
TMS therapy can treat depression without a single pill — using a magnetic coil that pulses against the scalp for a few minutes a day. After more than 15 years of FDA-cleared use, transcranial magnetic stimulation (TMS) has moved from curiosity to mainstream psychiatric tool. This article covers how it works, the conditions it treats well, where the evidence is still uncertain, and the honest answer to a question many ENT patients ask: does it help tinnitus?
How TMS Therapy Works
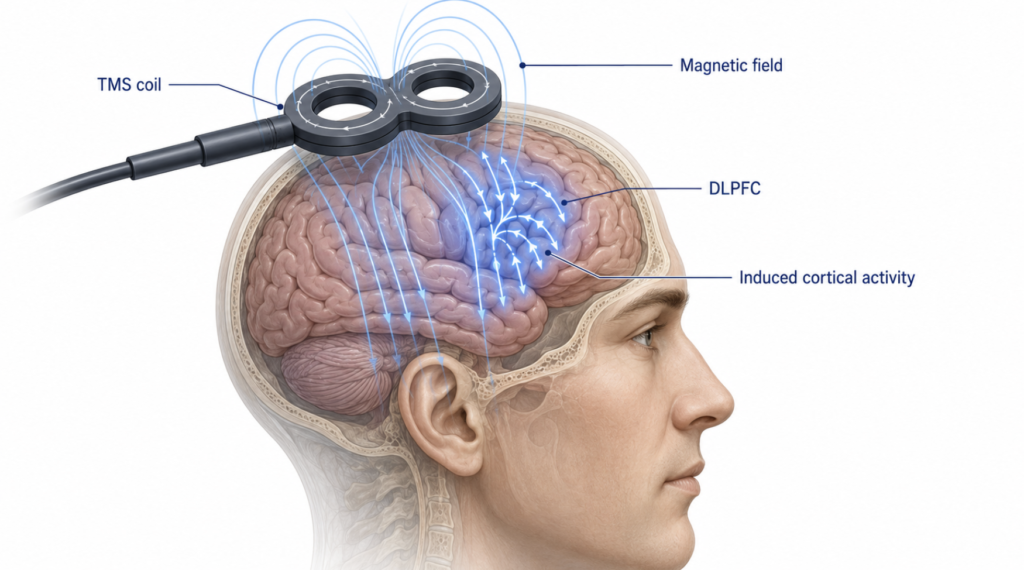
TMS rests on a simple piece of physics: a changing magnetic field induces an electric current. A coil placed on the scalp delivers brief, focused magnetic pulses that pass painlessly through the skull and trigger small electrical currents in the cortex beneath. Those currents make nearby neurons fire, and repeated sessions appear to shift the excitability of targeted circuits in lasting ways — a plasticity effect similar in spirit to long-term potentiation.
Most protocols target the dorsolateral prefrontal cortex (DLPFC), a region tied to mood regulation. The treatment is non-invasive and requires no anesthesia; patients stay awake and usually return to normal activity immediately after a session.
FDA-Approved Conditions
TMS first earned FDA clearance for major depressive disorder in adults in 2008. Since then, approved indications have expanded to obsessive-compulsive disorder (2018), smoking cessation (2020), and depression with comorbid anxiety. In 2024 and 2025, several manufacturers received clearance to treat adolescent depression, extending the therapy to patients as young as 15.
Migraine is also FDA-cleared, but with an important distinction worth understanding. Migraine uses single-pulse TMS (sTMS) — a handheld, often home-use device that delivers one magnetic pulse to interrupt the cortical wave thought to trigger an attack. The depression, OCD, and smoking indications instead use repetitive TMS (rTMS or deep TMS), which delivers trains of pulses in a clinic to reshape circuit activity over weeks. Same underlying physics, different machines and protocols.

Across the psychiatric indications, a consistent pattern emerges: TMS performs best for disorders of mood and compulsion that involve identifiable prefrontal circuits.
Where TMS Works Well
The strongest evidence is in treatment-resistant depression — patients who have failed at least one antidepressant. A 2024 meta-analysis of randomized trials found that deep TMS produced a response in roughly 45% of patients versus 24% on sham, and remission in 38% versus 14% [Lan XJ, Deep transcranial magnetic stimulation for treatment-resistant depression, 2024]. Those are meaningful numbers for people who have run out of medication options.
