
The connection between the shingles vaccine and hearing loss is one most patients never hear about. Even with treatment, about one in three patients with herpes zoster oticus does not fully recover facial movement, and some never recover their hearing [Monsanto, Treatment and Prognosis of Facial Palsy on Ramsay Hunt Syndrome, 2016]. Most people picture shingles as a painful band of blisters on the torso; as an otolaryngologist, I see the version that attacks the face and ear, where a vaccine designed “for a rash” quietly earns its keep.
This article separates what we know with certainty from what is still a promising hypothesis. The distinction matters, because recent dementia headlines have led some patients to ask for a “dementia shot.” That is not what this vaccine is: its established purpose is preventing shingles, and any cognitive protection is, for now, an unproven potential bonus rather than a reason to vaccinate.
A Quick Map of the Evidence
The science behind the shingles vaccine sits at very different levels of certainty. Reading the table below first will make the rest of the article easier to weigh.
| Claim | Evidence level | Verdict |
|---|---|---|
| Vaccine prevents shingles and post-herpetic neuralgia | Randomized controlled trials (highest) | Established |
| Vaccine lowers risk of ear and facial-nerve shingles (Ramsay Hunt) | Biological reasoning + RCT data on zoster overall | Very likely, not directly trialed for this endpoint |
| Vaccine lowers dementia risk | Natural experiment / observational (lower) | Association only — causality unproven |
| Vaccine lowers stroke risk | Observational signals | Hypothesis — awaiting trials |
What Shingles Really Is, and Why ENTs Care
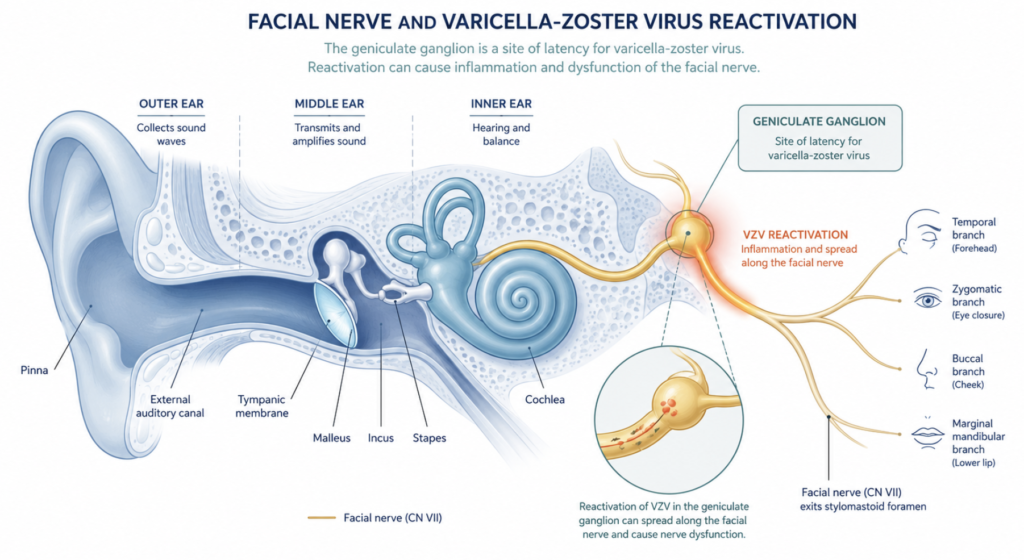
Shingles is the reactivation of varicella-zoster virus (VZV), the chickenpox virus, which hides in nerve ganglia for decades. When it wakes up in the geniculate ganglion of the facial nerve, the result is herpes zoster oticus, better known as Ramsay Hunt syndrome.
Ramsay Hunt is not a rare curiosity to an ear specialist. It is an important cause of acute peripheral facial paralysis. Because the virus sits next to the vestibulocochlear nerve, patients often arrive with hearing loss, tinnitus, and vertigo alongside the facial weakness and ear rash.
