
Most people who walk into a clinic with a chronically runny, blocked nose assume they have an allergy. A large share of them do not, which is why telling allergic vs nonallergic rhinitis apart is the first real decision a clinician makes. In one comprehensive review, roughly a quarter of patients presenting with chronic rhinitis symptoms turned out to have a non allergic form, and the single most common nonallergic type, vasomotor rhinitis, accounted for about 80% of those cases [Baroody, Nonallergic Rhinopathy: A Comprehensive Review of Classification, Diagnosis, and Treatment, 2024].
That distinction is not academic hair-splitting. Allergic and nonallergic rhinitis can look almost identical at the bedside, yet they differ in what causes them, how they behave over time, and which treatments actually work. This article walks through how clinicians separate the two, why the separation changes management, what the nonallergic subtypes are and how their outlooks diverge, and what the current guidelines recommend for each.
Allergic vs Nonallergic Rhinitis: How to Distinguish
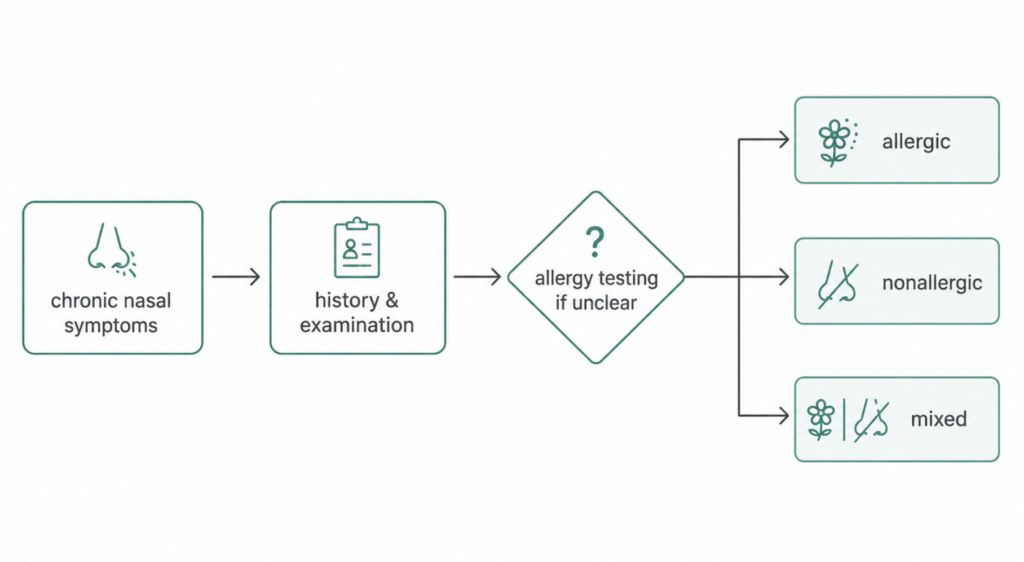
Allergic rhinitis (AR) is an IgE-mediated reaction to a specific allergen — pollen, house dust mite, animal dander, mold. Nonallergic rhinitis (NAR) produces the same headline symptoms (congestion, rhinorrhea, sneezing, postnasal drip) without that IgE-driven mechanism. Because the symptoms overlap so heavily, the diagnosis leans first on a careful history rather than a single test [Quillen, Diagnosing Rhinitis: Allergic vs. Nonallergic, 2006].
Clinical clues
Certain patterns push toward allergy. Seasonality, prominent sneezing, itching of the nose and palate, and accompanying eye symptoms (itchy, watery eyes) all point to AR, as does an early age of onset and a personal or family history of atopy. A pediatric study that modeled these features found seasonality, sneezing, moderate-to-severe symptoms, and a good response to antihistamines were independent predictors that separated AR from NAR at the primary-care level [Topal, Predictive Factors to Differentiate Between Allergic and Nonallergic Rhinitis in Children, 2014].
Nonallergic rhinitis tends to read differently. Onset is often later in life, there is usually no family history of allergy, and itching and eye involvement are less prominent. The triggers are telling: instead of pollen or pets, patients describe strong smells, perfumes, smoke, alcohol, spicy food, or shifts in temperature, humidity, and barometric pressure setting off their nose [Baroody, Nonallergic Rhinopathy: A Comprehensive Review of Classification, Diagnosis, and Treatment, 2024].

When allergy testing is needed
History and examination resolve most cases, but testing settles the ambiguous ones. Allergy testing — skin prick testing or allergen-specific IgE in blood — is not mandatory for every patient, but it is valuable when the picture is mixed or the diagnosis is uncertain [Quillen, Diagnosing Rhinitis: Allergic vs. Nonallergic, 2006]. The logic matters: NAR is fundamentally a diagnosis of exclusion, reached after IgE-mediated causes have been ruled out.
