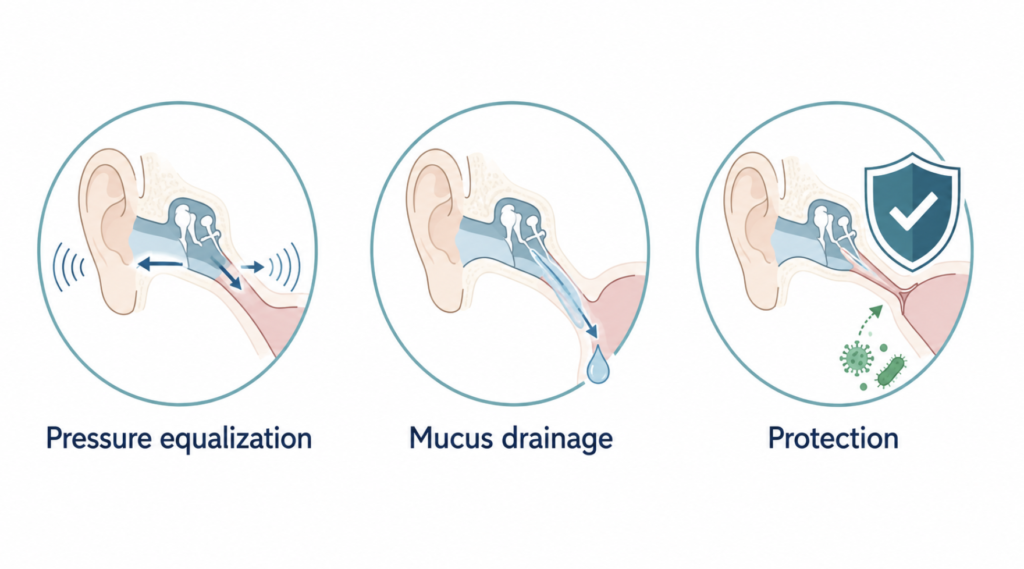
Pressure equalization is the function people actually feel. The middle ear is a sealed air pocket, and for the eardrum to vibrate efficiently the pressure inside has to match the pressure outside. On an aircraft, in an elevator, or underwater, the outside pressure changes fast, and the tube has to let air move in or out to keep the two sides balanced. That is what you are forcing when you swallow, yawn, or hold your nose and gently blow to “pop” your ears.
The other two jobs are quieter but just as important. A layer of tiny beating cilia sweeps mucus and debris down the tube toward the nose, keeping the middle ear clean. At the same time, because the tube spends most of its time closed, it acts as a one-way guard against nasal secretions and germs washing up into the ear.
Here is the part that makes the tube unusual: it is normally shut. Unlike your windpipe, it does not sit open. It flicks open only briefly during swallowing and yawning, when two small palate muscles — tensor veli palatini and levator veli palatini — pull it apart for a fraction of a second before it closes again. That design keeps the middle ear protected, but it also means the tube’s most important action is fast, intermittent, and hidden deep in the head — a detail that will matter a lot when we get to testing.
Why It Matters More Than People Think
A tube this small does not sound like a big deal until you see what happens when it stops working. Persistent eustachian tube dysfunction is one of the main upstream causes of middle-ear disease, and it is considered an important factor in how conditions like otitis media with effusion, eardrum retraction, chronic otitis media, and cholesteatoma get started [Smith, Tests of Eustachian tube function: a review, 2015]. When the tube cannot ventilate the middle ear, pressure drops, fluid collects, and the eardrum gets pulled inward — and from there a cascade of longer-term problems becomes possible.
Children feel this most. Fluid trapped behind the eardrum (“glue ear,” or otitis media with effusion) muffles hearing during exactly the years when kids are learning to speak, which is why chronic effusions are taken seriously rather than simply waited out. It is not just an ear problem; it can become a hearing-and-language problem.
So the stakes are higher than the anatomy suggests. A structure you cannot see, doing a job you barely notice, quietly determines whether the middle ear stays healthy — which is a good reason to want a reliable way to check whether it is working. That turns out to be the hard part.
Why Eustachian Tube Function Is So Hard to Evaluate
Here is the honest state of the field: there is no gold-standard test for eustachian tube function. A systematic review of the available tests concluded that while several exist, all have significant limitations, and no single one can be treated as the reference standard for diagnosing tube dysfunction [Smith, Tests of Eustachian tube function: a review, 2015]. For a condition this common, that is a striking gap.
Part of the problem is a distinction most people miss: a tube that is open is not the same as a tube that is working. You can have an open, patent tube that still fails to regulate pressure properly — and the opposite failure mode, a patulous tube that stays open too much, causes its own set of symptoms like hearing your own voice boom inside your head [Schilder, Eustachian tube dysfunction: consensus statement on definition, types, clinical presentation and diagnosis, 2015]. “Patency” and “function” are different questions, and most simple checks only get at the first.
The tests we do have each capture a sliver of the picture. Tympanometry measures pressure and eardrum mobility, but its sensitivity for tube dysfunction is often poor, and other maneuver-based tests vary widely from study to study [Tailor, Outcome measures for baro-challenge-induced Eustachian tube dysfunction: a systematic review, 2018]. On the symptom side, the ETDQ-7 questionnaire is the one patient-reported score that has been formally validated — but the very reason it was developed is that clinical assessment of ETD was limited without a standardized symptom measure, and a questionnaire, by nature, reflects how a patient feels rather than what the tube physically does [McCoul, Validating the clinical assessment of eustachian tube dysfunction: the Eustachian Tube Dysfunction Questionnaire (ETDQ-7), 2012].
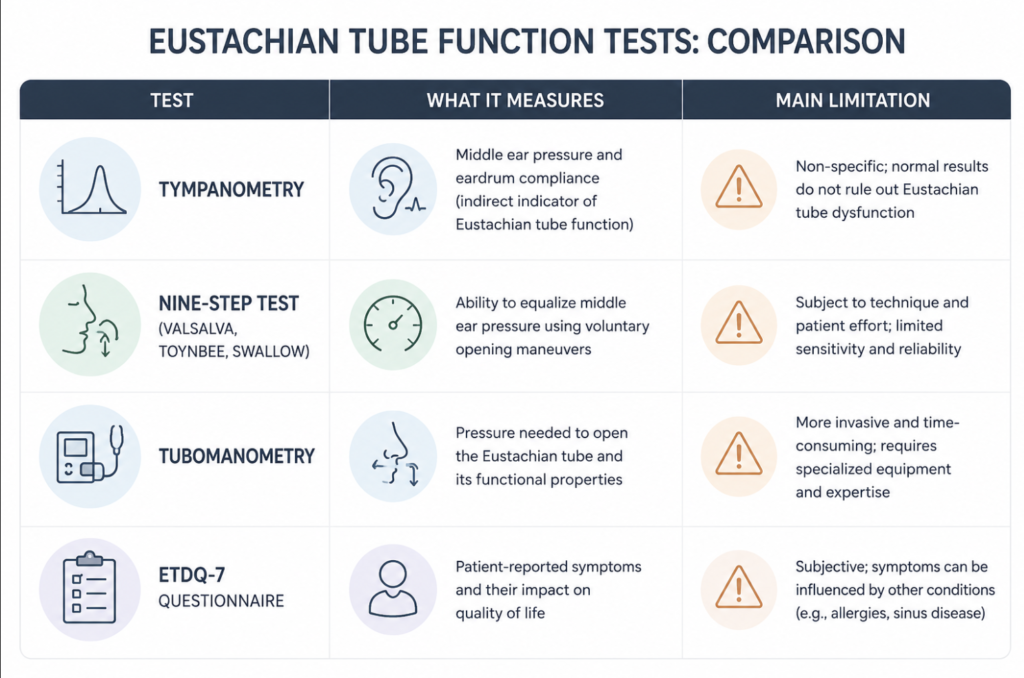
Because no single test is trustworthy alone, the most defensible approach is to combine them — pairing objective measurements with a patient-reported score improves accuracy over relying on either one [Smith, Tests of Eustachian tube function: a review, 2015]. In practice this is why a patient can walk in with textbook symptoms — fullness, muffled hearing, an ear that will not pop — and still have a normal tympanogram. The tube may genuinely be underperforming; our instruments just are not good enough to prove it cleanly. That mismatch is not the patient imagining things, and it is not the doctor missing something obvious. It is a real limit of the tools.
Born With It, or Can You Train It?
The starting point is anatomy, and a lot of it is set from birth. The tube’s length, diameter, and angle vary from person to person, and those baseline features influence how well it opens. In children the tube is shorter and lies more horizontally, which is part of why middle-ear infections cluster in early childhood and tend to ease as the skull grows and the tube lengthens and steepens. Certain congenital and craniofacial conditions — cleft palate is the classic example, along with Down syndrome — come with tube dysfunction so consistently that ear disease is almost expected. In other words, some of your eustachian tube function is simply inherited hardware.
But “can you train it?” is where the internet gets things wrong, so it is worth being precise. Most of what gets sold as strengthening the eustachian tube is not muscle-building at all. It is one of two things: learning to actively open a reluctant tube, or reducing the inflammation that is blocking it. Those are real and useful — they are just not the same as bulking up a bicep.
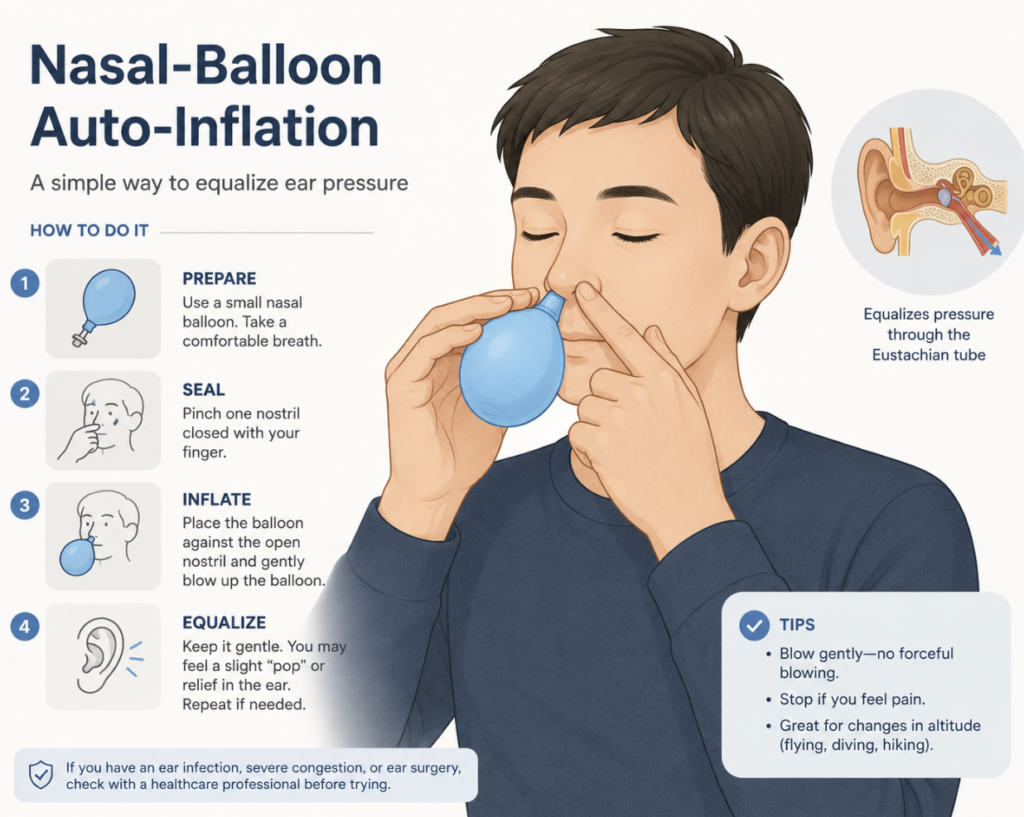
Take auto-inflation. Using a nasal balloon device (blowing up a small balloon through one nostril) does two things: it pushes air through the tube to clear trapped fluid, and it teaches you how much effort it takes to open your own tubes. In a randomized trial in school-aged children with glue ear, auto-inflation cleared middle-ear fluid more often than usual care alone, with a number needed to treat of about nine [Williamson, An open randomised study of autoinflation in 4- to 11-year-old school children with otitis media with effusion in primary care, 2015]. That is a genuine, evidence-backed benefit — but notice what it is doing: opening and draining, not remodeling the tube.
The gentler maneuvers work the same way. Swallowing, yawning, the Valsalva (pinch-and-blow), and the Toynbee (pinch-and-swallow) are all ways to actively trigger an opening. Breathing-retraining has some early support too: in a small preliminary trial, adding the Buteyko breathing technique to a nasal steroid roughly doubled the share of patients whose symptom scores normalized by twelve weeks, though the difference at six weeks was not statistically significant [Zeng, Buteyko breathing technique for obstructive Eustachian tube dysfunction: preliminary results from a randomized controlled trial, 2019]. Promising and worth knowing about — but “preliminary” and “adjunctive” are the right words, not “cure.”
And when the tube is structurally too narrow, the fix is mechanical, not muscular. Balloon dilation of the eustachian tube — physically widening it with a catheter — outperformed medical management in a randomized trial, with about half of treated patients reaching a normal tympanogram at six weeks versus roughly one in seven on medicine alone [Poe, Balloon dilation of the eustachian tube for dilatory dysfunction: a randomized controlled trial, 2018]. That is a procedure that changes the anatomy, which is the clearest sign that “training” was never really about strength.
The diver-and-pilot comparison makes the point cleanly. Experienced divers get remarkably good at equalizing under pressure, but what they are drilling is technique — the timing and coordination of opening the tube on demand — not the raw power of the tube. And even for people whose ears fail specifically under pressure changes, there is still no clean test to pin the problem down [Tailor, Outcome measures for baro-challenge-induced Eustachian tube dysfunction: a systematic review, 2018]. So the honest answer to “can you train it?” is: you can train your technique and you can calm the inflammation around it, and both can meaningfully improve symptoms — but you are working with an anatomical baseline you did not choose.
Clinical Perspective
The uncomfortable reality of this condition is that we are often treating something we cannot directly measure. Because no test is decisive on its own, a careful diagnosis leans on the whole picture — the symptoms, a battery of imperfect objective tests, and how things behave over time — rather than one number. That is not hand-waving; it is the appropriate response to genuinely limited tools.
For everyday symptoms, low-risk opening techniques are reasonable to try, and auto-inflation in particular has evidence behind it. The one caution worth repeating: a forceful Valsalva is not harmless, and blowing too hard against a pinched nose can injure the ear — gentle is the whole point. And if fullness or muffled hearing persists beyond a couple of weeks, comes with pain, or brings a clear change in hearing, that is the moment to have an ENT look rather than to keep experimenting at home.
Key Takeaways
- The eustachian tube does three things: it equalizes middle-ear pressure, drains secretions, and protects the middle ear from germs and reflux.
- Persistent eustachian tube dysfunction is an important upstream cause of middle-ear disease, from glue ear in children to eardrum retraction and cholesteatoma.
- There is no gold-standard test for eustachian tube function; the best current approach combines imperfect objective tests with a validated symptom score.
- A tube that is open is not necessarily a tube that is working — patency and function are different questions.
- “Training” the eustachian tube mostly means learning to open it and reducing obstruction, not strengthening it like a muscle; the anatomy you are born with sets the baseline.
FAQ
What does the eustachian tube do? It connects the middle ear to the back of the nose and performs three functions: equalizing middle-ear pressure with the outside air, draining fluid and mucus out of the middle ear, and protecting the middle ear from pathogens. It stays closed most of the time and opens briefly when you swallow or yawn. The pressure job is the one you notice — it is what lets your ears “pop” and adjust on a plane or underwater.
Why can’t doctors just measure eustachian tube function? Because no single test is reliable enough to serve as a gold standard. The tube’s key action is fast, intermittent, and hidden deep in the head, and the available tests each capture only part of what is happening. Tympanometry, maneuver-based tests, and symptom questionnaires all have real limitations, so clinicians combine several tests plus symptoms rather than trusting one result — which is why classic symptoms can coexist with a “normal” test.
Do eustachian tube exercises actually work? Some do, but not by strengthening the tube. Auto-inflation with a nasal balloon has trial evidence for clearing middle-ear fluid in children, and gentle maneuvers like swallowing, yawning, and a careful Valsalva can help open a blocked tube. A breathing technique (Buteyko) showed early promise as an add-on. These improve opening and drainage or reduce inflammation — real benefits, but different from building muscle. Avoid forceful blowing, which can harm the ear.
Is eustachian tube dysfunction hereditary? Partly. The tube’s shape, length, and angle are set from birth and influence how well it opens, and certain inherited conditions — cleft palate and Down syndrome, for example — come with a high rate of tube dysfunction. Children are also more prone because their tubes are shorter and more horizontal, which usually improves with growth. So there is a genuine inherited baseline, even though inflammation and technique are the parts you can actually influence.
When should I see an ENT? See a specialist if ear fullness or muffled hearing lasts more than a couple of weeks, comes with pain, or brings a noticeable change in your hearing. Brief blockage during a cold or a flight that resolves on its own is normal. Persistent symptoms are worth evaluating, because ongoing tube dysfunction can lead to fluid buildup and longer-term middle-ear problems that are better addressed early than left alone.
References
Schilder AGM, Bhutta MF, Butler CC, Holy C, Levine LH, Kvaerner KJ, et al. Eustachian tube dysfunction: consensus statement on definition, types, clinical presentation and diagnosis. Clin Otolaryngol. 2015;40(5):407-411.
McCoul ED, Anand VK, Christos PJ. Validating the clinical assessment of eustachian tube dysfunction: the Eustachian Tube Dysfunction Questionnaire (ETDQ-7). Laryngoscope. 2012;122(5):1137-1141.
Smith ME, Tysome JR. Tests of Eustachian tube function: a review. Clin Otolaryngol. 2015;40(4):300-311.
Tailor BV, Smith ME, Hutchinson PJA, Tysome JR. Outcome measures for baro-challenge-induced Eustachian tube dysfunction: a systematic review. Otol Neurotol. 2018;39(2):138-149.
Poe D, Anand V, Dean M, Roberts WH, Stolovitzky JP, Hoffmann K, et al. Balloon dilation of the eustachian tube for dilatory dysfunction: a randomized controlled trial. Laryngoscope. 2018;128(5):1200-1206.
Williamson I, Vennik J, Harnden A, Voysey M, Perera R, Breen M, et al. An open randomised study of autoinflation in 4- to 11-year-old school children with otitis media with effusion in primary care. Health Technol Assess. 2015;19(72):1-150.
Zeng H, Chen X, Xu Y, Zheng Y, Xiong H. Buteyko breathing technique for obstructive Eustachian tube dysfunction: preliminary results from a randomized controlled trial. Am J Otolaryngol. 2019;40(5):645-649.
Joonpyo Hong, MD is a board-certified otolaryngologist practicing in Korea. This article reflects his clinical interpretation of published research and does not constitute individual medical advice.
For more interesting contents:
https://curiousmd.com/ear-and-sinus-barotrauma-decongestant-guide/
https://curiousmd.com/ozempic-ear-side-effect-weight-loss-clogged-ears/
https://curiousmd.com/random-stabbing-ear-pain-few-seconds/
Link out to:
Eustachian Tube Dysfunction — StatPearls (NCBI Bookshelf, NIH):https://www.ncbi.nlm.nih.gov/books/NBK555908/
Physiology, Eustachian Tube Function — StatPearls (NCBI Bookshelf, NIH):https://www.ncbi.nlm.nih.gov/books/NBK532284/
Eustachian Tube Function — Medscape / eMedicine:https://emedicine.medscape.com/article/874348-overview