Clinical Perspective: A diagnostic trap is the roughly one in three cases where the rash is faint or absent, a presentation called zoster sine herpete. Sudden one-sided hearing loss or facial droop can appear with no obvious blisters, so VZV belongs on the differential for unexplained sudden sensorineural hearing loss, and prompt treatment is a priority.
Timing matters here. Observational studies and expert consensus suggest that starting antiviral and steroid treatment as early as possible, ideally within 72 hours of symptom onset, improves the odds of recovery, and Ramsay Hunt generally carries a worse prognosis than Bell’s palsy [Coulson, Prognostic Factors in Herpes Zoster Oticus (Ramsay Hunt Syndrome), 2011].
The Solid Part: This Vaccine Prevents Shingles
This is the claim that rests on the strongest possible evidence: randomized controlled trials (RCTs), the gold standard in which thousands of people are randomly assigned to vaccine or placebo.
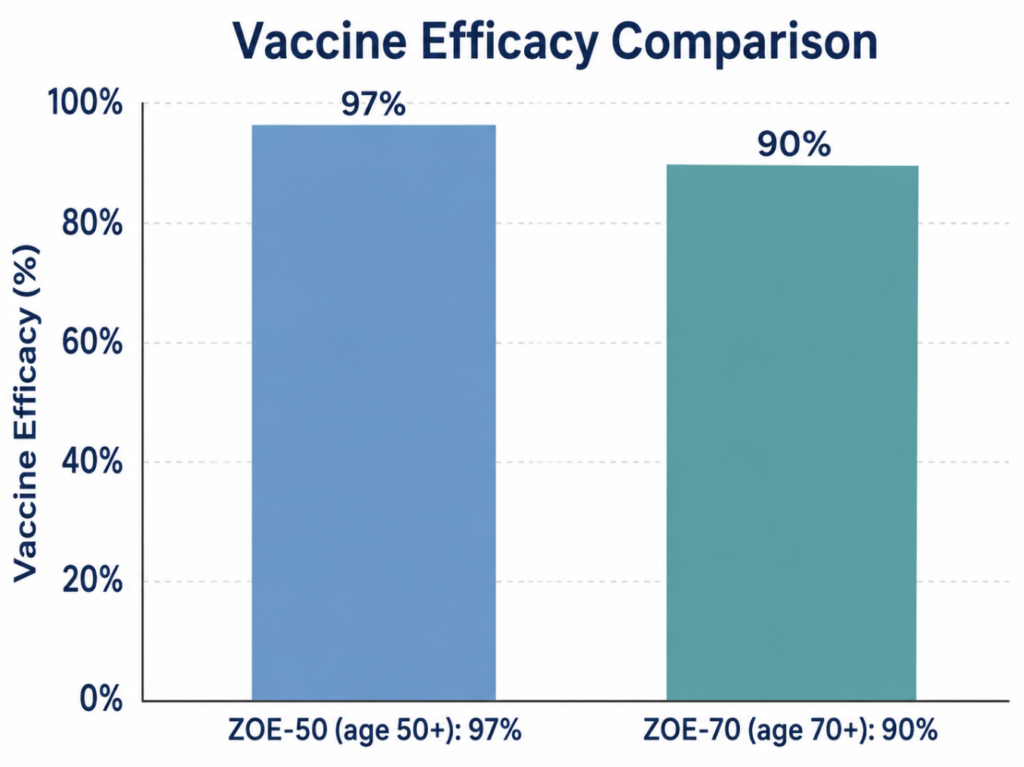
In the ZOE-50 trial, the recombinant zoster vaccine reduced shingles by 97.2% in adults aged 50 and older [Lal, Efficacy of an Adjuvanted Herpes Zoster Subunit Vaccine in Older Adults, 2015]. The companion ZOE-70 trial showed 89.8% efficacy in adults aged 70 and older, with an 88.8% reduction in post-herpetic neuralgia [Cunningham, Efficacy of the Herpes Zoster Subunit Vaccine in Adults 70 Years of Age or Older, 2016].