OCD is the second best-supported use. A meta-analysis of 25 randomized trials reported a moderate benefit and roughly a threefold higher chance of treatment response compared with sham [Steuber ER, A Meta-analysis of Transcranial Magnetic Stimulation in Obsessive-Compulsive Disorder, 2023].
A large dose-response analysis spanning multiple mental disorders confirmed that depression and OCD show the clearest, most reproducible responses to specific stimulation patterns, while also mapping which coil positions and frequencies matter most [Sabé M, Transcranial Magnetic Stimulation and Transcranial Direct Current Stimulation Across Mental Disorders, 2024].
Where the Evidence Is Still Unclear
For many other conditions, TMS is studied but not proven. Trials are ongoing in PTSD, substance use disorders, chronic pain, stroke rehabilitation, and autism, with mixed or preliminary results.
The picture is especially cautious for neurodegenerative disease. A comprehensive review of 70 studies in Alzheimer’s, Parkinson’s, and related dementias concluded that the therapeutic benefit remains inconclusive, limited by small trials and inconsistent protocols [Sanches C, Past, Present, and Future of Non-invasive Brain Stimulation Approaches to Treat Cognitive Impairment in Neurodegenerative Diseases, 2021]. A promising mechanism is not the same as a proven outcome — a distinction that matters when patients are paying out of pocket.
Does TMS Work for Tinnitus?
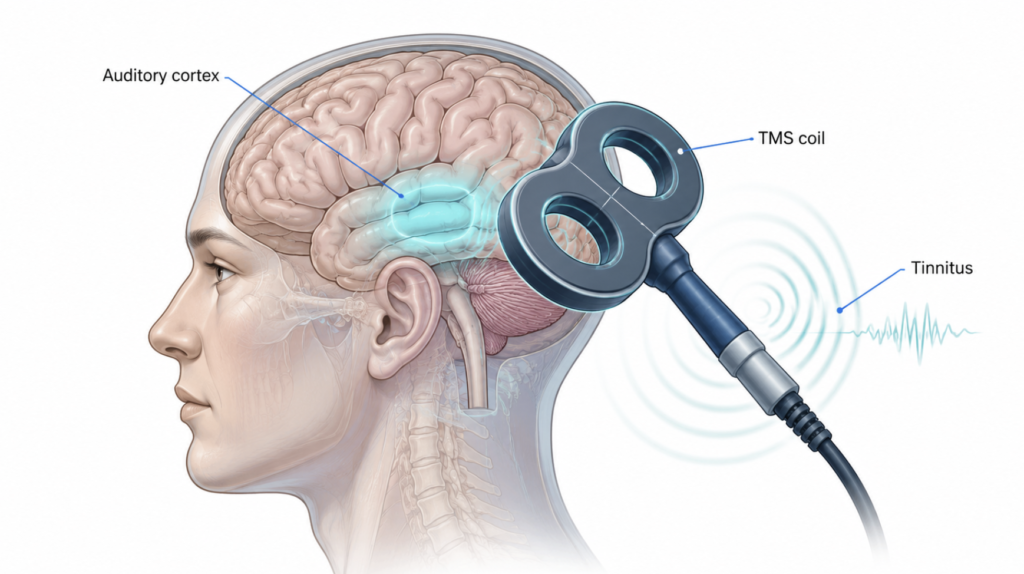
Here the honest answer is: partially, and not durably. Chronic tinnitus affects an estimated 10–15% of adults, and because it has no reliable cure, rTMS has been studied as a way to quiet overactive auditory cortex.
A 2025 meta-analysis of 16 randomized trials (1,105 patients) found that rTMS did outperform sham treatment on tinnitus severity scores at one month — but that advantage disappeared by six months [He Z, Efficacy of repetitive transcranial magnetic stimulation for subjective chronic tinnitus, 2025]. In other words, TMS may offer short-term relief for some people with tinnitus, but the evidence does not yet support it as a lasting fix. It remains off-label for this use.
Clinical Perspective
From an ENT standpoint, the gap between psychiatric and auditory applications is striking. For treatment-resistant depression and OCD, the evidence justifies real confidence. For tinnitus, the right posture is cautious optimism — TMS is worth watching, but patients should be wary of any clinic promising a “cure.” Established approaches still form the backbone of tinnitus care: hearing aids where hearing loss is present, sound therapy, and cognitive behavioral therapy.
