
Apple Watch sleep apnea accuracy has quickly become one of the most common questions in primary care and sleep clinics. Since Apple’s sleep apnea notification received FDA clearance in September 2024, a feature sitting on tens of millions of wrists has begun sending people to doctors who would never otherwise have come. That is genuinely useful. But the underlying question — do I have sleep apnea? — cannot be answered by a watch, and understanding why explains almost everything about where this technology helps and where it quietly misleads.
What follows is how the feature works, where it sits relative to a formal sleep study, and the central tension that matters most: the same enormous scale that makes Apple’s data powerful is also what makes it data that must be treated with caution.
How the feature actually works (and why “Breathing Disturbances” is not “AHI”)

Sleep apnea is diagnosed by counting events. Each time breathing stops (an apnea) or becomes shallow enough to lower blood oxygen (a hypopnea), it counts. Summed and divided by hours of sleep, these events produce the apnea-hypopnea index (AHI) — fewer than 5 is normal, 5 to 14 is mild, 15 to 29 is moderate, and 30 or more is severe [Kapur, Clinical Practice Guideline for Diagnostic Testing for Adult OSA, 2017].
The Apple Watch does not measure airflow, oxygen, or brain activity directly. Instead, its accelerometer picks up the tiny body movements that breathing produces, and a machine-learning model turns those signals into a metric Apple calls Breathing Disturbances. Apple is explicit in its own technical documentation that this metric is not equivalent to the AHI (Apple Inc., Estimating Breathing Disturbances and Sleep Apnea Risk from Apple Watch, 2024). It is a proxy — an educated estimate built on indirect evidence.
The notification logic is conservative by design. The watch evaluates a user’s data in 30-day blocks, requires at least 10 nights of recording in that window, and flags a user only if at least half of those nights show elevated Breathing Disturbances consistent with moderate-to-severe disease (Apple Inc., 2024). In other words, it is not a nightly verdict, it ignores mild apnea entirely, and it is explicitly not intended for people already diagnosed with sleep apnea.
The three-tier diagnostic ladder
The clearest way to place the Apple Watch is to see sleep apnea testing as a ladder with three rungs.
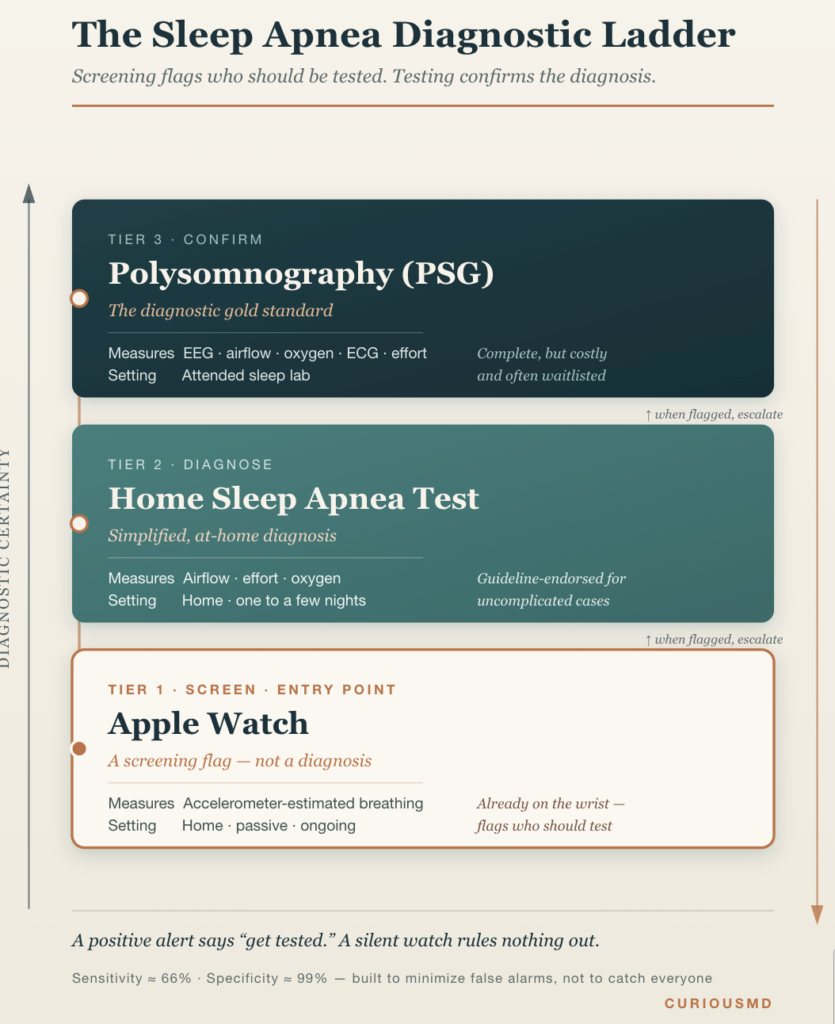
| Polysomnography (PSG) | Home Sleep Apnea Test (HSAT) | Apple Watch | |
|---|---|---|---|
| Role | Diagnosis (confirm) | Diagnosis (simplified) | Screening (flag) |
| What it measures | EEG, eye movement, muscle, ECG, airflow, oxygen, effort | Airflow, respiratory effort, oxygen | Accelerometer-estimated breathing |
| Setting | Sleep lab, attended | Home, one to a few nights | Home, passive, ongoing |
| Output | Full sleep architecture + AHI | AHI | “Possible apnea” notification |
| Access | Limited, costly, waitlisted | Moderate cost, prescription | Already on the wrist |
PSG is the gold standard, and for good reason — it is the only test that captures the full picture of sleep, including disorders that mimic or accompany apnea [Kapur, 2017]. But that completeness is also its weakness. PSG is expensive, requires trained staff and a lab bed, and carries waiting lists that stretch for months in many health systems. Sleeping in an unfamiliar room wired to a dozen sensors also distorts the very thing it aims to measure — the “first-night effect.”
HSAT was created to relieve exactly that bottleneck, and clinical guidelines now endorse it for uncomplicated patients with a high probability of moderate-to-severe OSA [Kapur, 2017]. The Apple Watch sits one rung below even that: it does not diagnose anything. It decides whether a person should climb onto the ladder at all.
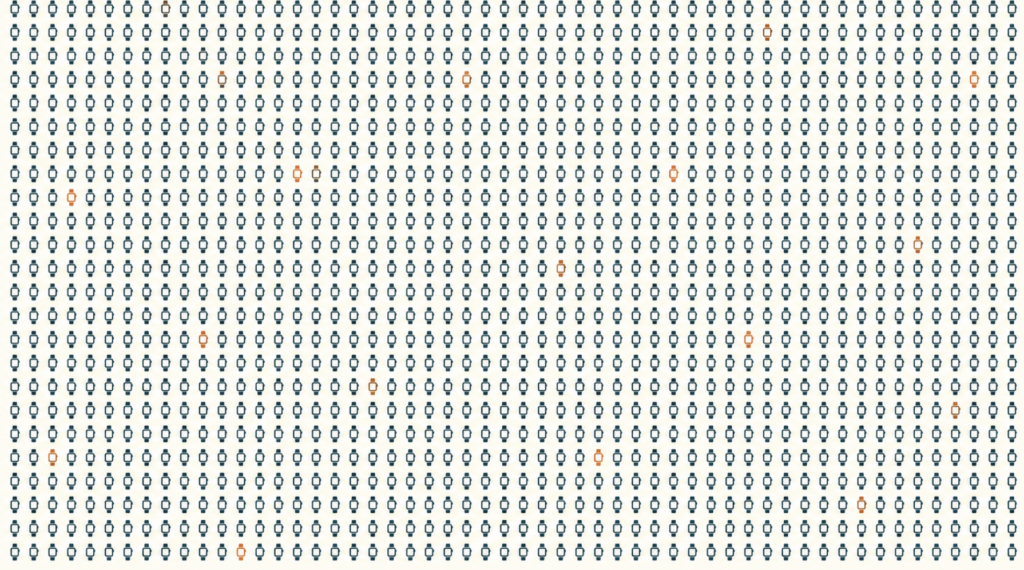
The real strength: scale
Here is what no sleep lab can do. Apple did not build the most accurate sleep sensor — it put a decent one on a device that hundreds of millions of people already wear every night, voluntarily, without a referral or a prescription or a symptom frightening enough to drive them into care.
That matters because sleep apnea is both common and largely invisible. An estimated 425 million adults worldwide have moderate-to-severe OSA, and close to a billion have at least mild disease [Benjafield, Estimation of the Global Prevalence and Burden of Obstructive Sleep Apnoea, 2019]. A large majority remain undiagnosed, in part because the people who have it are often asleep when it happens and feel “fine” during the day [Peppard, Increased Prevalence of Sleep-Disordered Breathing in Adults, 2013]. No one can self-refer for a condition they do not know they have.
Passive, opportunistic screening at this scale is something medicine has never had before. The watch accumulates a long time-series across dozens of nights in a person’s actual bedroom — far more nights, in far more natural conditions, than any sleep study captures. As a screening funnel that quietly identifies candidates and nudges them toward testing, the population-health potential is enormous.
Clinical Perspective. The feature’s true value is behavioral, not diagnostic. A patient who arrives holding a watch alert is worth far more to medicine than one who never arrives at all. Its real job is to convert an undiagnosed person into a tested person — and on that narrow task it may accomplish more than a decade of public-awareness campaigns. It deserves to be taken seriously rather than dismissed as a gadget.
The flip side: can the data be trusted?: Apple Watch Sleep Apnea Accuracy
The caution follows directly from the strength. The same scale that makes this data powerful is exactly what makes it data worth questioning.
A sleep study generates a small amount of carefully curated data. A technician checks that the sensors are seated, the environment is controlled, and the recording is clean. Apple’s validation studies were run the same way — controlled conditions, screened participants, expert-scored ground truth. A watch worn at home has none of that supervision. It collects indiscriminately: a night in an unfamiliar hotel, a night after too much alcohol, a night with a loose band, a night spent asleep on the couch with the watch half off. All of it flows into the same pile.
This is the crux: a large volume of data is not the same as reliable data. Unscreened, real-world signals carry noise that no algorithm fully removes — motion artifacts, inconsistent wear, position changes, differences between watch models. When millions of such nights are aggregated, the sheer quantity can create an illusion of precision that the underlying signal does not earn. A confident-looking number on a clean screen hides the fact that it is a probabilistic estimate built on indirect movement data.
There is also a quieter problem of who generates the data. The people most likely to wear an Apple Watch skew younger, wealthier, and more health-conscious. The people at highest risk for serious apnea skew older, heavier, and often less connected to this kind of technology. Consumer-device validation studies have largely been run in healthy young adults under lab conditions, which limits how confidently the results transfer to the patients who need screening most [Robbins, Accuracy of Three Commercial Wearable Devices for Sleep Tracking in Healthy Adults, 2024].
Clinical Perspective. Aggregated consumer data should not be mistaken for epidemiological truth. It is an excellent hypothesis generator and a poor final answer. A patient’s watch summary is best read as a story about their nights — useful and suggestive, but requiring verification before it informs any treatment decision.
What “66% sensitivity” really means
The numbers Apple reported to regulators capture this precisely. In a clinical validation of roughly 1,500 participants, the notification reached a sensitivity of about 66% and a specificity of about 99%, with specificity near 100% in people whose breathing was actually normal (Apple Inc., Estimating Breathing Disturbances and Sleep Apnea Risk from Apple Watch, 2024). The algorithm was deliberately tuned to favor specificity — to almost never cry wolf.
Read in plain language, those two numbers describe the whole clinical picture.
High specificity means a positive alert is trustworthy. A watch that indicates possible moderate-to-severe apnea is very probably right, and testing is warranted. False alarms are rare.
Moderate sensitivity means a negative result is nearly meaningless. A sensitivity of 66% implies the feature misses roughly one in three people who genuinely have moderate-to-severe apnea — and by design, it ignores mild apnea altogether. A quiet watch is not a clean bill of health.
Clinical Perspective. The real danger is not the false positive — Apple engineered that risk away — but false reassurance. A person with loud snoring, witnessed breathing pauses, and disabling daytime fatigue may conclude they “must be fine” simply because no alert ever arrived. That reasoning is backwards and potentially harmful. When symptoms point to apnea, a silent watch should change nothing about the decision to seek evaluation. The alert is worth trusting when it fires; the silence is worth ignoring when it does not.

Where this is heading
The trajectory is promising if expectations stay honest. Fusing more signals — oxygen saturation, heart rate, temperature — onto the existing accelerometer base could lift sensitivity without sacrificing the excellent specificity. A clean referral pathway, where a watch alert routes automatically to an HSAT and, when needed, to a full PSG, could turn the bottom rung of the ladder into a genuine pipeline that eases the diagnostic backlog rather than flooding clinics with worried-but-well patients.
The honest limits will remain, though. The watch cannot distinguish obstructive from central apnea, cannot diagnose the many sleep disorders that are not apnea, and cannot replace a measurement of airflow and oxygen with a measurement of wrist motion. It is a smarter front door, not a new house.
Clinical Perspective. The bottom line: the Apple Watch sleep apnea feature is one of the most useful screening tools to reach the public in years, precisely because it meets people where they already are. But its intelligence lives in the alert, not in the absence of one, and its data — for all its volume — is the start of a conversation with a clinician, never the end of one. Treated as an invitation to be tested, the notification does exactly the job it deserves to do.
Key Takeaways
- The Apple Watch screens for, but does not diagnose, sleep apnea — its “Breathing Disturbances” metric is an accelerometer-based estimate, not the clinical apnea-hypopnea index.
- A notification is highly trustworthy (specificity near 99%); the absence of one is not (sensitivity around 66%), so a silent watch does not rule out apnea.
- The feature targets moderate-to-severe apnea only and ignores mild disease by design.
- The watch’s greatest strength — massive, passive scale across millions of users — is also the source of its greatest weakness: unscreened, noisy, real-world data that volume alone cannot make reliable.
- The right clinical use is as a front door: act decisively on a positive alert, and disregard a negative one when symptoms suggest a problem.
FAQ
Can an Apple Watch diagnose sleep apnea? No. The Apple Watch can only flag a possibility and prompt a person to seek testing. A formal diagnosis requires a sleep study — either in-lab polysomnography or a home sleep apnea test — that measures airflow and oxygen directly [Kapur, 2017]. The watch’s signal is an estimate derived from movement, not a clinical measurement.
How accurate is the Apple Watch sleep apnea feature? It is very accurate when it raises an alert and much less accurate when it stays silent. Apple’s regulatory data show specificity near 99% but sensitivity around 66%, meaning positive alerts are reliable while roughly a third of true moderate-to-severe cases are missed (Apple Inc., 2024). It is built to minimize false alarms, not to catch everyone.
Does no notification mean there is no sleep apnea? No, and this is the most important misunderstanding to avoid. Because sensitivity is only about 66% and mild apnea is excluded by design, many people with real apnea will never be flagged. Loud snoring, gasping at night, or persistent exhaustion despite adequate sleep all warrant a medical evaluation regardless of what the watch shows.
Apple Watch versus a sleep study — what’s the difference? A sleep study directly measures breathing, oxygen, and often brain activity to produce a diagnosis; the Apple Watch infers breathing patterns from wrist motion to produce a screening flag [Kapur, 2017]. The watch is the device that signals whether a sleep study is needed, not a replacement for one.
References
- Benjafield AV, Ayas NT, Eastwood PR, et al. Estimation of the global prevalence and burden of obstructive sleep apnoea: a literature-based analysis. Lancet Respir Med. 2019;7(8):687-698.
- Kapur VK, Auckley DH, Chowdhuri S, Kuhlmann DC, Mehra R, Ramar K, Harrod CG. Clinical Practice Guideline for Diagnostic Testing for Adult Obstructive Sleep Apnea: An American Academy of Sleep Medicine Clinical Practice Guideline. J Clin Sleep Med. 2017;13(3):479-504.
- Peppard PE, Young T, Barnet JH, Palta M, Hagen EW, Hla KM. Increased prevalence of sleep-disordered breathing in adults. Am J Epidemiol. 2013;177(9):1006-1014.
- Robbins R, Weaver MD, Sullivan JP, Quan SF, Gilmore K, Shaw S, Benz A, Qadri S, Barger LK, Czeisler CA, Duffy JF. Accuracy of Three Commercial Wearable Devices for Sleep Tracking in Healthy Adults. Sensors (Basel). 2024;24(20):6532.
Note: Performance figures for the Apple Watch sleep apnea feature (sensitivity ~66%, specificity ~99%, notification logic) are drawn from Apple’s own technical documentation supporting its FDA clearance and are not, at the time of writing, published in a peer-reviewed journal. This distinction is itself relevant to the article’s argument about data and evidence tiers.
Joonpyo Hong, MD is a board-certified otolaryngologist practicing in Korea. This article reflects his clinical interpretation of published research and does not constitute individual medical advice. This article is not intended to advertise or promote any specific company or product.
For more interesting contents:
https://curiousmd.com/wearable-ai-for-sleep-apnea-2026/
https://curiousmd.com/child-snoring-not-normal-by-age/
https://curiousmd.com/sleep-cycles-by-age/
Link out to:
Apple’s official technical document (Estimating Breathing Disturbances and Sleep Apnea Risk from Apple Watch) — primary source for the 66% sensitivity / 99% specificity figures and the notification logic (30-day blocks, 10-night minimum, Breathing Disturbances metric), https://www.apple.com/health/pdf/sleep-apnea/Sleep_Apnea_Notifications_on_Apple_Watch_September_2024.pdf
FDA 510(k) clearance record (K240929) — official regulatory document confirming the September 2024 FDA clearance, https://www.accessdata.fda.gov/scripts/cdrh/cfdocs/cfpmn/pmn.cfm?ID=K240929
Kapur et al., AASM Clinical Practice Guideline for Diagnostic Testing (2017, full text on PMC) — basis for the AHI severity thresholds and the PSG/HSAT diagnostic ladder, https://pmc.ncbi.nlm.nih.gov/articles/PMC5337595/
Benjafield et al., Lancet Respiratory Medicine (2019, full text on PMC) — source for the global OSA prevalence (425 million moderate-to-severe) and undiagnosed-burden statistics, https://pmc.ncbi.nlm.nih.gov/articles/PMC7007763/
Apple Newsroom official announcement (September 2024) — background on the feature’s launch, intended users (adults 18+ without a prior diagnosis), and supported devices, https://www.apple.com/newsroom/2024/09/apple-introduces-groundbreaking-health-features/