
Have you ever wondered whether there is an evolutionary reason for allergies? Some researchers have noticed that people with allergies may have a lower risk of certain cancers, particularly in tissues exposed directly to the outside world — though this link is far from settled [Sherman, Allergies: Their Role in Cancer Prevention, 2008]. Observations like this raise an intriguing possibility: that a runny nose, sneezing, and itchy eyes might not be a simple malfunction, but the visible edge of an old defense system.
This article looks at allergies from two angles. First, the evolutionary “why”: several competing hypotheses for why this seemingly self-defeating reaction exists at all. Then the practical “what it means for you”: straight answers to the questions patients ask me most about allergic rhinitis, heredity, and asthma.
A note before we start. The evolutionary ideas below are hypotheses, not settled theory. They are useful frameworks supported by suggestive evidence, but none has been definitively proven, and researchers still disagree about them.
So What Is the Evolutionary Reason for Allergies?
From a survival standpoint, allergy looks like a design flaw. The immune system mounts a violent, sometimes fatal response to pollen, peanuts, or cat dander — things that pose no real threat. Why would evolution preserve a system that occasionally kills its owner over a bee sting?
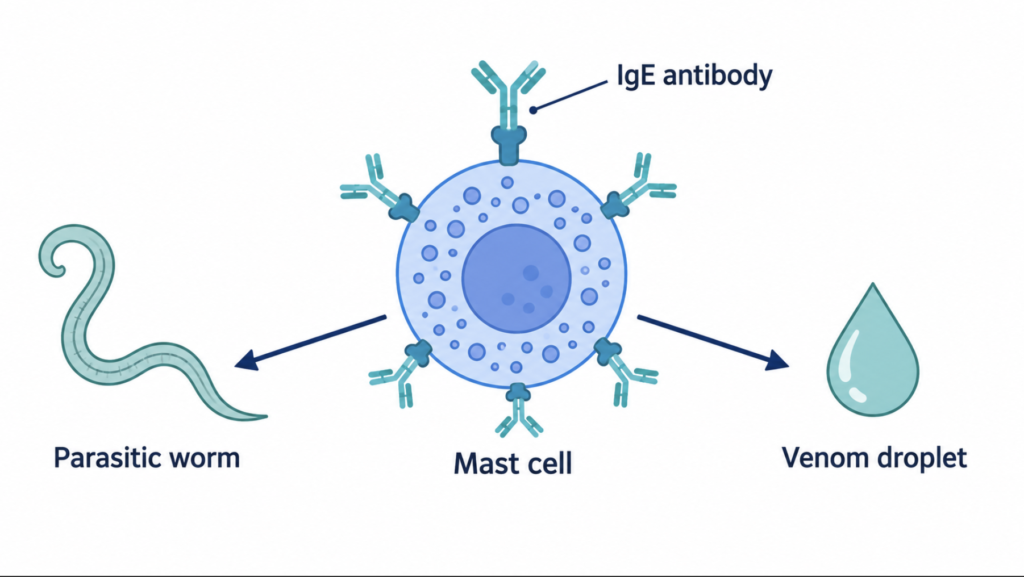
The conservative logic of evolution offers a clue. The antibody class behind allergy, IgE, along with mast cells and the whole machinery of the allergic response, is ancient and conserved across mammals. Traits that are purely harmful tend to be selected out. Their persistence suggests the system was doing something useful, and that allergy is the misfire of an otherwise valuable tool.
The parasite hypothesis
The most established idea is that IgE evolved primarily to defend against large parasites — helminths (worms) and arthropods — rather than microbes. Sneezing, coughing, mucus, itching, and gut cramping are all effective ways to physically expel or dislodge a parasite from the skin, airway, or gut.
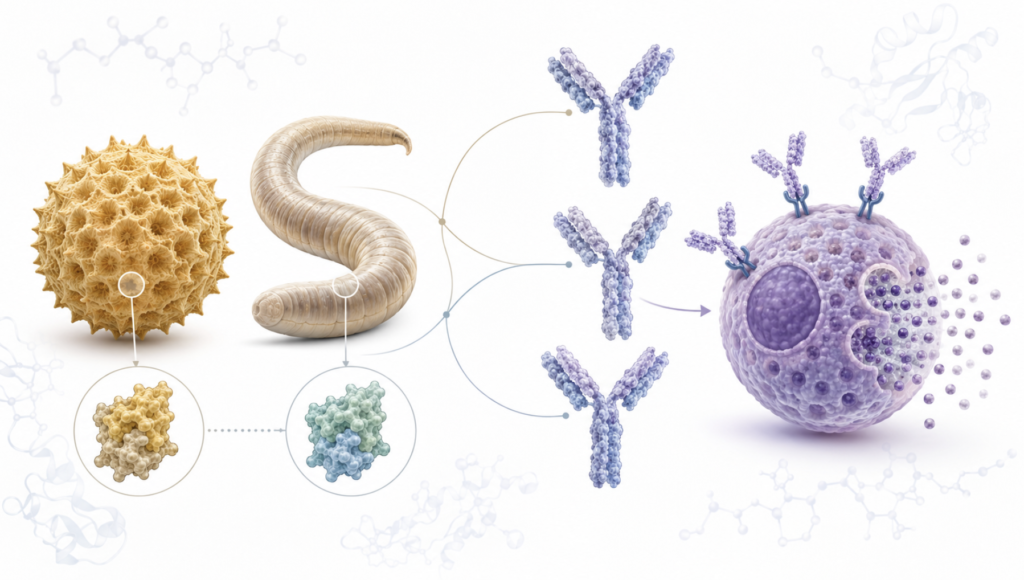
A 2015 computational study gave this idea molecular weight. Researchers systematically compared allergenic proteins with parasite proteins and found striking structural similarities, concluding that allergens look “like” parasites to the immune system [Tyagi, Comparisons of Allergenic and Metazoan Parasite Proteins: Allergy the Price of Immunity, 2015]. In their framing, allergy is the price we pay for anti-parasite immunity. Again, this is a hypothesis — a compelling correlation, not proof of cause.
The toxin hypothesis
A second, complementary idea was proposed in 1991: that the allergic response evolved as a last line of defense against environmental toxins, such as venoms and toxic plant compounds [Profet, The Function of Allergy: Immunological Defense Against Toxins, 1991]. Under this view, vomiting, diarrhea, tearing, and sneezing are mechanisms to expel a toxin fast, and the discomfort is the point.
For decades this was largely dismissed. Then a 2013 Stanford experiment offered support: mice given a low, sting-equivalent dose of honeybee venom became more resistant to a later lethal dose, and that protection depended on IgE [Marichal, A Beneficial Role for Immunoglobulin E in Host Defense Against Honeybee Venom, 2013]. It was among the first hard evidence that an “allergic-type” IgE response could actually reduce the toxicity of a real poison. Whether the same holds in humans is still unknown.
The toxin hypothesis also loops back to that opening fact. If allergy helps expel carcinogen-bearing particles from exposed tissues, lower cancer rates in those tissues would make sense — which is exactly the pattern Sherman and colleagues reported, though they were careful to call it support for a hypothesis, not a settled mechanism [Sherman, Allergies: Their Role in Cancer Prevention, 2008].
Are We Just “Too Clean”?
If allergy is an old defense, why does it seem so much more common now? The classic answer is the hygiene hypothesis. In 1989 a short paper noted that British children from larger families had less hay fever, and proposed that early exposure to infection might protect against allergy [Strachan, Hay Fever, Hygiene, and Household Size, 1989]. The term “hygiene hypothesis” came later, and the original paper never used it.
The idea has since been refined into what is often called the “old friends” hypothesis. The argument is that the exposures our immune system actually needs are not cold-and-flu pathogens, but the microbes and parasites we co-evolved with over hundreds of thousands of years [Rook, The Hygiene Hypothesis and the Increasing Prevalence of Chronic Inflammatory Disorders, 2007]. Without enough of this early “training,” the immune system is thought to become poorly regulated and quick to overreact to harmless antigens.
Worth repeating: this is a hypothesis under active debate. Decades of work have not pinned down a single clean mechanism, and the “too clean” framing is an oversimplification of a much messier picture.
Clinical Perspective The evolutionary view is useful as context rather than as a diagnosis. It helps explain why allergy clusters in families and rises in urban environments, but it does not change the clinical workup. Genes, indoor allergen exposure, air quality, the gut microbiome, and the integrity of the nasal lining all contribute together. Evolution sets the stage; the individual case is where management decisions are made.
What This Means for You: 5 Common Questions
Beyond the evolutionary theory, the practical questions are the ones that come up most often — about heredity, children, and asthma. Here are clear answers to five of them.
1. Is allergic rhinitis hereditary? Yes, it tends to run in families — but what is inherited is a tendency, not the disease itself. More precisely, you inherit a predisposition to mount allergic (IgE) responses, which is why rhinitis, asthma, and atopic dermatitis often cluster within the same family rather than appearing in isolation.
2. If a parent has allergic rhinitis, how likely is the child to have it? When one parent is atopic, the child has more than a 50% chance of developing atopic symptoms; when both parents are affected, that figure rises to as much as 80% [Kolb, Atopic Dermatitis, 2023]. These are estimates for allergic disease in general, not a guarantee the child will develop rhinitis specifically. Genetics, allergen exposure, air pollution, smoke, and early infections all interact.
3. Are specific allergens — like dust mites — inherited? Not directly. You do not inherit a “dust mite allergy” as such; you inherit a tendency to become sensitized and to produce IgE readily. So it is more accurate to say a family shares a predisposition to react to dust mites or pollen than to say a particular allergy is passed down.
4. Does asthma raise the chance of allergic rhinitis, and vice versa? Both directions are linked. A meta-analysis of nearly 275,000 people found that a history of allergic rhinitis was strongly associated with developing asthma, with a pooled odds ratio of 3.82 [Tohidinik, History of Allergic Rhinitis and Risk of Asthma; a Systematic Review and Meta-Analysis, 2019]. This reflects the “one airway” concept: the upper and lower airways are continuous, so inflammation rarely stays politely in one place.
5. Can someone with only allergic rhinitis suddenly develop asthma as an adult? Yes. Allergic rhinitis is a recognized risk factor for asthma, and lower-airway symptoms can emerge years later, including in adulthood. So “I only had rhinitis as a kid” does not rule out adult-onset asthma. New cough, wheeze, nighttime symptoms, or exercise-triggered breathlessness deserve an asthma evaluation.
Key Takeaways
- Allergy may be an ancient defense system — against parasites or toxins — misfiring at harmless targets, though this remains a hypothesis rather than proven fact.
- People with allergies show lower rates of some cancers, a pattern that fuels the toxin hypothesis [Sherman, 2008].
- What is inherited is the allergic tendency, not a specific allergy; the risk exceeds 50% with one affected parent and reaches up to 80% with both [Kolb, 2023].
- A history of allergic rhinitis is strongly linked to asthma (pooled odds ratio 3.82), supporting a “one airway” approach [Tohidinik, 2019].
- Adult-onset asthma can follow childhood rhinitis, so new lower-airway symptoms warrant evaluation.
FAQ
What is the evolutionary reason for allergies? The leading hypotheses are that allergy evolved to defend against parasites or environmental toxins. IgE-driven reactions like sneezing and itching can expel worms or poisons, and allergens happen to resemble parasite proteins. These are well-supported ideas but not confirmed theories.
Why might allergic people get fewer cancers? One hypothesis is that allergic symptoms expel foreign particles, some carcinogenic, from exposed tissues before damage accumulates. A large 2008 review found more studies reporting lower cancer rates in allergy sufferers than higher ones, though the relationship varies by cancer type and is not proven causal.
Is allergic rhinitis hereditary? The predisposition is. Allergy clusters in families, and children of allergic parents are at higher risk, but environment heavily shapes whether and how it appears. Inheritance raises the odds; it does not seal the outcome.
Can allergic rhinitis turn into asthma? It can be a precursor. Rhinitis is a known risk factor for asthma, and the two share the same continuous airway. New cough, wheeze, or breathlessness in someone with rhinitis should prompt an asthma check.
Joonpyo Hong, MD is a board-certified otolaryngologist practicing in Korea. This article reflects his clinical interpretation of published research and does not constitute individual medical advice.
References
- Profet M. The function of allergy: immunological defense against toxins. Q Rev Biol. 1991;66(1):23-62.
- Marichal T, Starkl P, Reber LL, et al. A beneficial role for immunoglobulin E in host defense against honeybee venom. Immunity. 2013;39(5):963-975.
- Sherman PW, Holland E, Sherman JS. Allergies: their role in cancer prevention. Q Rev Biol. 2008;83(4):339-362.
- Tyagi N, Farnell EJ, Fitzsimmons CM, et al. Comparisons of allergenic and metazoan parasite proteins: allergy the price of immunity. PLoS Comput Biol. 2015;11(10):e1004546.
- Strachan DP. Hay fever, hygiene, and household size. BMJ. 1989;299(6710):1259-1260.
- Rook GA. The hygiene hypothesis and the increasing prevalence of chronic inflammatory disorders. Trans R Soc Trop Med Hyg. 2007 Nov;101(11):1072-4.
- Tohidinik HR, Mallah N, Takkouche B. History of allergic rhinitis and risk of asthma; a systematic review and meta-analysis. World Allergy Organ J. 2019;12(10):100069.
- Kolb L, Ferrer-Bruker SJ. Atopic Dermatitis. In: StatPearls. Treasure Island (FL): StatPearls Publishing; 2023.
For more interesting contents:
https://curiousmd.com/ai-allergy-forecast-personalized-prediction/
https://curiousmd.com/korea-2026-pollen-allergies/
https://curiousmd.com/anti-tslp-antibody-nasal-polyps/
Link out to:
https://journals.plos.org/ploscompbiol/article?id=10.1371%2Fjournal.pcbi.1004546
https://pmc.ncbi.nlm.nih.gov/articles/PMC4164235/
https://www.worldallergyorganizationjournal.org/article/S1939-4551(19)31223-2/fulltext