One caution belongs here. A negative allergy test does not automatically equal nonallergic disease. Some patients have local allergic rhinitis, where the allergic reaction is confined to the nasal mucosa and standard systemic tests come back negative — a reminder that “tests negative” and “not allergic” are not always the same statement.
| Feature | Allergic rhinitis | Nonallergic rhinitis |
|---|---|---|
| Mechanism | IgE-mediated | Non-IgE (neurogenic, irritant, hormonal, etc.) |
| Typical onset | Childhood / younger | Usually adult-onset (e.g., after age 20–35) |
| Triggers | Pollen, dust mite, dander, mold | Odors, smoke, temperature/pressure change, alcohol, food |
| Itching / eye symptoms | Common | Usually mild or absent |
| Seasonality | Often present | Usually absent (perennial) |
| Family history of atopy | Frequently present | Usually absent |
| Allergy testing | Positive | Negative (diagnosis of exclusion) |
Patterns, not absolutes — many patients sit somewhere between these columns.
Why the Distinction Matters
The reason to bother separating AR from NAR is simple: although their symptoms and signs are similar, their treatment and follow-up are different [Topal, Predictive Factors to Differentiate Between Allergic and Nonallergic Rhinitis in Children, 2014]. Mislabeling a nonallergic patient as allergic leads to therapies that underperform, repeated testing, and an unnecessary clinical and financial burden.
It is also rarely a clean either/or. Many patients have mixed rhinitis, carrying both an IgE-mediated and a nonallergic, neurogenic component at the same time [Baroody, Nonallergic Rhinopathy: A Comprehensive Review of Classification, Diagnosis, and Treatment, 2024]. By some estimates nearly half of patients labeled with allergic rhinitis actually carry a coexisting nonallergic component, making mixed rhinitis one of the most common patterns in practice [Settipane, Epidemiology of Rhinitis: Allergic and Nonallergic, 2007]. Recognizing the nonallergic contribution explains why a patient with confirmed pollen allergy still flares in response to cold air or perfume long after pollen season ends — and why treating only the allergy leaves them disappointed.
Types of Nonallergic Rhinitis — and Their Prognosis
“Nonallergic rhinitis” is not one disease but a collection of conditions that share a final common symptom set. The subtypes differ in mechanism and, importantly for patients, in how they tend to behave over time. The classification and trigger framework below follows a recent comprehensive review [Baroody, Nonallergic Rhinopathy: A Comprehensive Review of Classification, Diagnosis, and Treatment, 2024]; the prognostic generalizations are drawn largely from expert consensus and review-level evidence rather than randomized trials, so they describe tendencies, not guarantees.
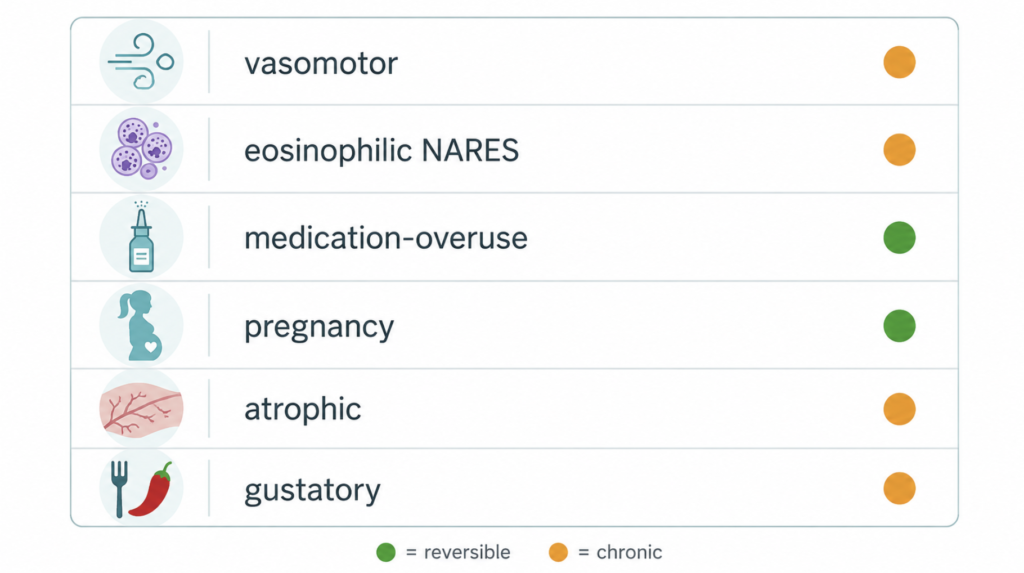
Vasomotor rhinitis (nonallergic rhinopathy / idiopathic rhinitis). The most common form, around 80% of NAR cases. It reflects a hyper-reactive, neurogenically driven nose responding to irritants and weather change, with transient receptor potential (TRP) ion channels increasingly implicated in its mechanism. It typically runs a chronic, relapsing-and-remitting course; the realistic goal is control of triggers and symptoms rather than cure.
