
A patient sits down to lunch, and within minutes the soft tissue under the jaw swells and starts to ache. By evening it settles — then the same thing happens at dinner. That mealtime rhythm of swelling and pain is the classic signature of a salivary gland stone. Most people are told to drink more water and wait it out. Sometimes that works. Often it does not, and knowing which situation you are in is what this article is about.
What Are Salivary Gland Stones?
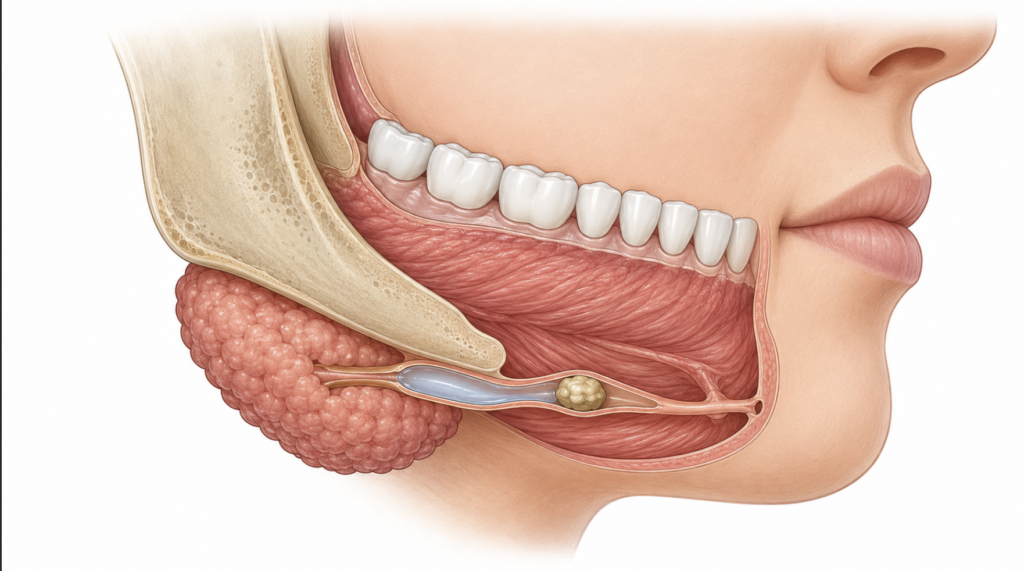
Salivary gland stones, known medically as sialolithiasis, are calcified deposits that form inside a salivary gland or the duct that carries saliva into the mouth. They are not true “rocks” — they are built up from minerals like calcium combined with organic material that accumulates over time. When a stone grows large enough to block the duct, saliva backs up behind it, and the gland swells.
The submandibular glands, which sit under the jaw and drain through a long, upward-running duct, account for the large majority of cases. In a retrospective cohort of 153 patients, 82% of stones were submandibular and 18% were parotid [Huoh, Etiologic factors in sialolithiasis, 2011]. The anatomy explains the bias: the submandibular duct is long, runs against gravity, and carries thicker saliva — all of which favor stone formation.
Why They Form
The exact cause remains uncertain, but the common thread is reduced or stagnant salivary flow. Dehydration thickens saliva, and anything that slows flow gives minerals time to settle. The same cohort found that diuretic use was more than twice as common among stone patients as in the general population, and smoking histories were also frequent [Huoh, Etiologic factors in sialolithiasis, 2011]. Reduced food intake, certain medications that dry the mouth, and chronic low-grade duct inflammation are all plausible contributors [Wilson, Salivary gland disorders, 2014].
Symptoms: The Mealtime Swelling Pattern
The single most useful clue is timing. Saliva production surges the moment you smell, taste, or begin to eat. If a stone is blocking the duct, that surge has nowhere to go, pressure builds, and the gland swells and hurts — usually within minutes of starting a meal, easing over the next hour or two.
A typical example: someone notices a firm, tender lump under one side of the jaw that appears at every meal and shrinks between meals. Massaging the area may release a rush of saliva with an unpleasant taste. If bacteria travel back up the obstructed duct, the gland can become infected, producing constant pain, redness, fever, and sometimes pus — a shift from a mechanical problem to one that needs prompt treatment [Wilson, Salivary gland disorders, 2014].
Can a Salivary Stone Pass on Its Own?
Small stones can pass on their own, but many do not — and that is the part patients are rarely told clearly. A stone only a millimeter or two across, sitting near the duct opening, has a reasonable chance of working its way out with hydration and massage. Larger stones, or stones deeper in the duct or within the gland itself, usually stay put. Their surface is often rough and irregular rather than smooth, so they tend to catch on the duct lining instead of sliding out.
This is why “just drink water” is incomplete advice. Conservative measures are the right first step, but if swelling keeps recurring over weeks despite good hydration, the stone is unlikely to clear by itself and waiting mainly risks repeated infections.
Treatment Options: From Massage to Sialendoscopy
Treatment is matched to the size and, above all, the location of the stone. The goal of modern management is to relieve the obstruction while keeping the gland whenever possible.
Conservative care
For small stones and early symptoms, the first line is non-surgical: staying well hydrated, applying warm compresses, gently massaging the gland toward the duct opening, and using sialagogues such as sour or tart foods that stimulate saliva flow and may help flush the stone out [Wilson, Salivary gland disorders, 2014]. If infection is present, antibiotics are added.
Gland-preserving removal
When stones do not pass, the field has moved decisively toward minimally invasive, gland-sparing techniques. Stones near the duct opening can often be removed through a small incision inside the mouth under local anesthesia. Deeper stones are increasingly reachable by sialendoscopy — a thin endoscope passed directly into the salivary duct that lets the surgeon find and retrieve the stone without removing the gland.
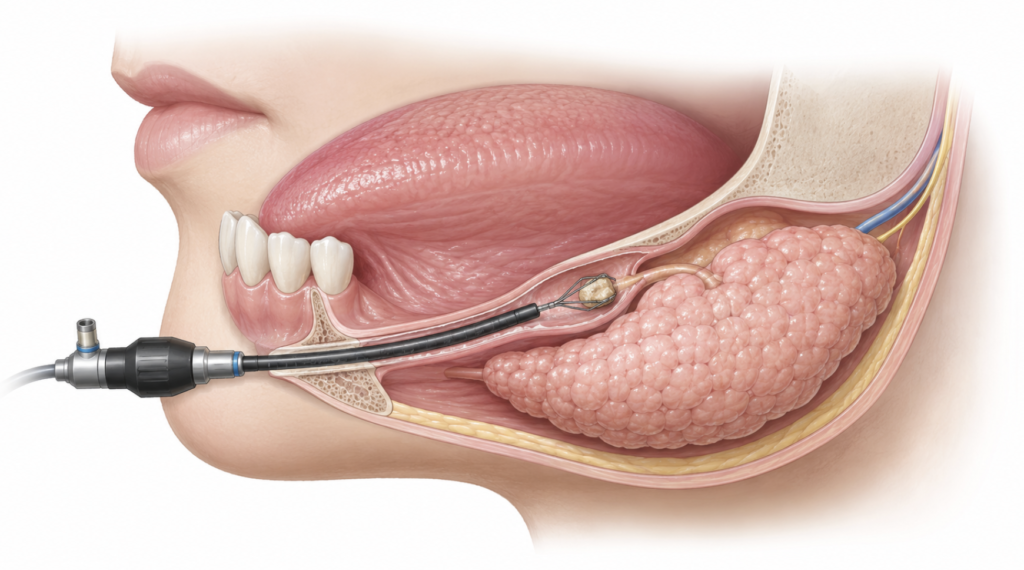
The case for preserving the gland is not just cosmetic. Historically, patients whose conservative treatment failed were offered removal of the whole gland; sialendoscopy has since emerged as an effective, gland-preserving alternative. A systematic review and meta-analysis of 29 adult studies found a pooled success rate of 86% for sialendoscopy alone and 93% when combined with a surgical approach, with low rates of gland removal [Strychowsky, Sialendoscopy for the management of obstructive salivary gland disease: a systematic review and meta-analysis, 2012]. Importantly, a preserved gland recovers function: in a prospective study using sialometry and scintigraphy, glands that had been obstructed regained secretory function after sialendoscopic clearance, becoming statistically comparable to the healthy opposite side [Su, Salivary gland functional recovery after sialendoscopy, 2009].
When gland removal is needed
Surgical removal of the gland is reserved for stones that cannot be reached or cleared by less invasive means, or for glands damaged by repeated infection. This is the last option, not the default.
| Stone location | Typical approach |
|---|---|
| Small, near the duct opening | Conservative care; may pass on its own |
| Distal duct (palpable in the mouth) | Transoral incision, often local anesthesia |
| Proximal duct or inside the gland | Sialendoscopy or combined endoscopic-open technique |
| Stone unreachable / gland damaged by infection | Gland removal |
Clinical Perspective
The decision that matters most in practice is not “stone or no stone” but “wait or intervene.” A single episode that resolves with hydration is reasonable to watch. A pattern of swelling at every meal that persists for weeks, or any episode with fever and spreading redness, is a signal to image the gland and plan removal rather than keep waiting. The aim is always to clear the blockage early enough that the gland is still worth saving — because a gland that keeps getting infected eventually stops being salvageable.
Key Takeaways
- About 8 in 10 salivary gland stones form in the submandibular gland under the jaw, largely because of its long, upward-draining duct [Huoh, Etiologic factors in sialolithiasis, 2011].
- Swelling and pain that appear within minutes of eating and ease afterward are the hallmark of an obstructing stone.
- While small stones near the duct opening have the best chance to pass on their own, larger or deeper stones most often require medical intervention.
- Sialendoscopy can clear many stones without removing the gland, and obstructed glands can regain function once cleared [Su, Salivary gland functional recovery after sialendoscopy, 2009].
- Whole-gland removal is a last resort, not the standard treatment.
FAQ
Can salivary stones pass on their own?
Small stones can, but most larger ones do not. A stone of one or two millimeters near the duct opening may flush out with hydration and gland massage. Bigger stones, or those deeper in the duct, tend to have rough surfaces that snag on the duct lining and stay in place. If swelling keeps returning for weeks despite good hydration, the stone is unlikely to clear on its own.
How are salivary gland stones removed?
Removal depends on location. Stones near the duct opening can often be taken out through a small incision inside the mouth. Deeper stones are increasingly removed by sialendoscopy, a thin scope passed into the duct, which avoids removing the gland. Whole-gland removal is reserved for stones that cannot be reached or glands damaged by repeated infection, and is uncommon where endoscopic approaches are available [Strychowsky, Sialendoscopy for the management of obstructive salivary gland disease: a systematic review and meta-analysis, 2012].
Are salivary stones dangerous if left untreated?
They are usually not life-threatening, but an obstructed gland can become repeatedly infected. Bacteria traveling up the blocked duct can cause painful swelling, fever, and pus, and in severe cases the infection can extend beyond the gland into surrounding neck tissues. Repeated infection can also permanently damage the gland, so persistent or infected stones should be treated rather than ignored [Wilson, Salivary gland disorders, 2014].
How can I lower my risk of forming them again?
Staying well hydrated is the most consistent measure, since thick, stagnant saliva favors stone formation. Reviewing medications that dry the mouth with your physician, and maintaining good oral hygiene to limit duct inflammation, are reasonable steps. These measures reduce risk but do not guarantee prevention, as the underlying cause is not fully understood [Huoh, Etiologic factors in sialolithiasis, 2011].
References
- Huoh KC, Eisele DW. Etiologic factors in sialolithiasis. Otolaryngol Head Neck Surg. 2011;145(6):935-939.
- Wilson KF, Meier JD, Ward PD. Salivary gland disorders. Am Fam Physician. 2014;89(11):882-888.
- Su YX, Xu JH, Liao GQ, Zheng GS, Cheng MH, Han L, Shan H. Salivary gland functional recovery after sialendoscopy. Laryngoscope. 2009;119(4):646-652.
- Strychowsky JE, Sommer DD, Gupta MK, Cohen N, Nahlieli O. Sialendoscopy for the management of obstructive salivary gland disease: a systematic review and meta-analysis. Arch Otolaryngol Head Neck Surg. 2012;138(6):541-547.
Joonpyo Hong, MD is a board-certified otolaryngologist practicing in Korea. This article reflects his clinical interpretation of published research and does not constitute individual medical advice.