
This week’s headline is hard to resist: a painless mouth swab that spots oral cancer in about an hour, with over 95% accuracy. The number is real, and the technology behind it is genuinely useful. But oral cancer swab test accuracy is a slipperier idea than a single figure suggests — that 95% is not the 95% most readers will picture, and understanding the gap between the two is the difference between reading a press release and reading the study.
Here is what this article unpacks: what “accuracy” actually measures, the specific conditions that produced the 95% figure, and why — even in the best case — a positive swab is a reason to do a biopsy, not a reason to skip one.
The Study in Plain Terms
The test comes from a cross-university team led by Queen Mary University of London, published in Biomarker Research [Teh, INHBA-S100A16 dysregulation enables a non-invasive molecular stratification platform for rapid detection of oral squamous cell carcinoma, 2026]. It is called qMIDS-V3. A brush is swept across a suspicious lesion to collect surface cells, and a lab measures the activity of four genes — INHBA, S100A16, YAP1, and POLR2A — using RT-qPCR. An algorithm turns those readings into a “malignancy index.” A control sample from a healthy part of the same person’s mouth is analyzed alongside it, and the whole process takes roughly one hour.
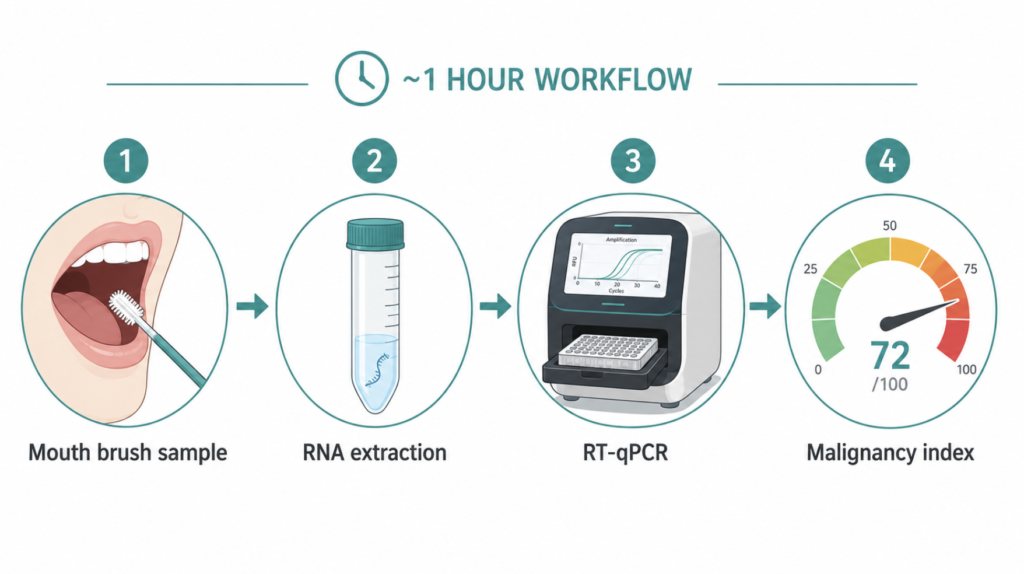
The headline claim is that this brush version performs about as well as an earlier tissue-based version that required a 1 mm microbiopsy. That matters most in places where a scalpel biopsy is genuinely difficult — the gum, for instance, where cutting can damage the underlying tooth and bone. A repeatable, painless swab in those locations would be a real practical gain.
The study tested 1,090 brush samples from 545 patients, each of whom gave paired swabs: one from the lesion and one from the opposite, healthy side of the mouth. So far, so promising. The question is what the accuracy number is measuring.
Oral Cancer Swab Test Accuracy: Decoding the Number
Sensitivity and Specificity Are Not the Same Thing
“Accuracy” is a single word hiding two different abilities, and a test can be strong in one and weak in the other.
Sensitivity is a test’s ability to correctly flag people who actually have the disease — in other words, how rarely it misses. Specificity is its ability to correctly clear people who do not have the disease — how rarely it raises a false alarm. A test that calls everyone positive has perfect sensitivity and useless specificity. A good test needs both to be high.
On this front, qMIDS-V3 looks strong: sensitivity 95.7% and specificity 95.1% in its best comparison. Those are respectable numbers. The catch is the phrase “best comparison.”
Which 95%? The Comparison That’s Easy to Miss
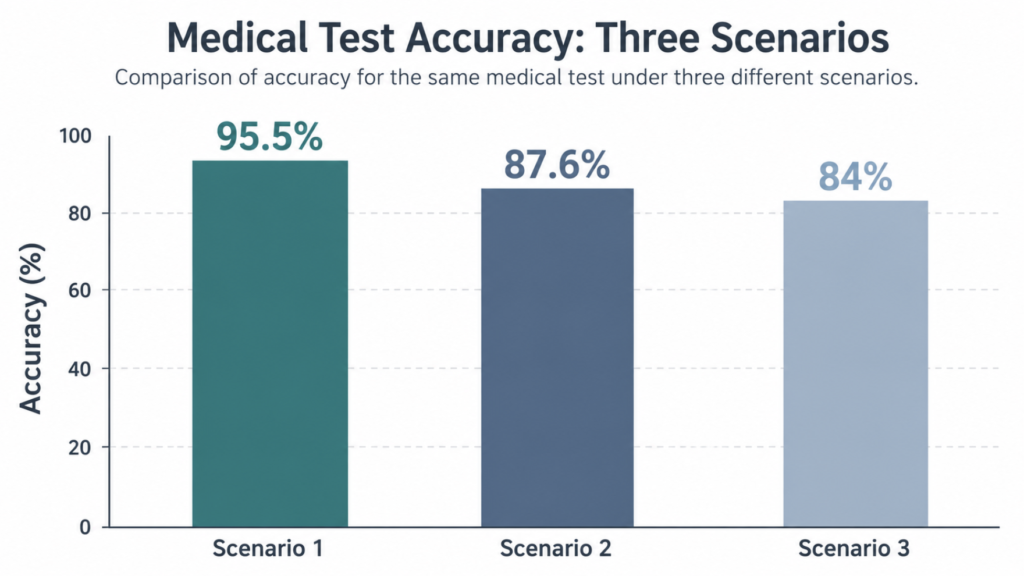
The researchers actually ran three different comparisons, and the 95.5% is the best of the three [Teh, 2026]. It came from separating cancer from low-risk lesions only — leukoplakia and lichen planus. That is, in fairness, the comparison most relevant to triage: a patient with a visible lesion usually needs to know “is this cancer or a low-risk condition?” So the flagship number is defensible for its intended job.
The picture gets more mixed with the other two comparisons. Against the patient’s own normal-looking mucosa, accuracy fell to 84% (AUC 0.913). Against a pooled group of normal mucosa plus low-risk lesions, it landed at 87.6%, with specificity dropping to 78.4% . None of these are bad numbers, but “95% accurate” is the ceiling of the range, not a single figure that describes the test everywhere.
| Comparison | AUC | Sensitivity | Specificity | Accuracy |
|---|---|---|---|---|
| Cancer vs. low-risk lesions (OPMD) | 0.975 | 95.7% | 95.1% | 95.5% |
| Cancer vs. normal mucosa | 0.913 | 84% | 84% | 84% |
| Cancer vs. normal + low-risk combined | 0.937 | 87.7% | 78.4% | 87.6% |
Why the Headline Number Will Look Better Than Real Life
This Was a Case-Control Study, Not a Screening Study
The design matters as much as the result. This was a case-control study: the researchers started with patients already sorted into known groups — confirmed cancer versus confirmed benign lesions — and checked how well the test told the pre-defined groups apart.
That structure tends to make a test look better than it will in practice, because the hard, ambiguous, in-between cases that fill a real clinic are underrepresented. It is a validation of the biological signal, not a measurement of how the test performs when you point it at the general public.
Prevalence Quietly Changes Everything
Here is the part most coverage skips. Of the 545 patients, 443 already had cancer — leukoplakia (63) and lichen planus (39) made up the rest. That means roughly 81% of the study population had cancer before the swab was ever taken.
In any realistic screening setting, the share of people with actual cancer is far lower. When disease is rare, even a highly specific test produces more false positives relative to true ones, so the chance that a positive result means real cancer — the positive predictive value — falls well below the accuracy figure. The study itself reports a high positive predictive value (97.8%), but that number was calculated inside a sample where roughly four in five people already had cancer; drop the prevalence to what a real clinic sees and the figure would fall. Put simply: “95% accurate” does not mean “a positive result is 95% likely to be cancer.” Those are different statements, and the second one depends heavily on who is being tested — a point the authors flag directly, noting their group sizes do not reflect true disease prevalence [Teh, 2026].
One More Caveat: Where the Patients Came From
The validation cohort was drawn from a single regional population in Uttar Pradesh, India. That matters because oral cancer patterns are not uniform worldwide — smokeless tobacco and areca nut use make oral cancer far more common in parts of South Asia than in, say, Korea or Western Europe. The underlying gene signature was validated earlier across UK, China, and Indian cohorts, which is reassuring, but the authors themselves list single-region sampling as a limitation on how far this specific result should be generalized.
Screening, Triage, or Diagnosis — Which Is This?
These three words get used interchangeably in headlines, and the distinction is the whole ballgame.
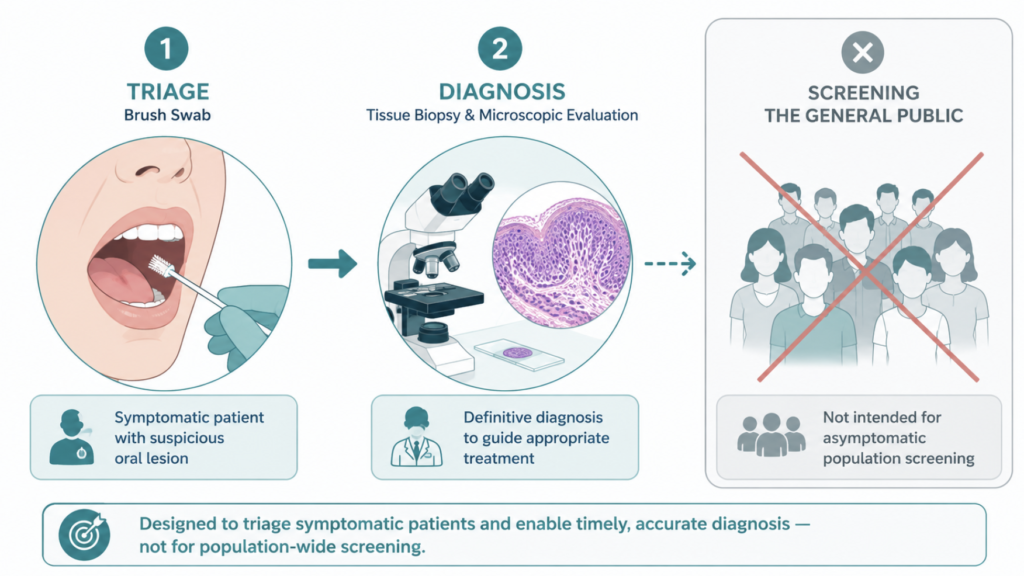
Screening means checking people with no symptoms to catch disease early. Triage means taking people who already have a suspicious lesion and sorting who needs urgent invasive workup. Diagnosis means confirming what a lesion actually is. This test is a triage tool — the authors describe it as a rapid case-finding or triage test. It is not a population screen, and it does not replace the diagnostic step.
That framing lines up with the broader evidence. A Cochrane review of adjunctive oral cancer tests concluded that none can currently replace scalpel biopsy with histology, with oral cytology showing the most promise among them (sensitivity 0.90, specificity 0.94) [Walsh, Diagnostic tests for oral cancer and potentially malignant disorders in patients presenting with clinically evident lesions, 2021]. The American Dental Association’s guideline reached the same conclusion: no adjunct has sufficient accuracy to be used routinely as a triage tool, and for a suspicious lesion, immediate biopsy or specialist referral remains the single most important step [Lingen, Evidence-based clinical practice guideline for the evaluation of potentially malignant disorders in the oral cavity, 2017].
That has one practical consequence worth stating plainly: because every adjunctive test carries a real false-negative rate, a lesion that looks or behaves suspiciously warrants a tissue biopsy regardless of a reassuring swab result. A negative index lowers the probability of cancer; it does not override what the clinician can see. And at the population level, a separate Cochrane review found a lack of high-certainty evidence to support routine oral cancer screening in apparently healthy adults, which is exactly why a tool like this belongs in the workup of people who already have a lesion, not in mass screening [Walsh, Clinical assessment for the detection of oral cavity cancer and potentially malignant disorders in apparently healthy adults, 2021].
Where This Test Genuinely Helps
None of this makes the swab a gimmick. Its real value may lie less in the dramatic “detects cancer” framing and more in monitoring. Because it is painless and repeatable, it is well suited to following patients with persistent potentially malignant disorders over time, watching for the moment a stable lesion starts to change.
There is also a system-level problem it could ease. In the UK, a 10-year audit cited in the study found urgent (two-week-wait) referrals for suspected oral cancer rose roughly 450% while the cancer detection rate among those referred fell by about 50% — a lot of anxious patients and biopsies for lesions that turn out benign . A reliable triage step that spares low-risk patients an unnecessary scalpel biopsy is a meaningful contribution, even if it never touches the general public.
Clinical Perspective
From a head and neck standpoint, the appeal is real: painless, fast, repeatable sampling — especially in sites where biopsy is awkward or damaging — is a step forward. The signal from these four genes appears robust, and that is worth taking seriously.
But the message for any patient is simple. A positive swab is not a verdict; it is a ticket to the next step, which is a biopsy. And a negative swab does not cancel clinical judgment — if a lesion looks or behaves suspiciously, it still warrants follow-up or biopsy regardless of the index. The right question to ask of any “X% accurate” test is never just the number. It is: accurate at what task, in which patients, compared against what?
Key Takeaways
- The “95.5% accuracy” applies only when the test separated cancer from low-risk lesions; against normal mucosa, accuracy fell to 84%.
- Sensitivity (catching real disease) and specificity (avoiding false alarms) are distinct — a single “accuracy” figure hides both.
- This was a case-control study where about 81% of participants already had cancer, which inflates apparent accuracy relative to real-world screening.
- The test is a triage tool for people who already have a suspicious lesion, not a screening test for the general public.
- A positive result is not a diagnosis; surgical biopsy with histology remains the standard for confirming oral cancer.
FAQ
Does this swab test replace a biopsy for oral cancer? No. A positive swab still needs to be confirmed by a surgical biopsy with histology, which remains the diagnostic standard. The swab is designed to sort which patients most need that biopsy, not to make the final call itself.
Does a positive swab mean I have cancer? Not necessarily. In real-world settings where oral cancer is uncommon, a positive result is less likely to reflect true cancer than the headline accuracy suggests, because the chance a positive is correct depends on how common the disease is in the group being tested.
Is 95% accuracy good for a cancer test? It depends on context. The figure only means something once you know which two groups were compared and how common the disease was in the study — the same test scored 95.5% against low-risk lesions but 84% against normal tissue.
Who is this test actually for? It is aimed at people who already have a suspicious oral lesion needing evaluation, and at patients with potentially malignant disorders who need long-term monitoring. It is not intended as a general screening test for people without symptoms.
What’s the difference between sensitivity and specificity? Sensitivity is how well a test catches people who truly have the disease, so higher sensitivity means fewer missed cases. Specificity is how well it clears people who do not have the disease, so higher specificity means fewer false alarms. A strong test needs both.
References
Teh MT, Patil R, Tekade SA, Mishra D, Chaurasia A, Waseem A. INHBA-S100A16 dysregulation enables a non-invasive molecular stratification platform for rapid detection of oral squamous cell carcinoma: results from a large diagnostic case-control study. Biomark Res. 2026;14(1).
Walsh T, Macey R, Kerr AR, Lingen MW, Ogden GR, Warnakulasuriya S. Diagnostic tests for oral cancer and potentially malignant disorders in patients presenting with clinically evident lesions. Cochrane Database Syst Rev. 2021;7(7):CD010276.
Walsh T, Warnakulasuriya S, Lingen MW, Kerr AR, Ogden GR, Glenny AM, Macey R. Clinical assessment for the detection of oral cavity cancer and potentially malignant disorders in apparently healthy adults. Cochrane Database Syst Rev. 2021;12(12):CD010173.
Lingen MW, Abt E, Agrawal N, et al. Evidence-based clinical practice guideline for the evaluation of potentially malignant disorders in the oral cavity: a report of the American Dental Association. J Am Dent Assoc. 2017;148(10):712-727.e10.
Joonpyo Hong, MD is a board-certified otolaryngologist practicing in Korea. This article reflects his clinical interpretation of published research and does not constitute individual medical advice.
For more interesting contents:
https://curiousmd.com/hpv-vaccine-and-throat-cancer/
https://curiousmd.com/ai-de-escalation-in-hpv-throat-cancer/
https://curiousmd.com/leukoplakia-white-patches-cancer-risk/
https://curiousmd.com/aphthous-ulcer-treatment-ent-guide/
Link out to:
- Queen Mary University of London — “New brush test detects oral cancer in one hour” — the research team’s own plain-language summary of the qMIDS-V3 study.
- The qMIDS-V3 study (Biomarker Research, 2026) — the full peer-reviewed paper, open access.
- Cochrane review: diagnostic tests for oral cancer in patients with clinically evident lesions — why no adjunctive test yet replaces biopsy.
- Cochrane review: clinical assessment to detect oral cancer in apparently healthy adults — the evidence on population-level oral cancer screening.