Nonallergic rhinitis with eosinophilia syndrome (NARES). Defined by nasal eosinophilia in the absence of systemic allergy, often with a notably reduced sense of smell. It tends to be persistent, and is the subtype most worth watching closely: it is described as a risk factor for nasal polyposis, aspirin sensitivity, and obstructive sleep apnea [Ellis, Nonallergic Rhinitis with Eosinophilia Syndrome and Related Disorders, 2007].
Drug-induced rhinitis, including rhinitis medicamentosa. Rebound congestion from overused topical decongestant sprays is the classic example. Prognosis here is among the most favorable of the group: it is largely reversible once the offending agent is stopped, though the rebound period can be uncomfortable. Other systemic medications (certain antihypertensives, for instance) can produce a similar picture that improves when the drug is adjusted.
Hormonal rhinitis, including rhinitis of pregnancy. Driven by endogenous hormonal shifts. Pregnancy (gestational) rhinitis is notably self-limiting, characteristically resolving completely within about two weeks of delivery, which makes conservative management the sensible default during pregnancy [Caparroz, Rhinitis and Pregnancy: Literature Review, 2016].
Atrophic rhinitis. Marked by mucosal atrophy and, in advanced forms, crusting and a paradoxical sense of congestion in a wide nasal cavity. This subtype tends toward a chronic, less reversible course and often needs ongoing nasal care rather than a short treatment course.
Gustatory rhinitis. A watery runny nose triggered by eating, especially hot or spicy food. It is benign and localized, and many patients manage well by anticipating the trigger or using a targeted nasal medication before meals.
| NAR subtype | Share / frequency | Typical course |
|---|---|---|
| Vasomotor (idiopathic) | ~80% of NAR | Chronic, relapsing-remitting; controllable, not usually curable |
| NARES (eosinophilic) | Less common | Persistent; risk factor for polyps, aspirin sensitivity, OSA |
| Rhinitis medicamentosa | Common, iatrogenic | Largely reversible after stopping the spray |
| Hormonal / pregnancy | Common in pregnancy | Pregnancy form resolves within ~2 weeks of delivery |
| Atrophic | Uncommon | Chronic, often less reversible |
| Gustatory | Common, food-linked | Benign, localized, manageable |
Treatment Guidelines at a Glance
Allergic rhinitis (ARIA-EAACI 2024–2025)
The Allergic Rhinitis and Its Impact on Asthma (ARIA) guidelines were revised in 2024–2025 using the GRADE framework, and the directionality of several recommendations changed from earlier versions. For intranasal therapy, the panel favored a fixed combination of an intranasal antihistamine plus an intranasal corticosteroid (INAH + INCS) over either component alone, and favored intranasal corticosteroids over intranasal antihistamines when choosing a single agent [Sousa-Pinto, Allergic Rhinitis and Its Impact on Asthma (ARIA)-EAACI Guidelines-2024-2025 Revision: Part I-Guidelines on Intranasal Treatments, 2025].
For oral and ocular options, the companion document favored intranasal corticosteroids over oral antihistamines, oral antihistamines over leukotriene receptor antagonists (LTRA), and oral antihistamines over ocular antihistamines; it suggested against adding an LTRA on top of an oral antihistamine [Vieira, Allergic Rhinitis and Its Impact on Asthma (ARIA)-EAACI Guidelines-2024-2025 Revision: Part II-Guidelines on Oral and Ocular Treatments, 2026]. Taken together, the intranasal corticosteroid (alone or paired with an intranasal antihistamine) sits at the center of modern AR pharmacotherapy. Allergen avoidance and, for selected patients with persistent or insufficiently controlled disease, allergen immunotherapy round out the approach.
Nonallergic rhinitis
NAR is less tidily standardized than AR, and treatment is matched to the dominant symptom and subtype rather than a single algorithm. The practical first line combines trigger avoidance with topical therapy — an intranasal corticosteroid and/or an intranasal antihistamine, with azelastine being the commonly cited intranasal antihistamine because it has activity in nonallergic disease [Baroody, Nonallergic Rhinopathy: A Comprehensive Review of Classification, Diagnosis, and Treatment, 2024].
From there, treatment follows the phenotype. A runny-nose-predominant patient often benefits from intranasal ipratropium, an anticholinergic that targets watery rhinorrhea. Decongestants may give short-term relief for congestion but must not be used long-term, since chronic use is exactly what causes rhinitis medicamentosa. Refractory cases warrant specialist referral for additional options, including procedures aimed at the nerves driving the hyper-reactive nose.
One practical point deserves emphasis: oral antihistamines and leukotriene antagonists, the familiar workhorses of allergic rhinitis, are generally less effective in nonallergic disease. Assuming “rhinitis is rhinitis” and reaching for the same oral allergy pills is a common reason nonallergic patients feel their treatment is failing.