Current Limitations and Future Directions
TMS has real constraints. Effects can fade, so many patients need maintenance sessions; a standard course requires daily visits over several weeks; and not everyone responds. Cost and time remain barriers.
The next generation aims to fix these problems. Accelerated protocols compress weeks of treatment into days, and image-guided targeting tailors the coil position to each patient’s brain anatomy. For tinnitus specifically, researchers are refining which cortical target and stimulation pattern might produce durable benefit. The technology is improving faster than the evidence — which is exactly why careful interpretation matters.
Key Takeaways
- TMS uses magnetic pulses to stimulate brain circuits and is non-invasive, requiring no anesthesia.
- The strongest evidence supports treatment-resistant depression and OCD, where response rates roughly double those of sham treatment.
- For tinnitus, TMS shows short-term benefit at one month but no proven effect at six months, and it remains off-label.
- Evidence is still inconclusive for neurodegenerative diseases, PTSD, and chronic pain.
- Patients should be skeptical of any provider promising a tinnitus “cure” with TMS.
FAQ
How does TMS work? TMS works by generating a magnetic field that induces small electrical currents in the brain. A coil placed on the scalp delivers focused pulses that pass through the skull and stimulate neurons in a targeted region, most often the prefrontal cortex. Repeated sessions gradually shift the activity of those circuits, which is thought to underlie the therapeutic effect in conditions like depression.
What conditions is TMS FDA-approved for? TMS is FDA-cleared for major depressive disorder, obsessive-compulsive disorder, smoking cessation, migraine, and depression with comorbid anxiety. Clearance was extended to adolescent depression in 2024 and 2025. Many other uses, including tinnitus, are considered off-label.
Can TMS cure tinnitus? No — current evidence does not support TMS as a cure for tinnitus. A 2025 meta-analysis found short-term improvement at one month that did not persist at six months. TMS may help some patients temporarily, but it is not an approved or reliable long-term treatment, and standard therapies remain first-line.
Is TMS safe? TMS is generally well tolerated, with patients awake throughout and no anesthesia required. The most common side effects are mild scalp discomfort or headache, and the most serious risk, a seizure, is rare. The main absolute contraindication is metal or electronic hardware near the coil — most notably a cochlear implant, which holds a magnet and electronics under the scalp that the magnetic pulse can damage or heat. This caution is especially relevant in ENT care, since some patients exploring TMS for tinnitus also have hearing implants.
References
He Z, Liao D, Ji Q, Yan S, Ai S. Efficacy of repetitive transcranial magnetic stimulation for subjective chronic tinnitus: a randomized controlled trial meta-analysis. Front Neurosci. 2025;19:1579846.
Lan XJ, Yang XH, Mo Y, Deng CJ, Huang XB, Cai DB, Zheng W. Deep transcranial magnetic stimulation for treatment-resistant depression: a systematic review and meta-analysis of randomized controlled studies. Asian J Psychiatr. 2024;96:104032.
Sabé M, Hyde J, Cramer C, Eberhard A, Crippa A, Brunoni AR, Aleman A, Kaiser S, Baldwin DS, Garner M, Sentissi O, Fiedorowicz JG, Brandt V, Cortese S, Solmi M. Transcranial magnetic stimulation and transcranial direct current stimulation across mental disorders: a systematic review and dose-response meta-analysis. JAMA Netw Open. 2024;7(5):e2412616.
Sanches C, Stengel C, Godard J, Mertz J, Teichmann M, Migliaccio R, Valero-Cabré A. Past, present, and future of non-invasive brain stimulation approaches to treat cognitive impairment in neurodegenerative diseases: time for a comprehensive critical review. Front Aging Neurosci. 2021;12:578339.
Steuber ER, McGuire JF. A meta-analysis of transcranial magnetic stimulation in obsessive-compulsive disorder. Biol Psychiatry Cogn Neurosci Neuroimaging. 2023;8(11):1145-1155.
Joonpyo Hong, MD is a board-certified otolaryngologist practicing in Korea. This article reflects his clinical interpretation of published research and does not constitute individual medical advice.
For more interesting contents:
https://curiousmd.com/ai-chatbot-for-tinnitus/
https://curiousmd.com/tinnitus-bimodal-stimulation-cbt-2026/