Two points follow logically. First, because Ramsay Hunt syndrome is a cranial-nerve form of shingles, a vaccine this effective at preventing shingles is very likely to reduce its incidence too. Second, that downstream protection has not been tested directly in a dedicated trial, so the honest phrasing is “very likely to reduce” rather than “proven to prevent.” It is a reasonable inference from strong data, not a separate proven fact.
The Promising Part: Dementia (Read This Carefully)
Here is where caution is essential. In 2025, a widely reported study used a quirk of Welsh vaccine policy, eligibility set by exact date of birth, to compare people who were just barely eligible against those just barely too old. In this natural experiment, the group eligible for the vaccine showed a roughly 20% lower rate of new dementia diagnoses over seven years [Eyting, A Natural Experiment on the Effect of Herpes Zoster Vaccination on Dementia, 2025]. A follow-up analysis observed an association with fewer mild cognitive impairment diagnoses and fewer dementia deaths among people who already had the disease [Xie, The Effect of Shingles Vaccination at Different Stages of the Dementia Disease Course, 2025].
These are clever, carefully designed studies, but they are natural experiments, not randomized trials. They strengthen an association; they do not prove the vaccine causes lower dementia rates. The researchers themselves are explicit that a randomized controlled trial is still needed, and they are working to launch one.
Clinical Perspective: The dementia data is best framed as a possible bonus, not a reason to get vaccinated. The established rationale rests on randomized-trial evidence: avoiding shingles and its complications, including the ear and facial-nerve disease seen in ENT practice. If the dementia benefit is confirmed one day, it would be welcome news layered on top of an already worthwhile vaccine.
The Speculative Part: Stroke and the Heart
VZV does not only inflame nerves; it can inflame blood vessels. In the year following a shingles episode, stroke risk rises measurably [Kang, Increased Risk of Stroke After a Herpes Zoster Attack: A Population-Based Follow-Up Study, 2009].
It is therefore plausible that preventing shingles also prevents some of these vascular events, and several observational analyses have reported lower rates of stroke and heart attack among vaccinated adults. But this evidence is observational, vulnerable to the bias that health-conscious people are both more likely to get vaccinated and less likely to have strokes. Until a randomized trial weighs in, these cardiovascular benefits remain hypothesis-generating rather than established.
Which Vaccine, and How Many Doses?
Globally, the field has shifted from the older live vaccine to the recombinant (non-live) vaccine, given as two doses two to six months apart. The recombinant vaccine works in people with weakened immune systems who cannot safely receive live vaccines, and its efficacy holds up better with age. In 2025 the World Health Organization reviewed the use of the recombinant zoster vaccine, suggesting that countries where shingles is a meaningful public health burden consider a two-dose schedule alongside their own cost-effectiveness analysis.
How Different Countries Recommend It
Who pays, at what age, and with which vaccine varies widely. The table below compares the picture as of early 2026. Policies change often, so treat this as orientation, not a substitute for checking your own national or local guidance.
| Country / region | Eligible age | Public funding | Vaccine and doses |
|---|---|---|---|
| United States | 50+ (immunocompromised 19+) | Not universally free; covered by Medicare and most private insurance | Recombinant, 2 doses |
| United Kingdom | 65, plus 70–79 catch-up; immunocompromised 18+ | Free through the NHS | Recombinant, 2 doses |
| Australia | 65+; Indigenous 50+; immunocompromised 18+ | Free for eligible groups | Recombinant, 2 doses |
| Japan | 65+; immunocompromised 60–64 | Partial subsidy (patient pays a share) | Live (1 dose) or recombinant (2 doses), patient’s choice |
| South Korea | Mostly 65+; criteria vary by district | No national program; local-government support only, varying by region | Varies by district — some fully free, some partly subsidized; vaccine type differs locally |
| Middle East (e.g. Saudi Arabia, UAE) | 50+ recommended | Recommended but generally not funded | Recombinant, self-paid |
| Much of Africa | No national programs | Not funded; access very limited | — |
A few patterns are worth flagging for readers deciding what to do.
First, the live-versus-recombinant split is narrowing fast. Where a national program still offers a live vaccine for budget reasons, that is a cost decision, not a statement that the two vaccines are equal: the recombinant vaccine has markedly higher and more durable efficacy in the trials cited above. For most adults with a choice who can manage the out-of-pocket cost, the recombinant vaccine is the stronger option.
Second, “recommended” and “funded” are different things. In several wealthy countries, including across the Middle East and South Korea, the vaccine is advised but not paid for by the state, which is a major reason uptake stays low even where awareness is reasonable.
Clinical Perspective: Shingles vaccination is commonly assumed to be part of national immunization program, as with influenza or pneumococcal vaccines. It generally is not — coverage depends on local government, age, and income criteria. Patients prioritizing protection against ear and facial-nerve complications may wish to ask specifically about the recombinant vaccine and confirm local subsidy eligibility before assuming it is free.
Third, if you are immunocompromised, the age rules usually do not apply. Most programs that fund the vaccine extend eligibility down to age 18 or 19 for people on immunosuppressive treatment or with conditions that raise shingles risk, and the recombinant vaccine is specifically the one indicated for this group.
Key Takeaways
- The recombinant zoster vaccine has randomized-trial evidence for preventing shingles and post-herpetic neuralgia (90–97% efficacy) — this is the established, gold-standard benefit.
- Because Ramsay Hunt syndrome is a cranial-nerve form of shingles, vaccination is very likely to reduce its incidence, although that endpoint has not been tested directly in a dedicated trial.
- VZV can cause sudden hearing loss and facial paralysis even without a visible rash (zoster sine herpete), making early recognition critical.
- Observational and natural-experiment studies suggest possible associations with lower dementia risk, but causality remains unproven.
- Reported cardiovascular benefits remain hypothesis-generating rather than established.
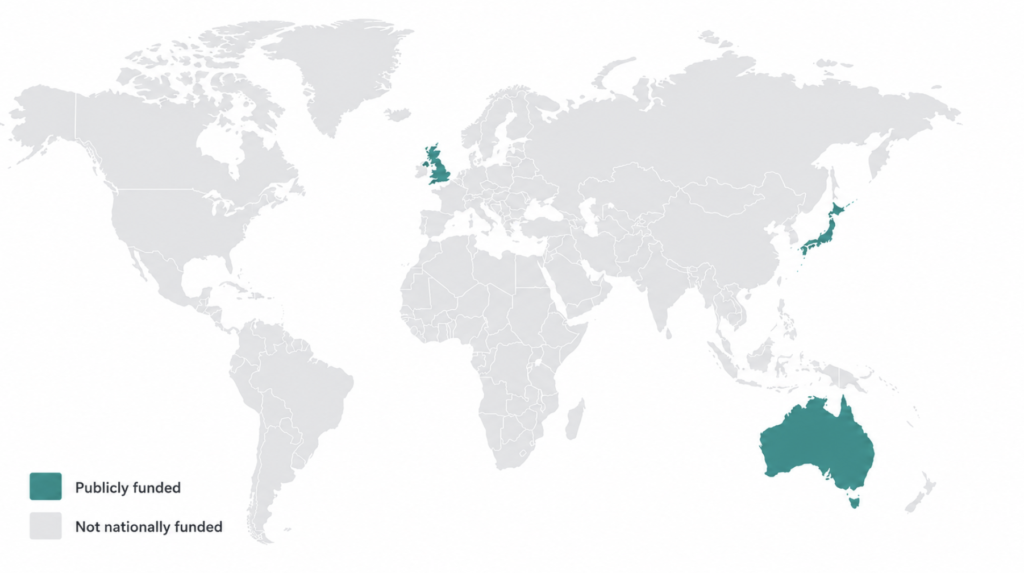
- Funding varies widely: the vaccine is publicly free for eligible groups in the UK and Australia but, in Korea, depends on local-government programs rather than a national scheme.
FAQ: Shingles Vaccine and Hearing Loss
Can the shingles vaccine prevent Ramsay Hunt syndrome? It is very likely to reduce the risk, though this has not been proven directly. Ramsay Hunt syndrome is herpes zoster affecting the facial nerve, and randomized trials show the vaccine prevents shingles by 90–97%. Lowering shingles overall should lower the ear-and-face form too, but no trial has measured Ramsay Hunt specifically as an outcome.
Does shingles cause sudden hearing loss? It can. When VZV reactivates near the ear, it can damage the vestibulocochlear nerve, producing hearing loss, tinnitus, and vertigo. In some cases hearing loss appears with little or no rash, which is why an ENT evaluation matter. However, VZV reactivation involving the facial nerve primarily manifests as facial palsy. In addition, routine use of antiviral agents for VZV reactivation in the facial nerve is not recommended.
Is the shingles vaccine really a “dementia vaccine”? No. The vaccine’s established purpose is preventing shingles. Observational and natural-experiment studies suggest a possible association with lower dementia risk, but they are not randomized trials and cannot prove causation. Treat any cognitive benefit as an unproven potential bonus, and get vaccinated for the established reason: preventing shingles.
Live or recombinant vaccine — which is better? The recombinant (non-live) two-dose vaccine is now preferred in most countries. It maintains high efficacy in older adults and can be given to many people with weakened immune systems who cannot receive the live vaccine.
Is the shingles vaccine free? Usually not automatically. Shingles vaccination is not usually a part of national immunization program except for few countires (e.g. UK, Australia..). Check with your national immunization program or district health center and clinic before assuming it is free.
References
- Lal H, Cunningham AL, Godeaux O, et al. Efficacy of an adjuvanted herpes zoster subunit vaccine in older adults. N Engl J Med. 2015;372(22):2087-2096.
- Cunningham AL, Lal H, Kovac M, et al. Efficacy of the herpes zoster subunit vaccine in adults 70 years of age or older. N Engl J Med. 2016;375(11):1019-1032.
- Eyting M, Xie M, Michalik F, Heß S, Chung S, Geldsetzer P. A natural experiment on the effect of herpes zoster vaccination on dementia. Nature. 2025;641(8062):438-446.
- Xie M, Eyting M, Bommer C, Ahmed H, Geldsetzer P. The effect of shingles vaccination at different stages of the dementia disease course. Cell. 2025;188(24):7049-7064.
- Kang JH, Ho JD, Chen YH, Lin HC. Increased risk of stroke after a herpes zoster attack: a population-based follow-up study. Stroke. 2009;40(11):3443-3448.
- Coulson S, Croxson GR, Adams R, Oey V. Prognostic factors in herpes zoster oticus (Ramsay Hunt syndrome). Otol Neurotol. 2011;32(6):1025-1030.
- Monsanto RD, Bittencourt AG, Bobato Neto NJ, Beilke SC, Lorenzetti FT, Salomone R. Treatment and prognosis of facial palsy on Ramsay Hunt syndrome: results based on a review of the literature. Int Arch Otorhinolaryngol. 2016;20(4):394-400.
Joonpyo Hong, MD is a board-certified otolaryngologist practicing in Korea. This article reflects his clinical interpretation of published research and does not constitute individual medical advice.
For more interesting contents:
https://curiousmd.com/japanese-encephalitis-vaccine/
https://curiousmd.com/ramsay-hunt-syndrome-facial-paralysis/
https://curiousmd.com/hpv-vocal-cord-cancer-young-non-smokers/
Link out to:
CDC – Shingles Vaccination (primary authority for the 90–97% efficacy data): https://www.cdc.gov/shingles/vaccines/index.html
CDC – Clinical Overview of Shingles (VZV reactivation & nerve involvement):
https://www.cdc.gov/shingles/hcp/clinical-overview/index.html
NHS – Who Can Get the Shingles Vaccine (reinforces the country-funding comparison):
https://www.nhsinform.scot/healthy-living/immunisation/shingles-vaccine/who-can-get-the-shingles-vaccine/