Clinical Perspective The most useful question is rarely “is this allergic or not?” but “how much of this is allergic, and what else is going on?” A patient with documented dust-mite allergy who still reacts to cold air, cooking smells, and a glass of wine has a neurogenic, nonallergic component layered on top of the allergy. Treating only the allergy in that situation predictably underdelivers. Naming the nonallergic part — and choosing tools such as an intranasal antihistamine or ipratropium that act on it — is often what finally improves control.
Key Takeaways
- Allergic and nonallergic rhinitis share symptoms but differ in mechanism, course, and treatment; history and examination separate most cases, with allergy testing reserved for ambiguous ones.
- Nonallergic rhinitis is a diagnosis of exclusion, and a negative allergy test does not always rule out a localized allergic process.
- Vasomotor (idiopathic) rhinitis is the most common nonallergic subtype at about 80% of cases and is typically controllable rather than curable.
- Prognosis varies sharply by subtype: rhinitis medicamentosa and pregnancy rhinitis are largely reversible, while atrophic rhinitis and NARES tend to be chronic and warrant closer follow-up.
- ARIA 2024–2025 places intranasal corticosteroids — alone or combined with an intranasal antihistamine — at the core of allergic rhinitis care, whereas nonallergic rhinitis relies more on trigger avoidance, intranasal antihistamines or corticosteroids, and ipratropium for runny-nose-predominant disease.
FAQ
How do I know if my rhinitis is allergic or not? The strongest clues come from your history, not a single test. Allergic rhinitis tends to be seasonal or triggered by pollen, dust, or pets, with sneezing, nasal and eye itching, and often a family history of allergy. Nonallergic rhinitis usually starts later in life, lacks prominent itching, and flares with irritants like smells, smoke, temperature changes, or alcohol. Allergy testing helps confirm the answer when the pattern is unclear.
Does nonallergic rhinitis ever go away? It depends entirely on the subtype. Rebound congestion from overused decongestant sprays and pregnancy-related rhinitis are largely reversible once the spray is stopped or the pregnancy ends. Vasomotor and atrophic forms tend to be chronic, where the realistic aim is good long-term control rather than a permanent cure.
Can you have both allergic and nonallergic rhinitis at the same time? Yes, and it is common — this overlap is called mixed rhinitis. Many patients carry both an IgE-mediated allergy and a nonallergic, irritant-driven component, which is why someone with a confirmed allergy may still react to perfume or cold air outside of allergy season. Recognizing both parts is key to treating the whole problem.
References
- Quillen DM, Feller DB. Diagnosing rhinitis: allergic vs. nonallergic. Am Fam Physician. 2006;73(9):1583-90.
- Topal E, Bakirtas A, Yilmaz O, Ertoy Karagol IH, Arslan U, Arga M, Demirsoy MS, Turktas I. Predictive factors to differentiate between allergic and nonallergic rhinitis in children. Int Forum Allergy Rhinol. 2014;4(6):447-52.
- Baroody FM, Gevaert P, Smith PK, Ziaie N, Bernstein JA. Nonallergic rhinopathy: a comprehensive review of classification, diagnosis, and treatment. J Allergy Clin Immunol Pract. 2024;12(6):1436-1447.
- Sousa-Pinto B, Bousquet J, Vieira RJ, et al. Allergic Rhinitis and Its Impact on Asthma (ARIA)-EAACI guidelines-2024-2025 revision: part I-guidelines on intranasal treatments. Allergy. 2025;81(4):954-976.
- Vieira RJ, Sousa-Pinto B, Bousquet J, et al. Allergic Rhinitis and Its Impact on Asthma (ARIA)-EAACI guidelines-2024-2025 revision: part II-guidelines on oral and ocular treatments. Allergy. 2026;81(6):1947-1970.
- Settipane RA, Charnock DR. Epidemiology of rhinitis: allergic and nonallergic. Clin Allergy Immunol. 2007;19:23-34.
- Ellis AK, Keith PK. Nonallergic rhinitis with eosinophilia syndrome and related disorders. Clin Allergy Immunol. 2007;19:87-100.
- Caparroz FA, Gregorio LL, Bongiovanni G, Izu SC, Kosugi EM. Rhinitis and pregnancy: literature review. Braz J Otorhinolaryngol. 2016;82(1):105-11.
Joonpyo Hong, MD is a board-certified otolaryngologist practicing in Korea. This article reflects his clinical interpretation of published research and does not constitute individual medical advice.
For more interesting contents:
https://curiousmd.com/evolutionary-reason-for-allergies/
https://curiousmd.com/korea-2026-pollen-allergies/
https://curiousmd.com/ai-allergy-forecast-personalized-prediction/
Link out to: